
Abstract
Abstract
Objective:
This study identified birth events and infant/maternal factors related to breastmilk sodium (Na+) among primiparous mothers.
Subjects and
Results:
Presence of gestational diabetes increases the risk of an elevated breastmilk Na+ level at 48 hours, and increased number of breastfeeds (mean=8.91, SD=3.77) lowers it, indicating lactogenesis II was initiated.
Conclusions:
Breastfeeding frequency impacts initiation of lactogenesis II, which in turn influences duration of breastfeeding exclusivity. Therefore feedings should be promoted as soon as possible after birth and as frequently as eight to 12 times a day.
Introduction
LS- II starts around 30–40 hours after birth of a term infant and is first characterized by changes in breastmilk components, followed by milk onset—an increase in the amount of milk secreted, which corresponds to a maternal perception of fuller breasts. 2 Breastmilk changes, in particular, a decrease in breastmilk sodium (Na+) and an increase in lactose, 6 correspond to decreased lactocytes cellular permeability 6 and closure of tight junctions. 7
The prevalence of delayed LS-II varies in between 11% to 44%,3,8,9 with primiparity being the strongest risk factor. Several factors with mixed evidence have been associated with delayed LS- II: cesarean section, emergency cesarean section, prolonged labor stage II, stress, maternal age, diabetes, obesity, ineffective breastfeeding, and preonset supplementation.9–18 The goal of this study was to determine the influence of birth events and maternal/infant factors on LS-II marker breastmilk Na+ among primiparous breastfeeding mothers.
Subjects and Methods
The data were collected as part of a larger study on perceived insufficient milk. The convenience sample was recruited between July 2009 and June 2010 from two mother–baby units at a Canadian university maternal care center, which averages 3,200 births annually. Inclusion criteria were (1) first-time breastfeeding mothers ≥18 years old, (2) birth of an infant at ≥37 weeks of gestation and with a birth weight of ≥2,500 g, (3) French and/or English language spoken and written, and (4) a phone number for the 6-week postnatal follow-up. Mother–infant separation of >24 hours was the exclusion criterion.
In total, 410 mothers were eligible, but 36.6% (150) refused to participate because of lack of time, fatigue, or enrollment in another study. Of the remaining 260 mothers, eight were excluded because of incomplete consent forms. The final sample included 252 mothers, of whom 60% (151/252) provided breastmilk samples, 79.7% returned the Week 2 questionnaire (201/252), and 84.9% were reached by phone at 6 weeks postpartum (214/252).
The mean maternal age was 29.5 years (SD=4.9 years) (range, 18-42 years). In total, 91% were married or lived with a spouse, and almost 60% were university graduates. Most women were working or studying full-time. Almost 25% reported a family annual income of ≤35,000 CDN$, and almost half reported ≥75,000 CDN$ annually. Among the group, 63% were North American. and 79% spoke French at home.
Procedure
The ethics review committee of the hospital approved the study. Each day the researcher consulted the units' assistant head nurse about new deliveries in the past 24 hours and their eligibility for participation in the study. A nurse then asked eligible mothers if they were interested in participating. If they agreed, the researcher met the mothers to explain the study and obtain informed consent. On Day 3, with Day 1 being the delivery day, mothers completed a questionnaire described below. They were encouraged to hand-express 0.5 mL of milk from each breast. The same questionnaire was then mailed to them at postnatal Week 2, and at postnatal Week 6 a phone call was made by a lactation consultant to ask about breastfeeding practices and offer guidance as needed.
Measures
Birth events
Type of delivery was categorized as vaginal, operative vaginal (e.g., forceps), elective cesarean (planned during pregnancy), or nonelective cesarean (emergency) in the Day 3 questionnaire.
Data collected through chart review by the first researcher included total duration of labor, length of first stage and second stage, use of oxytocin stimulation/induction, anesthesia/analgesia methods, Apgar score at 1 minute and 5 minutes, skin-to-skin contact after birth, and first hour breastfeeding.
Infant factors
Infant factors included in Day 3 and postnatal Week 2 questionnaires were as follows:
1. Infant Breastfeeding Assessment Tool.
19
The Infant Breastfeeding Assessment Tool measures infant breastfeeding behavior at the last feeding and includes four items: readiness to feed, rooting reflex, latch-on, and suckling. Each item has a possible score of 0 to 3. A score of ≥10 indicates optimal breastfeeding behavior. Inter-rater reliability index of 91% between mothers and professionals' ratings has been reported.
19
This instrument was used to predict breastfeeding cessation in the first 2 weeks postnatally.
19
Cronbach's α was 0.71 for this study. 2. Breastfeeding frequency, measured according to the number of times the mother breastfed her infant in the last 24 hours. 3. Irritability at the breast, subscale of the Mother and Baby Scale.
20
This measures infant temperament at the breast. It contains eight items answered on a one-dimensional scale from “never apply” (=0) to “very/often apply” (=5). Higher scores mean a more irritable infant at the breast. Internal consistency reliability reported is 0.86.
20
Irritability of the infant at the breast has been negatively associated with breastfeeding behaviors at 6 weeks.
21
Cronbach's α was 0.85 for this study.
Infant data collected through chart review included sex, gestational age, birth weight, and percentage weight loss on Day 3.
Maternal factors
Maternal data collected through chart review included maternal diseases, medications, breast surgery, prepregnancy weight, and height.
Breastmilk Na+ was assessed after helping mothers hand-express 0.5 mL of milk from each breast in clean propylene containers. Samples were frozen immediately and then thawed before analysis. Thawed samples were centrifuged for 15 minutes at 4°C in a Micromax RF IEC machine to ensure that the lipid portion of breastmilk was separated. This was to avoid a false reading of decreased Na+. 22 Samples were then analyzed using a gasometry apparatus. The mean from the right and left breasts was used for data analysis.
Supplemental feed frequency and reasons for their administration were self-reported by the mother in the Day 3 questionnaire.
At postnatal Weeks 2 and 6, mothers were asked whether their breastfeeding practices were exclusively breastmilk (no other type of feed including water), predominantly breastmilk (which includes one or two feeds other than breastmilk), partial (three or more feeds other than breastmilk), and no breastmilk.
Data analysis
Data were entered and analyzed using SPSS version 18.0. Descriptive statistical analyses were done. The relationships among the breastmilk Na+ outcome, birth, maternal/infant factors, and breastfeeding practices were analyzed. Pearson correlations were used to assess continuous variables. Student's t test analysis was used to assess categorical variables. Analysis of variance was used for categorical variables with multiple comparisons. Variables found significantly related to breastmilk Na+ were then entered in multivariate analyses using regression. Data collected through chart review on oxytocin use during labor, prepregnancy weight, height, skin-to-skin contact, and breastfeeding in the first hour after birth were not entered in the analyses because data were incomplete and therefore could skew the results.
Results
Breastmilk Na+
The mean breastmilk Na+ was 42.73 mmol/L (SD=22.12 mmol/L; range, 14.50–120.00 mmol/L).
As shown in Table 1, factors related to breastmilk Na+ were maternal age, gestational diabetes, insulin use, ethnicity, and breastfeeding frequency. All other measures of birth events and infant and maternal factors were found not related to breastmilk Na+. The relation between breastfeeding frequency and breastmilk Na+ was further explored using categories of 0–4, 5–6, 7–8, 9–10, and ≥11 breastfeeds in 24 hours. The differences in the mean breastmilk Na+ were found to be significant (Table 1), and the relation was linear (Fig. 1).
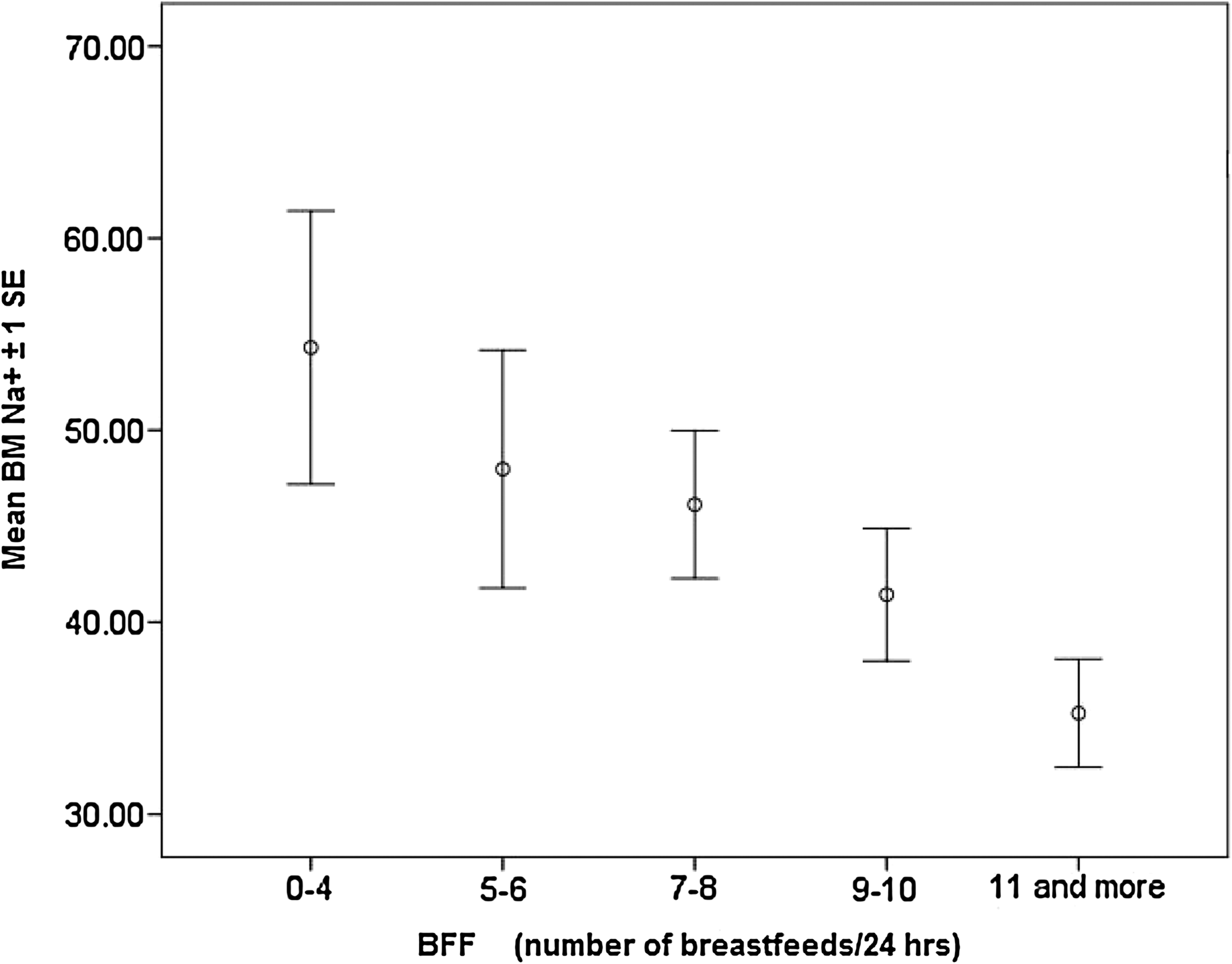
Graphical representation of the linear relation between mean breastmilk (BM) Na+ and number of breastfeeds at Day 3 (approximately 48 hours). BFF, breastfeeding frequency.
p<0.05, **p<0.01.
Post hoc Tukey's test was done; no breastfeed category was found to be significant.
Post hoc Tukey's test was done; no ethnic group was found to be significant.
Regression analysis (Table 2) showed that presence of gestational diabetes increased the risk of an elevated breastmilk Na+ [β=0.319, t(131)=3.27, p<0.01] and that a higher breastfeeding frequncy was associated with a lower breastmilk Na+ [β=–0.20, t(131)=–2.09, p<.05].
R2=0.142.
p<0.01.
Breastmilk Na+ was related to breastfeeding practices at both Weeks 2 [t(121)=3.46, p<0.001] and 6 [t(132)=2.29, p<0.01]. The most frequent reported reason for stopping breastfeeding or introducing supplemental feeds was insufficient breastmilk.
Discussion
The mean breastmilk Na+ was similar to some published results 23 and higher than others.7,18,24 No single measure could confirm that LS-II was initiated, 22 although cutoffs in the range of 3–18 mmol/L have been proposed after Day 3. 25 For some primipara, an expected decline in breastmilk Na+ was observed, indicating that LS-II was initiated. 26 As the number of breastfeeds increased, the decline in breastmilk Na+ was greater.
Mixed evidence is reported on the necessity of milk removal in the first few days after birth for LS-II to be initiated. 7 It has been suggested that milk removal is not necessary for the establishment of LS-II because in both breastfeeding and non-breastfeeding mothers, the changes in biological markers associated with LS-II are similar. 27 Some authors hypothesized that milk expression by itself in non-breastfeeding mothers contributed to initiate LS-II because potential inhibitory local factors were removed. 7 However, for some mothers in our primiparous sample, frequent milk removal was necessary to obtain junctional closure. 7 To our knowledge, this is the first study to document the relationship between breastfeeding frequency and breastmilk Na+. Although relation does not mean causation, 28 this result adds evidence to the presence of inhibitory local factors in early breastmilk hypothesis and the necessity of frequent milk removal in order to prevent their inhibitory effect on LS-II initiation. 7
Breastmilk Na+ on Day 3 was associated with breastfeeding practices at postnatal Weeks 2 and 6, confirming previous results. 29 The lowest breastmilk Na+ was on Day 3, meaning that LS-II is initiated and the more a mother breastfeeds exclusively at postnatal Weeks 2 and 6. It is then plausible to believe that mothers who reported insufficient breastmilk as a reason for stopping breastfeeding or introducing supplemental feeds may have presented postglandular insufficiency defined as any interference with frequent and effective mammary gland stimulation. 7 Even though the measurement of Na+ as a marker of LS-II is precluded from the clinical practice, its significance is of importance for healthcare professionals.
Limitations
There are a few limitations to this study. First, it is a convenience sample; therefore self-selection might have occurred. Second, the breastfeeding assessment measures were self-administered, obviously subjective in nature. Not all mothers provided breastmilk samples, and these missing data might not have been random. Reasons given by mothers for not providing samples were not enough milk so that they wanted to keep it for their baby and not being able to hand express. Therefore, mothers with a successful breastfeeding experience might have been overrepresented.
Conclusions
In this sample of primiparous breastfeeding mothers, a higher number of feedings was associated with a lowered breastmilk Na+, the biological marker of LS-II, which was associated with duration of exclusive breastfeeding. Therefore interventions should be directed toward promoting early frequent feedings of at least eight to 12 in 24 hours as previously recommended. 30 Promotion of hand expression at the beginning or between feedings may ensure additional stimulation in at-risk groups such as primiparous mothers with lactation difficulties. Maternal medical conditions such as gestational diabetes and its impact on LS-II initiation deserve further investigations.
Footnotes
Acknowledgments
We want to thank all mothers who participated in this study. Thanks also to the nursing staff for their precious collaboration. Thanks to Diane Gagnière and Solange Poulard, lactation consultants, who did the 6-week phone calls and counseling as needed. Thanks to Dr. Monique Nuyt and laboratory staff who generously gave access to apparatus for breastmilk sample preparation and analyses. Thanks to Kate Johnson who edited this article. This study was funded by the Quebec Interuniversity Nursing Intervention Research Group, Canadian Nurse Foundation.
Disclosure Statement
No competing financial interests exist.