
Abstract
Background:
Autistic adults have a high incidence of mental health challenges, including suicidal thoughts and behavior (STB). Our objective was to gain a nuanced understanding of autistic adults’ experiences in seeking and receiving support for their mental health, including STB, presented in a format that could be operationalized to improve service provision for autistic adults.
Methods:
We applied an integrated codesign approach involving autistic adults at every stage of the research, acknowledging them as experts on their own lives. Thirty-three autistic adults with a history of STB participated in semi-structured narrative interviews, discussing their experiences seeking and receiving support for their mental health. We analyzed data using reflexive thematic analysis.
Results:
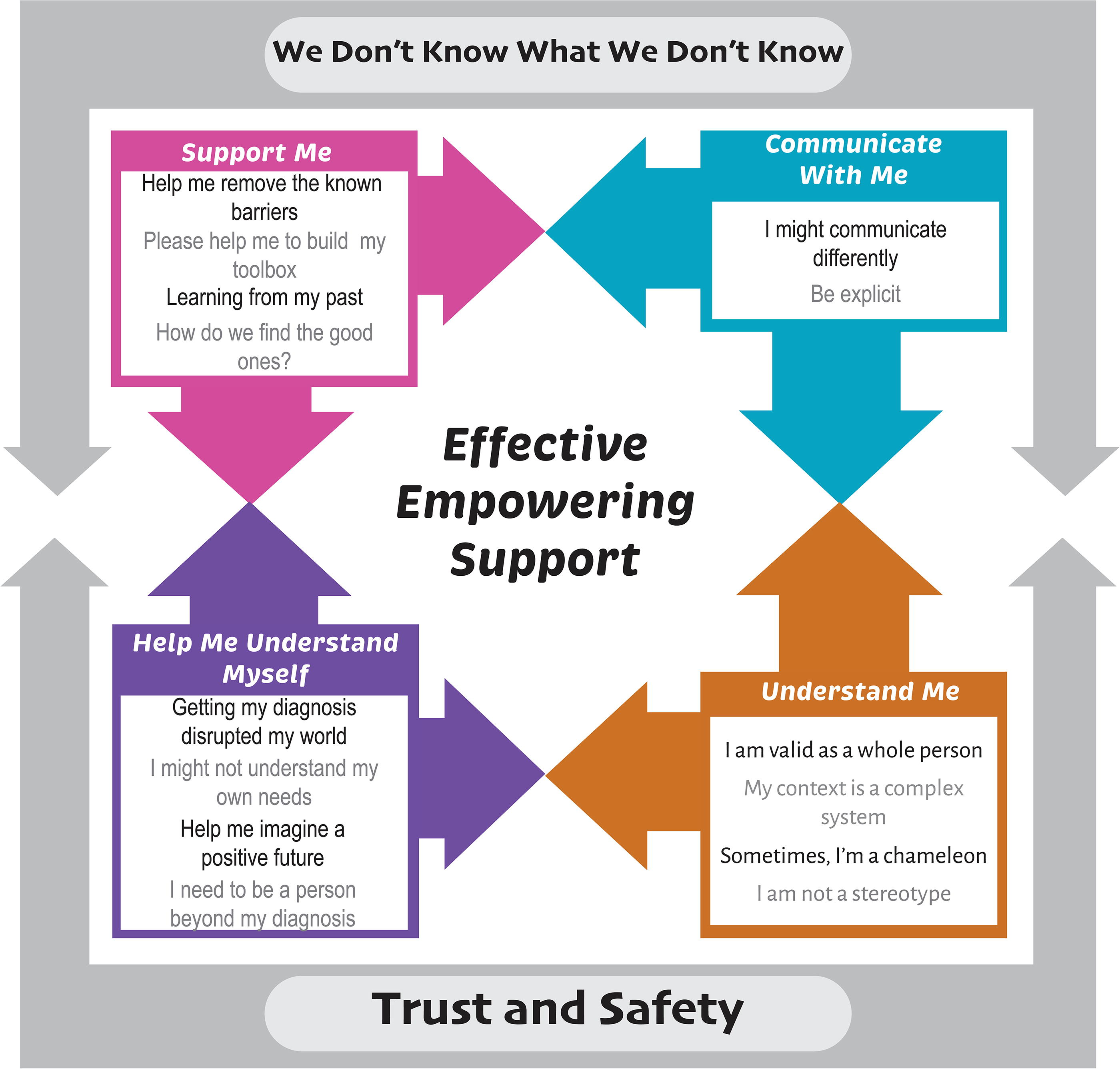
We constructed an overarching theme, “We Don’t Know What We Don’t Know,” representing the bidirectional misunderstandings that occur between health care providers and autistic people. Within the overarching theme were four central themes: (1) Communicate with Me (understanding the uniqueness of autistic communication); (2) Understand Me (developing a nuanced understanding of autism and being autistic); (3) Help Me to Understand Myself (developing self-understanding); and (4) Support Me (empowerment when supported). We constructed an underpinning theme, “Trust and Safety,” representing the need for psychological safety in all domains of mental health care. We centered the lived experiences of autistic adults to acknowledge the need for autistic people to feel safe and for service providers to build trust to effectively support the mental health of autistic adults.
Conclusions:
Our analysis demonstrates the need to facilitate access to mental health care and improve the quality and effectiveness of service utilization for autistic adults. Recommendations include improving understanding of and communication with autistic people, embedding education, cultural humility, and psychological safety, acknowledging power imbalances, adapting interventions, and validating autistic experience. Our thematic map serves as a framework to inform and improve health care services for autistic people.
Community Brief
Why is this an important issue?
Autistic adults often experience great difficulty accessing services for their mental health. They may also not benefit from health care services as much as nonautistic people if the services are not suited to their needs. This is important because autistic adults can experience more mental health challenges than nonautistic people. Compared with the general population, autistic adults also experience more suicidal thoughts and behavior. This includes higher rates of suicide death. Improving mental health services for autistic adults may improve their quality of life and prevent suicide.
What was the purpose of this study?
We wanted to understand the experiences of autistic adults when they looked for support for their mental health, including experiences of suicidal thoughts and behavior. We wanted to find out how to improve support for autistic adults with mental health challenges.
What did the researchers do?
We asked 33 autistic adults who had previously experienced suicidal thoughts or behavior about their experiences seeking support for their mental health. We asked them who they reached out to for support, what the experience was like, and what could be improved. An autistic researcher analyzed these conversations to identify common themes between the research participants. We looked for problems with health care services that might make it difficult for autistic adults with mental health challenges to access and receive appropriate support.
What were the results of the study?
We found that challenges accessing health care services included: (1) communication between autistic adults and service providers, (2) (mis)understanding of autism and autistic people, (3) difficulties autistic adults experience in understanding themselves and their support needs, and (4) finding appropriate services and supports. We found that misunderstanding between autistic adults and health care service providers was common, and that autistic people may not feel safe when using mental health care services. This made it very difficult for autistic adults to receive the support they needed for their mental health.
What do these findings add to what was already known?
Our findings build on previous research through our development of a new framework. This framework can be used to identify gaps between what is provided by health care services and the unmet needs of autistic adults. We suggest that health care providers can use this framework to critically assess their service offerings from the perspective of people with lived experience.
What are potential weaknesses in the study?
We excluded autistic adults with intellectual disability and complex communication needs from our study. Our results might not apply to autistic people who have those challenges. We also excluded self-identified autistic adults, even though this group also experiences more mental health challenges than nonautistic people.
How will these findings help autistic adults now or in the future?
Our findings can be used to help health care service providers to better understand and meet the needs of autistic adults.
Introduction
Autistic adults are at increased risk of co-occurring mental health conditions, which, in turn, increase risk for suicidal thoughts and behavior (STB).1–4 There is strong evidence that suicide risk is significantly elevated in autistic people compared with the general population; risk of premature death by suicide is about 3-fold that of the non-autistic population and 5-fold when considering only individuals without intellectual disability.5–7 Autistic people may experience additional, more severe, and sometimes unique (e.g., fear of the unknown, loss of control, and overstimulation) sources of distress compared with other populations, increasing the likelihood that an individual may progress from suicidal ideation to a suicide attempt.8–11 The interaction between stressors, psychopathology, and suicide rates may be most salient in those individuals with co-occurring mood or other mental health conditions. 12 The autistic population has identified access to appropriate and effective mental health services as a research priority. 13
Autistic people face barriers to service access and utilization.14–16 This includes limited understanding of autism and the needs and experiences of autistic adults; systems that fail to accommodate autistic thinking styles, sensory needs, and communication preferences; and therapeutic approaches that have not been developed with or for autistic people.14–16 Difficulty accessing appropriate mental health care can increase isolation, stigmatization, and suicidal ideation. 14 Moreover, health care comes at considerable economic cost to individuals and society. 17 Services therefore need to be designed, accessed, and delivered in ways that maximize effectiveness for the population they are intended for.
Current study
Although a limited body of research has explored autistic people’s challenges accessing health care services (for a summary of previous research findings, see Supplementary Table S1),14–16,18 the experiences of autistic adults seeking mental health support in Australia remains underexplored. Furthermore, no research has specifically focused on the experiences of autistic adults who had a history of STB. Therefore, in this qualitative study we interviewed autistic about their experiences seeking and receiving support for their mental health. We recruited participants who had lived experience of STB. We aimed to develop knowledge that could inform services on adapting their current provision to better meet the needs of autistic clients, ultimately improving access to health care. We joined with people with lived experience in the research process (e.g., inviting autistic people to help generate research questions). Our research was guided by the following questions:
What are the experiences of autistic adults seeking and receiving support for their mental health, including STB? What are the barriers to access and effective utilization of mental health care services? What factors are associated with successful navigation of services and processes? How can these insights inform service design and provision to remove obstacles and facilitate improved service access and utilization?
Methodology
Participants
A total of 33 autistic adults (16 women, 14 men, and 3 non-binary; Mage = 41.72, standard deviation [SD] = 11.49 years, range = 21–68) without co-occurring intellectual disability participated in the study. Participants were required to be able to communicate in verbal or written English, be aged 18 years or older, and have received a diagnosis of autism from a qualified health professional. We recruited participants with a history of one or more suicidal attempts (i.e., a potentially self-injurious act committed with a wish to die, as a result of the act; n = 20), interrupted attempts (i.e., interrupted by an outside circumstance from starting the potentially self-injurious act if not for that, an actual attempt would have occurred; n = 1), or suicidal ideation (i.e., thoughts about a wish to be dead or not alive anymore, or wish to fall asleep and not wake up; n = 12), assessed with the Columbia-Suicide Severity Rating Scale (C-SSRS). 19
Most participants were born in Australia (n = 23) and spoke English at home (n = 29). Primary diagnoses included autism spectrum disorder (n = 17) or Asperger’s syndrome (n = 16). Co-occurring diagnoses included anxiety and depression (both n = 23) and attention deficit hyperactivity disorder (n = 10); no participants reported intellectual disability. Participants were highly educated overall (e.g., bachelor’s degree, n = 14; master’s degree, n = 8; PhD, n = 3), were in a relationship (n = 21), and lived with a spouse, partner (n = 17) or family member (n = 6).
Dataset generation
The study was approved by La Trobe University Human Research Ethics Committee (HEC20235). The study was advertised in a newsletter sent to participants from one of two longitudinal autism studies.20,21 The first stage of the research consisted of a quantitative study, which included assessment with the C-SSRS. Following review of C-SSRS responses to determine eligibility (i.e., history of STB), we invited participants into the qualitative study. Forty-three participants reported a suicide attempt and 15 reported other suicidal behavior (e.g., interrupted attempt) or suicidal ideation on the C-SSRS, resulting in a possible pool of 58 participants. To balance having a sample sufficiently large and diverse to generate meaningful data with ethical considerations (i.e., not subjecting participants to unnecessary data collection), we initially capped our recruitment target to 40 participants. We then invited participants via email beginning with those with history of a suicide attempt, to those reporting suicidal ideation on the C-SSRS, until we reached 40 participants or exhausted the participant pool (n = 33). Online interviews (i.e., Zoom video call, n = 32, Zoom chat, n = 1) were scheduled for a maximum of 60 minutes each (M = 47, SD = 10 minutes, range = 22–67).
We managed elevated risk of distress or suicide according to our study protocol, which included a detailed risk assessment procedure.12,22 We provided all participants with links to mental health care resources; a team psychologist followed up any participants reporting suicidal ideation or behavior. Recruitment and interviews were conducted in 2021, participants were reimbursed with a voucher (AUD $45).
Codesign statement
Following participatory research guidelines, we involved the community in the research process. 23 We identified and invited community members from diverse backgrounds, with the aim of being guided by their expertise and lived experience. Autistic and nonautistic researchers collaborated with community members (see Table 1) in the design, development, and implementation phases. 24 We met regularly with community members to discuss the study, identify research priorities, and to inform the interview questions. Specifically, we invited community members (n = 26) and research participants from the broader study (n = 15) to contribute questions, suggestions, and ideas that would improve our understanding of the mental health and suicide prevention support needs within the autistic community; we incorporated their responses and suggestions into the interview guide (see Supplementary Data).
Public Involvement in Research (Primary Identity)
Data analysis
The first author (JW) analyzed the open-ended narrative survey responses using reflexive thematic analysis, applying Braun and Clarke’s Quality Assessment Framework to ensure conformity to our analysis plan.25–29 The first author reviewed interview transcripts to gain an overall sense of each participant’s experiences, making written reflections after each reading and detailing impressions and thoughts regarding the narrative, prior to manually coding data for semantic codes (e.g., “autism is an integral part of my mental health”) and latent meaning (e.g., “pathologization of difference”). This was an iterative process, during which the first author read and reread the transcripts to build patterns of shared meaning, in an “artfully interpretive” approach, acknowledging and embracing researcher subjectivity and encouraging deep and considered engagement with the data.28,30 While semantic coding formed many of the building blocks of meaning, the resultant themes and subthemes represent latent interpretation of meaning through the lens of the first author’s lived experience as an autistic adult. Specific details on approach, phases of analysis, and iteration of codes, themes and subthemes, as well as researcher positionality, are provided in the Supplementary Data.
Analysis
Participants discussed their experiences accessing and utilizing both formal and informal supports for their mental health generally, and during specific periods of mental illness, inclusive of STB. We also asked participants how services could be improved. We mapped the resulting themes and associated subthemes; each of which we considered integral to the experiences of study participants (see Fig. 1 and Table 2; also see Supplementary Table S4 for additional detail concerning theme conceptualization). Constructed themes and subthemes varied in terms of breadth of data synthesized; thus, the amount of space dedicated to each theme reflects heterogeneity in the amount of data generated.
Figure 1 represents the complexity and interconnectedness of participants’ experiences in their support journey. While we initially discussed various forms of support as static loci visited by participants at a point in time, supports were fluid and interconnected, where an experience with one support impacted on the experience with the next. Thus, support seeking was iterative at all stages from mental health to mental ill-health, and back again. Participants described ongoing support-seeking, including during periods of STB. We drew on these iterative, interconnected descriptions of participant experiences and conceptualized the thematic map as interconnected with each domain influencing the others. Underpinning the diagram, and participant narratives, is the idea that feelings of trust and safety are necessary for successful navigation and support-seeking. At the top of the diagram the overarching theme: “We don’t know what we don’t know” acknowledges the potential for misunderstandings and reminds us of the need for cultural humility in support relationships. These overarching and underpinning themes bracket four central themes: “Communicate with Me,” “Understand Me,” “Help Me Understand Myself,” and “Support Me.” These themes are bidirectionally interconnected (represented by the arrows in Fig. 1). The central text in the diagram, “Effective, Empowering Support,” is representative of the contribution of positive support to well-being. To increase accessibility, we included a thematic table of Figure 1 (see Table 2).
Overarching theme: We don’t know what we don’t know
This theme represents the idea that autistic people and mental health care providers often misunderstand each other.
Autistic people commonly report negative experiences in the mental health care system, both in the current study (e.g., “I think, because they’re not looking through an autism-informed lens … that tends to make you feel a bit othered, alienated, dysfunctional”; P006), and in broader literature.14–16,18,31,32 Realizing that we do not know something requires humility, may spark curiosity, and may inspire inquiry or research on a topic. However, when we don’t know what we don’t know, we may be unaware of the existence of pertinent information or may consider our knowledge of the topic sufficiently comprehensive or complete. 33 This can present a barrier to understanding, failure to notice or accept new or contrary information, or to consider alternative perspectives. Not knowing that we don’t know, and acting on that (lack of) knowledge, may lead to harm via acts of omission or commission.34–36 These acts of harm may be both unintentional and unnoticed by the perpetrator, leading the victim of harm to feel invalidated and unseen, and further perpetuating the divide of “we don’t know what we don’t know.”33,37,38
Participants expressed frustration with health care providers who seemed to misunderstand their needs: “[The doctor] said [you don't look autistic] within three minutes of me walking in the door” (P007). They shared stories of health care providers becoming frustrated, and even angry if they misinterpreted information and instructions: “I had a GP [general practitioner] yell at me, because I had only been communicating with a psychologist by email, and that psychologist had stopped replying to my emails” (P016). In many of these narratives, we identified potential mutual misunderstandings, influenced by differences in communication, lack of understanding of autistic people by health care providers, lack of understanding about autism and themselves by autistic people, and support practices and structures that were invalidating, inaccessible or ineffective for autistic individuals.
[It’s like] how cultural difference between two different people hinders communication. So, if I’m from somewhere and you’re from somewhere else, and I do something that’s supposed to mean something physically or in the way that I say it, and it’s got all the good intentions that are supposed to make you feel comfortable, but for you—you’re unfamiliar with this, so it just goes over your head, you know? So, there’s been miscommunication there, because of our different experiences in our lives. (P016)
Theme 1: Communicate with me
This theme represents how autistic people may need health care providers to adapt their communication methods and styles to better match communication preferences and needs:
[Because I’m autistic] I feel like less effort is made to understand me as a patient. [I’m] just not getting the impression that they trust that I’m doing my best to communicate. (P001)
Given the need for adaptation (i.e., more effort), this statement indicates that less effort was offered by the provider to understand and support the autistic person; the exact opposite of what is needed was provided. Communication difficulties and misunderstandings were a common element of many participants’ narratives when describing their attempts to access and utilize health care supports. As such, two discrete subthemes were constructed: “Be Explicit” and “I Might Communicate Differently.”
Be Explicit
This subtheme identifies the need for health care providers to give clear, detailed explanations of their processes and what to expect, helping autistic people better understand and access services.
Participants suggested that this can be enacted both by direct communication, without the use of vague metaphor and hidden meaning, and by providing sufficiently detailed information to minimize ambiguity about expectations, procedures, and requirements. Participants expressed relief when provided with explicit, detailed communication: “It takes a lot of the mental load off me, because I don’t have to make all the social decisions on the fly, because I know what they are, because I know what I’m supposed to be doing” (P016).
Thematic map.
Thematic Table
I Might Communicate Differently
This subtheme represents participants’ views of autistic communication as a unique way of engaging with the world.
Autistic communication may reflect a different and unique communication style compared to nonautistic communication.39–41 Participants shared many experiences involving miscommunication and misunderstanding when attempting to access health care services, reflecting systemic communication barriers. It is notable that persistent challenges in social communication and interaction is one of the diagnostic criteria for autism, yet in the participant narratives, it appeared that very little effort was made by health care providers to accommodate or understand these challenges (e.g., communication factors leading to difficulties making appointments). 42 Difficulties in executive function, such as remembering during business hours to make the appointment and difficulties with multistep processes, were common factors, as was uncertainty around social rules (e.g., how long one should wait for a promised call back before following up). In addition, many participants expressed a dislike of telephone calls. Participants described how health care providers failed to accommodate these needs:
[The GP] yelled at me, because I hadn’t called the psych[ologist], and that was obviously the most sensible thing to do. I don’t call anybody. I don’t want to call anybody. Unless it’s like an absolute [expletive] emergency. (P016)
Participants indicated a need for improving awareness of and willingness to accommodate their communication needs (e.g., patience and time to ensure understanding):
I’m quite emotional, which is something that’s improved a bit as I’ve aged, but [I need providers] who won’t get angry at me if I’m going slowly or getting emotional. (P001)
Theme 2: Understand me
Universally identified in the narrative of every participant in this study, this theme is demonstrative of health care providers’ limited understanding of autistic experiences, culture, and needs, negatively impacting the therapeutic relationship:
I’ve had [health care professionals] say to me that I don’t seem to be autistic … Which immediately makes me realize that they're probably not the people that I want to be forming a therapeutic relationship with. (P013)
Four subthemes were constructed under “Understand Me.”
I Am Valid as a Whole Person
This subtheme represents the need for health care providers to recognize that each person’s unique identity and experiences are essential parts of their whole self.
Study participants identified factors ranging from unhelpful to potentially harmful when interacting with health care services. “Pathologization of difference” was reported to be widespread and problematic, particularly when that difference was identified as underpinning one’s identity. Pathologization of autistic characteristics may result in “othering” due to a power imbalance whereby autistic differences are perceived to be undesirable.43–45 Othering can make it difficult for a minority or subordinate group to develop or maintain a positive identity, 44 as evident in the narratives of several participants—for example, “It would be nice if there was room in the world for people like me” (P003); and “I already thought that there was something wrong with me and I felt bad already. [She] was reinforcing that idea that there was something wrong” (P013).
Participants reported a lack of validation of their lived experiences and autistic identity by health care providers. Invalidation is likely to have significant and long-term impacts on one’s health and well-being, including internalizing invalidation, overcompensating for the perceived problem, and rejecting or avoiding care, leading to worsening of psychological distress and subsequent intensification of mental illness.46–50 Invalidation of diagnosis can negatively impact on one’s self-identity; many autistic individuals consider that autism underpins their way of being 51 : “When people just say, well, obviously you’re not autistic, it feels like they’re taking away a big part of who I am, as well as invalidating a lot of the struggles that I have” (P007). Invalidation of diagnosis by (often well-meaning) health care providers was a barrier to both access and utilization of services and impacted the provider’s ability to support the autistic person effectively: “It’s an integral part of my mental health. I can’t not be who I am and that’s just part of who I am” (P004). In a further example of the complexity of navigating health care services, participants also shared their understanding that while disclosure of diagnosis often led to invalidation, disclosure was essential to effective utilization of supports:
[Disclosure] helps [health care providers], because autistic people have different thinking processes and sometimes different ways of behaving. (P029)
My Context Is a Complex System
This subtheme represents how a person’s entire life context and circumstances significantly influence how they access and engage with health care services.
Given communication differences and high levels of co-occurring mental and physical health conditions, autistic adults are inherently disadvantaged when navigating interconnected and often complex, unaccommodating, and hostile systems.3,4,6,52,53 Change to complex systems can have unexpected, unplanned, and disproportionate repercussions.54,55 Participants described significant challenges trying to understand and manage systemic changes (and the often unexpected repercussions of those changes): “I felt like things were fine until they weren't and then things would get really, really bad really quickly and it was always when the psychologist thought I was doing well” (P019); “[I can’t] comprehend in my head how people just can’t follow the rules” (P021).
Sometimes I’m a Chameleon
This subtheme represents the participants’ experiences of masking and how those experiences impact and have impacted their interactions with health care providers.
Masking (also camouflaging or compensating) refers to behaviors that may be employed by autistic individuals to hide autistic traits and behaviors considered socially unacceptable, as well as describing artificial social behaviors that are employed to fit into non-autistic society. 56 Masking can be a barrier to access and use of health care services, in terms of not appearing “autistic enough” to qualify for supports: “Because I present pretty normally, on the surface, they don’t really take me seriously” (P009); conversely, masking can be an asset whereby others may assume competence: “I suspect that my experience of working with psychiatrists in particular would have been remarkably much worse if I were not good at masking.” (P001)
Regardless of the effect on accessing and utilizing supports, there was consensus amongst participants that masking had a cost for the autistic person’s self-esteem and identity, by draining emotional resources: “If I go to a conference, or something like that, and I have to be a normal human being for a week, then [I] will have a meltdown for days when I get home” (P007); and increased demands on cognitive processes: “You’re constantly having to translate what you're thinking into something that somebody else is going to understand or not react to” (P026). Participants also reported that their ability to mask could be unreliable: “I try and blend in and sometimes I fail” (P024).
I Am Not a Stereotype
This subtheme represents participants’ frustrations with many health care providers’ (mis)understanding of autism.
A common theme in participant narratives was the stereotypical (mis)understanding of autism held by many health care providers. Participants reported having their competence or capabilities assumed based on their autism diagnosis: “I feel like [because of my diagnosis] both of them were approaching me like I was a child. I didn’t have autonomy, and I didn’t have the right to choose what was happening with me” (P016). Participants also reported having their diagnosis questioned based on the provider’s (poor) understanding of autism: “She completely disregarded everything I said and [told me] if you’re autistic you’d have problems with sensory issues that you could have no way of understanding as a normal person.” (P019)
Theme 3: Help me understand myself
This theme reflects participants’ experiences that self-understanding removes barriers and enhances successful access to and use of supports.
Developing an understanding of oneself and one’s needs could mitigate feelings of failure and shame and reduce associated distress, leading to more successful navigation of supports. Strategies used included metacognition to understand one’s thoughts and behaviors as indicators of mental health challenges: “when I have a lot of trouble navigating small changes in routine and things like that, […] that’s when I’m probably having some extra problems [with my mental health]” (P033); understanding how to choose the best person to support them: “I need less, and I need calm, so I would go to my boyfriend. I would not go to my mother. Despite that their intentions are exactly the same the delivery is very different” (P007); and having simple, concrete solutions: “Keeping it clear and simple and doable, concrete, in terms of, like, go to the beach, or do something action orientated like have a bath” (P006).
Conversely, experiencing difficulties in understanding themselves, their support needs, and their place in the world, added to challenges in accessing and utilizing supports. As one study participant said, when asked what supports might help them where previous tactics had failed, “I honestly don’t know [what supports are available]. It's one of these things; we don’t know what we don't know” (P005).
Getting My Diagnosis Disrupted My World
This subtheme reflects how an autism diagnosis reshaped participants’ perspectives on their life experiences.
For those study participants who discussed being diagnosed as an adult, there was consensus that the diagnosis changed how they viewed the world and their place in it. An autism diagnosis often challenged the commonly held self-belief that the participant was a “failed neurotypical person” and validated their experiences as real rather than imaginary: “It makes sense, it’s changed my self-concept. I’m not a freak; it’s not my fault and it’s not something I have to fix with bloody mindfulness” (P031).
I May Not Understand My Own Needs Without Assistance
This subtheme highlights participants’ struggles in recognizing their needs, behaviors, and support options, as well as identifying solutions.
It can be difficult for an autistic person to recognize their own basic needs (often due to alexithymia and poor interoception), let alone find ways to meet them, especially if one needs support to do so. 57 Participants discussed difficulty understanding how they were feeling, how to support optimal functioning, and what their support needs were: “I think this is a very classic autistic thing where we don’t realize that we’re feeling bad, until we’re feeling horrible” (P007).
Participants also expressed an awareness of choosing maladaptive coping strategies but not knowing how or where to look for support to choose better strategies: “I would probably just try and cope, in a dysfunctional way, like drink too much. I might have a relapse of an eating disorder” (P006); “Nothing positive. I self-medicate with alcohol, basically, switches the brain off and get some sleep” (P012).
Help Me Imagine a Positive Future
This subtheme captures participants’ experiences of psychological rigidity and self-criticism, and the positive changes achievable with proper support.
Rumination, as well as rigid, Black and White thinking are commonly self-reported characteristics of autism both in the current study, and in the wider literature.58,59 Importantly, both rumination and rigidity are linked to increased risk of mental health challenges, including STB.58–60 Study participants acknowledged rumination and rigidity as contributing to their difficulties: “I know that most people with depression have rumination anyway, but my experience of it in terms of autism is that it’s very rigid, like there are rules in place and it’s very structured” (P001).
Participants described thinking about themselves and the future in a way that was rigid and negative: “I’ve grown towards the position that there’s pretty much nothing that can be done to improve my communication abilities from the life stage I’m at. I’ve given up a bit” (P003). Another participant shared their difficulty in finding meaning and value when considering how they fit in the world:
You get up. You go to work. You come home. You do schoolwork and clean the house. You go to bed and then you do it all again tomorrow. I’m not having a profound impact on anything. I’m not creating a cure for cancer. I’m not making meaningful differences to the human species. So, what is the point of me? (P021)
Participants also identified that it is possible, with the right support and an understanding of themselves, to develop a positive appraisal of oneself: “Something is kicking in from knowing––having the information about how my brain is wired is really helping me” (P008). Beyond a simple understanding of one’s own cognition, participants reported the development of increased psychological flexibility, including strategies such as cognitive diffusion and acceptance.61,62 “[What helped was] understanding that the feeling was transitory and even though I had suicidal thoughts I had no intention of acting on them” (P023).
I Need to Be a Person Beyond My Diagnosis
This subtheme represents the ways participants have found meaning and engagement in the world, positively impacting their lives.
Participants discussed positive aspects of their lives in terms of opportunities to contribute meaningfully to the world, and the benefits this brings to the individual making the contribution; meaningful contribution was worthwhile, even when it came at a significant cost to the person making the contribution:
I’m happy to talk and I find meaning if the rubbish I say to you will help someone like my kid. Because I’ve spent 35, 40 years feeling different until I found out I was different. It would have been good if smart people like you and your team would find a way to help kids like mine. So, a momentary sadness or pain [for me] for the betterment of kids like my son is worth it. (P021)
Theme 4: Support me
This theme highlights participants’ experiences that, with appropriate conditions and accommodations, health care providers can offer not only effective but also empowering support.
Previously discussed themes and subthemes constructed from our data are inextricably entwined in our fourth theme, “Support Me.” Participants discussed that when caregivers understand the support needs and strengths of individuals they support, as well as the context inhabited by those individuals, and when the two parties can communicate with each other in ways that foster understanding, the support is most effective. When the individual receiving support understands themselves and their own needs, they gain the most benefit from that support: “He was able to understand what I was saying, and the experiences I was talking about, and help me approach situations in a way that I could manage them more appropriately” (P012).
Help Me to Remove the Known Barriers
This subtheme reflects participants’ recognition of widespread barriers to mental health care access and their need for support to address these challenges.
Participants discussed a range of barriers to effective access and use of mental health care supports (see Supplementary Table S5). Many participants described characteristics of autism itself, and commonly co-occurring conditions (e.g., mood or personality disorders) 63 as barriers to access and utilization of supports, identifying the need for assistance to overcome these barriers:
I get very anxious in medical settings anyway, and then you pile on all of that sensory stuff on top. I find it so overwhelming, and so stressful, that I avoid going, despite having significant health issues … I can’t do it by myself, all that is stuff I need help with. (P007)
Please Help Me to Build My Toolbox
This subtheme reflects participants’ awareness that supporting mental health requires diverse interventions and tools, which can be hard to find or may need adaptation or individualization to work effectively for autistic people.
Participants described a range of complex mental health support needs that often changed over time, related to both autism and co-occurring conditions. One of the difficulties experienced by participants as they attempted to build their toolbox was the need to find and co-ordinate supports themselves, as well as communicate between different caregivers to ensure important information is shared appropriately. “There’s not really much coordination between the different people involved in your [care], my GP writes the new referral letters every six months, but apart from that, no” (P001). Conversely, successful development and maintenance of supportive relationships were perceived positively:
I switched doctors and this new doctor for the last six months or so, she’s had that capacity to ask good questions. Even when I haven’t needed the appointment as such. … She’s been there as a check-in, as an anchor. We’ve maintained that once a month. (P002)
Participants reported that therapies (i.e., counselling/talk therapy, cognitive behavioral therapy, mindfulness), interventions and strategies that were not individualized to their needs were ineffective, suggesting poor person-activity fit. 64
Learning from My Past
This subtheme represents the experience of participants of a self-developed strategy to reduce distress associated with chronic suicidal ideation.
Participants, particularly those experiencing chronic STB, shared that they were able to reframe their reaction to mental ill-health and suicidal ideation by acknowledging that the feeling or thoughts were transitory, adopting an attitude of “this too shall pass.”
It’s better now. (I’ve developed) ways of managing my mental states … or even just accepting an experience if it’s particularly intense. Like feeling suicidal, for instance. But accepting it as an experience that will pass and that will change (P002).
How Do We Find the Good Ones?
This subtheme highlights participants’ challenges in finding health care professionals with a nuanced understanding of autism who can offer tailored care.
When asked, “Can you suggest any changes to a mental health professional or service to assist them to provide better care to autistic people experiencing a mental health or suicide crisis?” participants’ responses centered around the necessity of building ongoing relationships with providers who have a true understanding of, and willingness to engage with, autistic adults and their lived experience. “I think the key issue I find in general is the fact that, unless you really understand being on the [autism] spectrum, it’s difficult to get any effective support” (P026).
Filtering potential supports to find professionals who would be a good fit is seen as a stumbling block. “I think in practice finding professionals who do have that needed understanding, that’s where the hard part is” (P028); there were several suggestions indicating that a way to filter supports would be welcomed and useful: “[We need a way of] making it easy to locate [and] identify professionals who are autism friendly and are experienced with autism” (P030).
Underpinning theme: Trust and safety
This theme captures participants’ experiences that psychological safety and trust are essential components of successful support relationships: “The first thing I need is to [feel] safe […] If I don’t trust you, you can’t help me” (P030). It further reflects participants’ perception of the world as often feeling unsafe, particularly in health care interactions. However, when providers prioritized psychological safety, participants reported improvements in support. An individual’s experience can range from one that generates safety and trust to one that is actively harmful. One participant discussed their experience of being hospitalized following a second suicide attempt immediately after discharge from hospital for an initial attempt:
I saw a psychiatrist […] after attempting [suicide] while I was still in a medical ward […] he was doing a lot of gaslighting. I think it was an attempt to absolve the hospital of responsibility for my [suicide] attempt. (P027)
And then their later experience during the same admission of connecting with a caregiver who established a relationship grounded in cultural humility, a power-with dynamic, and ultimately, psychological safety:
She responded with understanding when I would do things. Like if I identified I was heading towards a meltdown she understood the significance of that and understood what ways best to help me. She never, ever, ever touched me without permission. She understood that if I said I needed 15 mins of leave to be able to go around the block to decompress, she would overrule the nurse who said “no” because they thought I was too big of a risk. Things like that. She understood how to communicate with me. [That was the] difference between knowing the world and everything in it is hopeless and there’s no point in trying because it’s actively hostile to your existence; and knowing that in spite of the world being hostile, there are parts of it that are safe. (P027)
Final Considerations
Our study demonstrates, through the lived experience of autistic adults, an imperative for change in the ways autistic people access and interact with health care services. The removal of barriers to access and use, and adaptation of approaches, systems, and interventions, to better accommodate the needs of autistic people is critical. Here, we aimed to produce useful, operationalizable knowledge that would honor the contribution of study participants. Our quality assessment (see Supplementary Data and Supplementary Table S1) demonstrates how our findings expand on existing research. The themes and framework developed herein bridge the gap between the positive intent of health care services and the unmet needs of autistic individuals seeking support, enabling autistic people to clarify and articulate their (mental) health care needs and guide them in self-advocacy. Health care providers might use this framework to critically assess their service offerings through the lens of each central theme. Our findings serve as a useful reminder to health care providers to interrogate their own biases and assumption. Importantly, we identify the crucial need for embedding trust and safety into systems and processes to improve health care outcomes for autistic people.
Implications for clinical practice
It is both poignant and concerning that several participants perceived a health care provider as being angry with them during interactions, raising concern for their well-being when seeking support. We suggest that health care services and providers need to adapt their understanding of, and communication with autistic people. This will require targeted training that addresses the diverse presentations and support needs of autistic adults. It may also require education for autistic adults to better understand themselves and their own support needs.
Health care providers must ensure that psychological safety is embedded within their services. Psychological safety can include one’s assessment of the consequences of taking interpersonal risks in each situation. 65 High levels of psychological safety occur when an individual is confident that they would not be embarrassed, rejected or punished for speaking up or for being their whole, authentic self.65–67 Health care systems, or actions taken by health care providers (e.g., failure to validate an individual’s autistic identity) may inadvertently erode psychological safety. 68 Moreover, there is an inherent, and often unchallenged, power imbalance between mental health care services staff and the people utilizing that service. 69 Without explicitly addressing this issue, this power imbalance may manifest in dynamics where the health care provider, however well-intentioned, has (coercive) power over the consumer.70,71 In contrast, when the caregiver consciously and deliberately shares power with the consumer, a collaborative, generative relationship of power with can develop.70,72 Cultural humility describes a personal accountability-based approach to managing this potential power imbalance. 73 It requires the health care provider to recognize their biases, and to actively work to recognize and respect each individual’s identity, experiences, beliefs, preferences, and the context they inhabit as an essential part of the consideration when interacting with, treating, and discussing their care.73–75 Cultural humility fosters a culture of trust and safety, and warrants further consideration by health care providers as a means of establishing a psychologically safe environment.69,73,76
There is emerging evidence that traditional therapies and interventions may be less effective when used with autistic adults.77,78 However, person-activity fit may be improved through individualization and appropriate adjustment. For example, adapting cognitive behavior therapy to accommodate autistic people’s needs may improve its effectiveness in this population. 79 Precision medicine that is tailored to an individual’s unique circumstances and needs may also improve outcomes, an approach supported by the autistic community.15,16,18,79,80 Conversely, a lack of contextualized autism knowledge and failure to individualize treatment are consistently recognized as barriers to access.81,82 A flexible approach to supporting autistic people’s mental health and that acknowledges and validates the person’s autistic identity is required. 83
There is a need to prioritize access and remove barriers to services (e.g., due to [mis]communication). Moreover, services must be psychologically safe. We identified several actions that could be implemented immediately to improve outcomes, for example, providing information in multiple formats (e.g., oral instructions, written instructions, video, social narratives) might improve comprehension. Nonetheless, it will require significant iterative consultation with the people most impacted, and further interrogation of the underlying problems inherent in a system that fails to meet the needs of the people it aims to serve. It is also important to acknowledge the stories of participants that inspire hope. These stories described positive interactions where they felt listened to and validated, supporting our optimism that positive change is achievable.
Community involvement: Outcomes and critical reflection
Our study was strengthened by community engagement leading to our identification of priority research areas (see Supplementary Table S6 for Guidance for Reporting Involvement of Patients and the Public, Short Form). 23 The diversity of experience and representation of the various community members contributed greatly to our research outcomes. This contrasts their experiences within complex health care systems where their voices were too often invalidated. Nonetheless, we acknowledge that the finalization of research questions, interviews, and interpretation of data were led by the research team.
Limitations
Most participants identified as women and were highly educated, limiting the generalizability of our findings to other autistic cohorts and not reflecting the typical gender ratio in autism. 84 As this study was conducted in Australia, our ability to generalize findings to other geographic locations and cultures is limited. Our results are also not generalizable to autistic adults with profound communication challenges, or those with co-occurring intellectual disability.5,85 Finally, undiagnosed or possibly autistic adults without formal identification were not included in this study, although we acknowledge that this group is likely to be at increased risk of STB.86,87
Footnotes
Acknowledgments
We thank the individuals who participated in this study and who were so willing to share their experiences with us. We also thank ASPECT Think Tank and the members of our autistic advisory group who made significant contributions to our research program, and for contributing to the development of the interview guide. We would like to acknowledge Kathleen Denney and Ensu Sahin for their assistance with data collection and Dr. Simon Bury, Dr. Angela Clapperton, Professor Cheryl Dissanayake, Professor Jo Robinson, Professor Julian Trollor, and Dr. Mirko Uljarević for their valued input to the research program and to the development of the interview guide.
Language Use
In this article we use identity-first language (IFL). IFL is preferred by the study advisory group as well as the study’s autistic authors. We acknowledge that some people with a diagnosis of autism prefer person-first language.
Data Access
Requests for access to the data sample should be directed to D.H.
Ethics Statement
The research was approved by La Trobe University Human Research Ethics Committee HEC20235. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from participants after the nature of the study was explained.
Authorship Confirmation Statement
D.H., M.A.S., and D.N. designed the study. D.H. collected the data with the assistance of a research assistant. J.W. analyzed the data. D.H. and J.W. wrote the article with input from all authors. All authors reviewed and approved the final version of the article. The article has been submitted solely to Autism in Adulthood.
Author Disclosure Statement
At the time of the study, D.H. was supported by a
Funding Information
This research was supported by research funding from Untapped Holdings awarded to D.H., a Suicide Prevention Australia National Suicide Prevention Research Fellowship awarded to D.H., and a Suicide Prevention Australia National Suicide Prevention Post-Doctoral Research Fellowship awarded to C.M.B. The funders had no role in the study design, data collection, analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and final responsibility for the decision to submit the report for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.