
Abstract
Background:
Racial/ethnic disparities in access to diagnostic services are pervasive for autistic children. However, a few studies have examined racial/ethnic health disparities among autistic adults, who commonly experience higher rates of health conditions than non-autistic adults. We aimed at examining the intersection of autism and race/ethnicity in association with psychiatric and medical diagnoses.
Methods:
The study population included adult members of Kaiser Permanente Northern California enrolled from 2008 to 2012. We ascertained 1507 adults who had an autism diagnosis documented in their electronic medical records. We sampled a matched control group of adults without an autism diagnosis (N = 15,070) at a 10:1 ratio. Our sample was 46% White, 17% Hispanic, 16% Asian, 7% Black, and 14% other race/ethnicity. We compared health diagnoses (a) between autistic and non-autistic adults within strata of race/ethnicity and (b) across race/ethnicity within strata of autistic and non-autistic adults. Lastly, we examined the interaction between autism and race/ethnicity on both multiplicative and additive scales.
Results:
Autistic adults were more likely to be diagnosed with most medical and psychiatric conditions compared with their non-autistic counterparts of the same race/ethnicity. Among autistic adults, Black, Hispanic, and Asian adults were less likely to be diagnosed with psychiatric conditions and Black and Hispanic autistic adults were more likely to be diagnosed with obesity than their White counterparts. In interaction models, we found that adults who were Black and autistic were disproportionately less likely to be diagnosed with psychiatric conditions and autoimmune disease and more likely to be diagnosed with hypertension than expected.
Conclusion:
Health vulnerabilities may be compounded at the intersection of autism and race/ethnicity. Future research should continue to apply an intersectional lens toward understanding and addressing these disparities. Our findings likely underestimate the health disparities that exist in uninsured autistic adults and those living in other parts of the United States.
Community brief
Why is this an important issue?
Very few studies have looked at how the combination of a person's autistic and racial/ethnic identities affects their health in adulthood. Dual experiences of ableism and structural racism may have a larger negative effect on the health of autistic people of color than either one experience alone. It is important to identify potential health disparities so that they can be addressed.
What is the purpose of this study?
We wanted to understand whether autistic adults of color were more likely to be diagnosed with medical and psychiatric conditions than non-autistic and/or White peers.
What did the researchers do?
We studied a diverse group of 1507 autistic adults and 15,070 non-autistic adults who all received health care from the same large, health plan in California. We examined electronic health records to determine whether diagnoses of health conditions differed by autism status and race/ethnicity. We then looked at whether autistic people of color were disproportionately diagnosed with these conditions compared with other groups.
What were the results of the study?
Within every racial/ethnic group, autistic adults were more likely than non-autistic adults to be diagnosed with most medical and psychiatric conditions. Among the autistic group, Black, Hispanic, and Asian adults were less likely to be diagnosed with psychiatric conditions compared with White adults. We saw similar differences in psychiatric diagnoses by race/ethnicity among non-autistic adults. Further, the diagnostic patterns among adults who were autistic and Black suggested that this group may experience unique difficulties receiving mental health and autoimmune diagnoses. They also may be at a higher risk of hypertension.
What do these findings add to what was already known?
Previous studies have found racial/ethnic disparities in both mental health and access to health care among autistic children. This study suggests that racial/ethnic disparities, especially in mental health care, may also exist among autistic adults.
What are potential weaknesses in the study?
As a broad social label, race/ethnicity does not tell us much about people's lived experiences. Future studies should replace race/ethnicity with more useful measures of our social environment, including economic opportunity and experiences of structural racism. In addition, health records may imperfectly represent the actual occurrence of health conditions. For example, we cannot tell from this study whether autistic people of color actually experience fewer psychiatric problems, are less likely to visit the doctor, or are more likely to have their problems missed by doctors. Lastly, because our findings are from an insured population, we have likely underestimated the health disparities that exist among autistic adults who do not have consistent insurance coverage or health care access.
How will these findings help autistic adults now or in the future?
We hope this study highlights the need for greater attention to the unique health risks at the intersection of autism and race/ethnicity in adults. Through more research and advocacy, we can increase awareness and understanding of these potential health disparities. This will lead to changes that promote more equal access to health care and greater well-being among autistic people of color.
Background
Autistic individuals tend to have more co-occurring medical and psychiatric conditions than the general population. 1 Some chronic conditions experienced by autistic people, especially mental health conditions, can cause daily impairment 2 and may increase risk of early mortality. 3 These poorer health trajectories appear to emerge in childhood and persist into adulthood,4–6 necessitating high health care use throughout the lifespan. 7
Other chronic conditions that disproportionately impact autistic adults, such as heart disease and obesity, gradually onset in adulthood and are often preventable with early intervention. Though autistic people have high health care spending, they often have worse access to high quality care, 8 such as evidence-based mental health services and medical homes, compared with non-autistic populations. 9
Racial and ethnic disparities in health and health care access may further compound the health care barriers experienced by autistic individuals. In the United States, people from historically marginalized racial and ethnic groups are less likely to receive care for preventive health and mental health. 10 Further, numerous studies suggest that racial/ethnic inequalities also pervade access to diagnostic and support services for autistic children and youth. In particular, Black and Hispanic children are more likely to have delayed diagnosis of autism and to receive fewer developmental and intervention services compared with White children.11–14
Unequal access to health care and health knowledge, racial prejudices in provider or health care diagnostic practices, cultural attitudes, language barriers, and neighborhood and socioeconomic factors are several of the known contributors to racial disparities in the general population.15,16 For autistic people from historically marginalized groups, these barriers may be even more pronounced and compounded by low provider awareness of autism, diagnostic overshadowing of co-occurring health conditions, patient challenges with communication and self-advocacy, difficulties with emotion regulation, and lack of accommodations for caregiver involvement.17–22
These health care disparities and the potential for greater marginalization at the intersection of autism and race/ethnicity have implications for health and well-being into adulthood. 23 Although research on the experiences of autistic adults is growing, very few studies have moved toward an intersectional framework24,25 of understanding how multiple forms of inequalities combine and interact in this population, specifically with respect to health status and health care use. 26
Intersectionality, as conceptualized by Dr. Kimberle´ Crenshaw, acknowledges the complex and multidimensional forms of compounded oppression that people experience when they hold identities that are multiply marginalized.25,27 For autistic people of color, they have their disability identity and their racial/ethnic identity that intersect and shape their experiences within the health care system. Thus, using an intersectional framework that incorporates and considers the sociohistorical roots of race and disability allows for empirical investigations that can better address health inequities and outcomes for historically marginalized communities. 28
Early evidence indicates that autistic adults from historically marginalized racial/ethnic groups in the United States face unequal eligibility for public health insurance programs and lower health care spending than White autistic adults. 29 Studies of adults with intellectual and developmental disabilities (IDD), more generally, have reported similar patterns of lower developmental, social, and health service access, as well as poorer health status, among people belonging to historically marginalized racial/ethnic groups compared with White peers.30,31 These studies suggest that the intersectional presence of race and disability can exacerbate disparities through the existence of double oppressions (racism and ableism) covertly embedded in systems of care.32,33
The aim of the present study was to examine racial/ethnic differences in the frequency of psychiatric and medical diagnoses in a diverse population of insured autistic adults who all have access to care at the same integrated health care system in Northern California. Though this population may experience less inequity than uninsured adults, we hypothesized that we would still see differences in health diagnoses by race/ethnicity, consistent with extant evidence of racial/ethnic disparities in autistic children and in the general population.
Methods
Setting and study population
The study took place at Kaiser Permanente Northern California (KPNC), a large, integrated health care delivery system that provides health care to ∼25%–30% of the San Francisco and Sacramento metropolitan areas and surrounding counties. KPNC's members are broadly representative of the local and statewide population in terms of sociodemographic characteristics, except for the extremes of the income distribution.34,35 Members were eligible for the study if they were adults 18 years of age as of January 2008 and were members of KPNC for at least 9 months in each calendar year from January 2008 to December 2012 (study details previously described in Croen, 20151).
From this pool, we ascertained 1507 adults who had an autism spectrum disorder (ASD) diagnosis (Autism: International Classification of Diseases-9-Clinical Modification [ICD-9-CM] 299.0; Asperger's Disorder [ICD-9-CM 299.8], Pervasive Developmental Disorder, Not Otherwise Specified [ICD-9-CM 299.9]) documented in their KPNC medical records on at least 2 separate occasions anytime before December 2012. At a 10:1 ratio, we matched a randomly sampled comparison cohort of non-autistic adults (N = 15,070) on sex assigned at birth and 5-year age groupings to adults in the autistic cohort.
Medical and psychiatric conditions
We determined the prevalence of health conditions by examining physician-documented medical and psychiatric diagnoses routinely captured in KPNC's electronic health records (EHR) between January 2008 and December 2012. Details about the specific conditions and ICD-9 codes are presented in earlier work 1 and are available in the Supplementary Table S1. These codes captured prevalent and incident conditions that were active during the study period.
Sociodemographic variables
From the EHR, we extracted age, and insurance payer (private or government) as of January 1, 2008, and length of KPNC membership (months) during 2008–2012, sex, and race/ethnicity. We based race/ethnicity on self-reported variables recorded in the EHR. We used these variables to categorize race/ethnicity as Hispanic, non-Hispanic Black/African-American, Asian, and non-Hispanic White. Due to small numbers, we combined members who identified as American Indian, Alaskan Native, Native Hawaiian, or Pacific Islander (n = 178) or who did not have race/ethnicity information in the EHR (n = 2136) in the category of “Other race/ethnicity.” Hispanic KPNC members were primarily Mexican American whereas Asian KPNC members were primarily Chinese, Filipino, and South Asian American.36,37 However, we had insufficient sample size to further evaluate these narrower racial/ethnic subgroups.
Ethical approval
All study procedures were approved by the KPNC Institutional Review Board (IRB# 00001045).
Statistical analyses
We estimated adjusted prevalence ratios (PRs) using modified Poisson regression, 38 controlling for age, sex, length of KPNC membership, and insurance payer. We first compared the prevalence of medical and psychiatric conditions between autistic and non-autistic adults of the same race/ethnicity in models stratified by race/ethnicity. Next, we examined differences in the prevalence of medical and psychiatric conditions across race/ethnicity, in models stratified by autistic adults and non-autistic adults.
To examine whether psychiatric and medical conditions occurred more or less frequently among individuals with intersectional identities (i.e., autistic and belonging to a historically marginalized racial/ethnic group) than would be expected from multiplying the independent associations of autism and race/ethnicity together, we examined PR models with an interaction term between autism status and race/ethnicity. 39 To assess departures from additivity, we used the regression output to calculate the relative excess risk due to interaction (RERI = PR11 − PR10 − PR01 + 1), using the delta method for 95% confidence intervals (CIs).40,41
An RERI >0 indicated a positive additive interaction or that the joint association of race/ethnicity and autism on a specific health outcome was greater than the sum of their individual associations, whereas an RERI <0 indicated a negative interaction or that their joint association was less than their sum. An RERI = 0 indicated no additive interaction. We used an alpha = 0.05 to assess statistical significance on the multiplicative and additive scales.
Results
Compared with the non-autistic cohort, the autistic cohort was more likely to be White (65.6% vs. 44.0%) and less likely to be Hispanic (9.5% vs. 17.9%) and Asian (10.6% vs. 16.3%). Black adults constituted ∼7% of both cohorts (Table 1). Reflecting trends in autism prevalence, the study sample was skewed toward young adults and males. Though the cohorts were matched on sex and age, the distributions of these variables differed across race/ethnicity. For example, autistic Asian, Black, and Hispanic adults were on average younger than their non-autistic counterparts.
Demographics of the Study Population by Race/Ethnicity, Kaiser Permanente Northern California
Other category includes American Indian, Alaskan Native, Native Hawaiian, or Pacific Islander (∼1%) and individuals who did not have race/ethnicity information in the EHR.
EHR, electronic health records; KPNC, Kaiser Permanente Northern California.
Among autistic adults, White adults had the oldest mean age (30.7 years) while Hispanic (24.8 years) and Asian adults (25.2 years) had the youngest mean ages. A quarter of autistic adults had Medicaid as their insurance payer compared with 1.4% of non-autistic adults; these fractions were slightly higher among autistic and non-autistic Black adults (33.9% and 7.1%, respectively).
Prevalence of psychiatric conditions
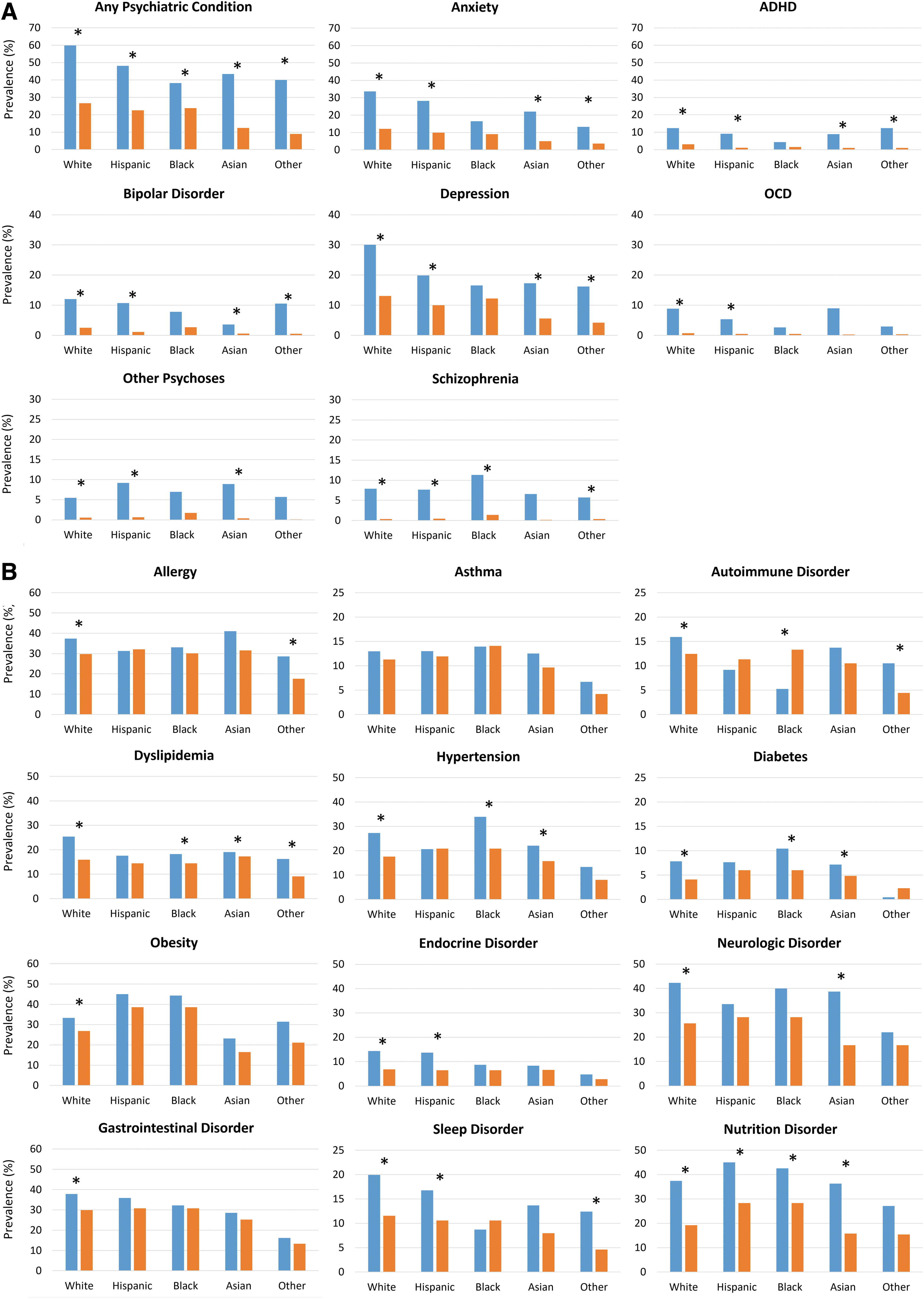
The prevalence of psychiatric conditions among autistic adults varied considerably by race/ethnicity (Fig. 1A and Supplementary Table S2); White autistic adults had the highest rate of any psychiatric condition (59.8%) followed by Hispanic (46.9%), Asian (44.0%), other race/ethnicity (40.0%), and Black autistic adults (38.4%). Anxiety and depression were the most prevalent psychiatric diagnoses among autistic adults across all racial/ethnic groups, but rates differed widely by race/ethnicity; White adults had the highest rates of anxiety and depression (33.6% and 30.1%, respectively), and Black adults had the lowest rates (17.0% for each condition). Schizophrenia-spectrum disorders had a different pattern, with Black autistic adults having the highest rate (10.7%) and Asian and other race/ethnicity autistic adults having the lowest rates (6.9% and 5.7%, respectively).
Prevalence of psychiatric
Similar psychiatric diagnostic profiles were observed among non-autistic adults, with some exceptions (Fig. 1A and Supplementary Table S2). For example, although White non-autistic adults had the highest prevalence of anxiety and depression, there were smaller differences in prevalence by race/ethnicity than observed in the autistic cohort.
Psychiatric conditions by ASD status, stratified by race/ethnicity
Autistic adults generally had significantly higher rates of co-occurring psychiatric conditions compared with their non-autistic counterparts of the same race/ethnicity, with the majority of PRs exceeding 2 (Fig. 1A and Supplementary Table S3). However, the magnitude of this contrast varied by racial/ethnic group. For example, the PRs for anxiety (adjusted prevalence ratio [aPR] = 1.64, 95% CI: 0.99 to 2.72) and depression (aPR = 1.33, 95% CI: 0.81 to 2.18) between autistic and non-autistic adults were the smallest among Black adults and not statistically significant.
Psychiatric conditions by race/ethnicity, stratified by ASD status
After adjusting for covariates, Black, Asian, and other race/ethnicity autistic adults were markedly less likely to be diagnosed with any psychiatric condition overall as well as several individual conditions, including anxiety, attention-deficit/hyperactivity disorder (ADHD), and depression, than their White autistic counterparts (Table 2). In addition, bipolar disorder was less often diagnosed in Asian autistic adults whereas obsessive compulsive disorder was less often diagnosed among Black and Other race/ethnicity autistic adults.
Prevalence Ratios of Psychiatric and Medical Conditions Comparing Race/Ethnic Categories, Among Autistic Adults, Kaiser Permanente Northern California, 2008–2012
Other category includes American Indian, Alaskan Native, Native Hawaiian, or Pacific Islander (∼1%) and individuals who did not have race/ethnicity information in the EHR.
Models adjusted for age, sex, KP membership length, and insurance payer.
Model did not converge due to small cell counts.
p < 0.05.
ADHD, attention-deficit/hyperactivity disorder; aPR, adjusted prevalence ratio; CI, confidence interval.
Hispanic and Asian autistic adults were two times more likely than their White counterparts to be diagnosed with other psychoses (i.e., delusional disorders, brief psychotic disorders, and other psychoses not related to schizophrenia-spectrum disorders). The prevalence of several other psychiatric conditions was also lower among Hispanic autistic adults relative to White adults but these estimates were not statistically significant.
Similar patterns by race/ethnicity were seen for anxiety, ADHD, bipolar disorder, depression, and any psychiatric condition in non-autistic adults after adjusting for covariates (Supplementary Table S4). In contrast to observations in the autistic cohort, obsessive-compulsive disorder (OCD) and other psychoses were diagnosed less often among Asian adults in the non-autistic cohort. The PRs for other psychoses and schizophrenia-spectrum disorders were also higher for Black adults in the non-autistic cohort than observed in the autistic cohort.
Intersection of ASD status and race/ethnicity with respect to psychiatric conditions
On both the multiplicative and additive scales, Black autistic adults had a lower prevalence of psychiatric conditions than would be expected based on the independent associations of ASD and Black race/ethnicity with psychiatric conditions, suggesting a negative interaction between these two factors (Table 3). We additionally observed evidence of a negative interaction between ASD and Black race/ethnicity on other psychoses and schizophrenia-spectrum disorders on the multiplicative scale and anxiety, ADHD, depression, and OCD on the additive scale (Table 3).
Interaction of Autism Status and Race/Ethnicity with Respect to Psychiatric and Medical Conditions
Other category includes American Indian, Alaskan Native, Native Hawaiian, or Pacific Islander (∼1%) and individuals who did not have race/ethnicity information in the EHR.
Models adjusted for sex, age, KP membership length, and insurance payer.
Interaction p-value on cross-product term of autism status and race/ethnicity. Reference group is White non-autistic adults.
p-value <0.05.
RERI, relative excess risk due to interaction.
In contrast, we observed a positive interaction (i.e., higher than expected prevalence) between ASD and Asian race/ethnicity with prevalence of anxiety and other psychoses on the multiplicative scale and a negative interaction with bipolar disorder on the additive scale (Table 3).
Prevalence of medical conditions
The prevalence of several medical conditions among autistic adults varied by race/ethnicity (Fig. 1B and Supplementary Table S2), including relatively common conditions such as allergies, cardiovascular diseases, obesity, neurologic conditions (e.g., epilepsy, migraines), and nutrition conditions (e.g., symptoms related to nutrition metabolism and development). One exception was asthma prevalence, which showed the least variation by race/ethnicity among autistic adults. Among non-autistic adults, the prevalence of obesity, neurologic diseases, and nutritional diseases varied the most by race/ethnicity.
Medical conditions by ASD status, stratified by race/ethnicity
After adjusting for covariates, many major chronic medical conditions, except for asthma, were significantly more common among autistic adults compared with non-autistic adults of the same race/ethnicity (Fig. 1B and Supplementary Table S3). In particular, cardiovascular diseases, diabetes, obesity, endocrine disorders, neurologic diseases, and nutritional conditions tended to be more common among autistic adults than non-autistic adults of the same race/ethnicity, though the PR was not always statistically significant. We observed no difference in the prevalence of sleep disorders between Black autistic and non-autistic adults, though sleep disorders were generally more common among autistic versus non-autistic adults in the other racial/ethnic strata.
Medical conditions by race/ethnicity, stratified by ASD status
Among autistic adults, the prevalence of several medical conditions varied by race/ethnicity (Table 2). We observed a higher prevalence of obesity among Hispanic (aPR = 1.44, 95% CI: 1.18 to 1.77) and Black (aPR = 1.38, 95% CI: 1.10 to 1.73) autistic adults and a lower prevalence of obesity among Asian autistic adults (aPR = 0.73, 95% CI: 0.54 to 0.99) compared with White autistic adults. Hispanic adults were also more likely to have nutrition conditions (aPR = 1.30, 95% CI: 1.06 to 1.58) than White adults.
Black adults, on the other hand, were less likely than White adults to be diagnosed with autoimmune disease (aPR = 0.31, 95% CI: 0.13 to 0.73) and sleep disorders (aPR = 0.48, 95% CI: 0.26 to 0.89) but they were more likely to be diagnosed with hypertension (aPR = 1.52, 95% CI: 1.17 to 1.98) and diabetes (aPR = 1.82, 95% CI: 1.03 to 3.21).
Among non-autistic adults, racial/ethnic differences in the frequency of medical conditions were more prominent (Supplementary Table S4). Compared with White non-autistic adults, Hispanic and Black non-autistic adults had a higher prevalence of several chronic conditions, including cardiovascular disease, obesity, and nutrition conditions. Hispanic non-autistic adults, in addition, had a higher prevalence of allergy, dyslipidemia, endocrine disorders, and gastrointestinal disorders. Although the prevalence of cardiovascular disease and diabetes was also significantly elevated among Asian non-autistic adults, the prevalence of other conditions, including asthma, obesity, and sleep disorders was lower than in White non-autistic adults.
Intersection of ASD status and race/ethnicity with respect to medical conditions
On both multiplicative and additive scales, Black autistic adults had lower than expected prevalence of autoimmune disorders (i.e., evidence of negative interaction) and higher than expected prevalence of hypertension (i.e., evidence of positive interaction) (Table 3). On the additive scale only, the prevalence of sleep disorders was lower than expected in Black autistic adults. Multiplicative interaction models also suggested evidence of other joint associations, including higher than expected prevalence of neurologic and nutrition conditions among Asian autistic adults and higher than expected prevalence of autoimmune diseases among other race/ethnicity autistic adults.
Discussion
Among the large and diverse member population of KPNC, we observed differences in the prevalence of various psychiatric and medical conditions by race/ethnicity among autistic adults. Although the prevalence of psychiatric diagnoses was high among autistic adults overall, Hispanic, Black, and Asian autistic adults were less likely to be diagnosed with any psychiatric condition than White autistic adults. These racial/ethnic differences in the prevalence of psychiatric conditions were generally similar among non-autistic adults.
With respect to medical conditions, we observed less variation by race/ethnicity among the autistic group than in the non-autistic group. Using interaction models on the multiplicative and additive scales, we observed evidence that individuals with intersectional identities of both autistic and either Hispanic, Black, or Asian race/ethnicity had elevated health vulnerabilities, in terms of both lower than expected diagnosis of some conditions (e.g., mental health and autoimmune conditions) and higher than expected diagnosis of others (e.g., hypertension).
Our analyses also suggested that other identities at the intersection of autism and race/ethnicity may also be more vulnerable to certain health conditions, but these interactions were only significant on either the additive or multiplicative scale. Although the additive scale is noted for its public health relevance for making decisions regarding resource allocation, evidence of interaction consistent on both scales can be more indicative of intersectional vulnerability than interaction on either scale alone. 42
Our finding of a lower prevalence of mental health diagnoses among autistic adults belonging to historically marginalized racial/ethnic groups is in line with studies demonstrating racial/ethnic inequalities in access to mental health care in the U.S. population. Although studies of health services in autistic adults are sparse, one study reported greater unmet mental and behavioral health care needs among Black versus White autistic adults. 43
Studies also indicate that children from racial/ethnic minority groups tend to have lower access to ASD diagnostic and support services, 44 and that Black and Hispanic children typically receive fewer mental health services, 45 including psychiatric evaluation and developmental screenings, than non-Hispanic White children. 46 Asian, Black, and Hispanic autistic children also have been found to be less likely to receive psychotherapeutic medication for behavioral challenges and hyperactivity than White children. 47
These findings are mirrored in the general adult population where disparities in mental health care for Black, Hispanic, and Asian adults relative to White adults are significant, spanning both outpatient visits and medication use.48,49 Thus, our findings of racial/ethnic differences in mental health likely reflect systematic under-detection among some groups rather than a truly lower psychiatric risk. Provider bias and discrimination when treating patients of color, a paucity of trauma-informed care approaches that are sensitive to experiences of racism and racialized trauma, cultural stigma around mental health, and the predominance of racially discordant patient–provider interactions are known to contribute to medical mistrust, avoidance of mental health care, and mental health disparities in the general population.16,50–52
Alternatively, there may be protective mental health factors within some racial/ethnic communities, including alternative coping mechanisms and racial/ethnic socialization to chronic stress, meriting more investigation.53–61
A few studies have closely examined intersectional effects among autistic people of color who additionally encounter systemic ableist discrimination. 19 However, our findings are somewhat consistent with two studies that identified racial/ethnic health disparities among autistic adults and adults with IDD more generally.31,62 In Medicaid data, Black, Hispanic, and Asian/Pacific Islander autistic beneficiaries tended to be less frequently diagnosed with mental health conditions, with the exception of schizophrenia, and more frequently diagnosed with several medical conditions including hypertension and diabetes in comparison with White autistic counterparts. 62
Black and Hispanic autistic adults, in addition, had a higher prevalence of obesity. In a separate study, Black and Latino adults with IDD were more likely to report poor physical and mental health and to have higher rates of obesity and diabetes than their peers without IDD of the same race/ethnicity. 31 Although we also observed higher rates of psychiatric conditions among autistic versus non-autistic adults within each race/ethnicity in our study, we observed that the mental health differences between autistic and non-autistic Black adults were generally less pronounced than in other racial/ethnic groups.
Unlike the study by Magana et al, which surveyed patients about their mental health symptoms directly, we examined EHR diagnoses, which are subject to differential access to diagnostic services. Although Black autistic adults likely do experience more mental health symptoms than their non-autistic counterparts, our interaction results suggest that the prevalence of psychiatric diagnosis is lower in this group than would be expected based on combining the individual effects of their two identities together.
These results may indicate that Black autistic adults disproportionately experience more barriers in access to mental health diagnosis and/or treatment than non-autistic peers and autistic people from other racial/ethnic backgrounds. However, little research has examined the health care barriers and facilitators experienced by autistic people of color. Autistic narratives suggest that providers may be more likely to dismiss or misdiagnose symptoms of autistic patients of color who present with or communicate health issues atypically. 63
Anecdotal evidence also indicates that adults with intersectional identities may feel a greater need to mask both autistic traits and psychiatric symptoms in health care settings or avoid seeking mental health care out of concern of being further marginalized and stigmatized.63,64 On the other hand, Black autistic adults were also less likely than expected to be diagnosed with other psychoses and schizophrenia-spectrum disorders. These two conditions tend to be diagnosed at greater rates among Black adults compared with White adults in the general population, though whether this is due to clinical bias or to a higher vulnerability stemming from social adversity remains unclear.65,66
More work is needed to understand whether Black autistic adults were less likely to be diagnosed with these conditions because of under-diagnosis, misdiagnosis, or truly lower symptomatology. 56
Several racial/ethnic differences in medical conditions among autistic adults, such as a higher prevalence of obesity among Black and Hispanic adults and a higher prevalence of diabetes and hypertension among Black adults, mirrored findings in non-autistic adults. The disproportionate burden of metabolic and cardiovascular disease in Black and Hispanic adults is well documented in the general U.S. population67–69 and has also been observed in studies of adults with IDD. 31 We observed evidence that adults who were autistic and non-Hispanic Black or Hispanic had greater than expected prevalence of hypertension, but the synergism was not consistent across scales of interaction.
We also observed a lower than expected prevalence of sleep and autoimmune conditions among Black autistic adults. Although these findings warrant closer attention, they were not replicated in a larger sample using Medicaid data. 62 Nevertheless, future studies can expand this intersectional framework to also consider disparities in mortality and morbidity stemming from these conditions. Research suggests that inequities in care and delayed diagnosis may contribute to faster disease progression and elevated risk of severe disease and health complications, such as has been seen with hypertension, autoimmune diseases, and sleep disorders among Black adults in the general U.S. population.70–73
While enhancing equitable access to preventive care is one target for interventions, the factors contributing to these differences are multilevel, reflecting a confluence of systemic (racial discrimination, residential segregation),74,75 cultural (e.g., spoken language, cultural attitudes toward care-seeking, and mental health stigma), 16 and individual factors (e.g., health literacy, lifestyle) operating both independently and interactively. In one study among adults with IDD, differences in the use of preventive care between Black and Hispanic adults were attenuated after adjusting for factors such as severity of intellectual disability, mobility, language, and living situation. 76
Though we did not have information on living arrangements, other studies have found that adults with IDD who live at home with family are more likely to have obesity than peers living in group settings. 77 These studies underscore the need for greater attention to the unique factors at the intersection of race and autism, including the level of support needs and types of disabilities, communication differences, and living arrangements, that may contribute to racial/ethnic disparities in autistic adults.
Our study has several key strengths, including its large and diverse sample of autistic adults. All adults in our sample had health insurance and were members of the same integrated health care system, which generally reduces variance related to quality of care by different insurance plans and health networks. The use of EHR also allowed us to look comprehensively at both psychiatric and medical health status, though studies are needed that can carefully examine disparities with respect to specific conditions within these broader diagnostic categories.
There are several important limitations to our study. First, we acknowledge that race/ethnicity is a crude social categorization and is not based on any meaningful biological difference. The purpose of using race/ethnicity was to identify potential health disparities and lay the groundwork for future studies that can deconstruct race/ethnicity into more useful and specific measures of social determinants of health such as educational attainment, economic opportunity, neighborhood factors, cultural attitudes, and experiences of structural discrimination and racism. 78
Within the conceptual framework of Kilbourne et al, our study falls into the first phase of detecting disparities, to be followed by next steps of understanding and reducing the determinants of these disparities. 79 Further, although race/ethnicity was based on self-report, the categories captured were broad and likely masked wide heterogeneity within each group, including the experiences of mixed race and specific ethnic groups. 37 We also did not have a sufficient sample size to disaggregate racial/ethnic groups such as American Indians, Alaskan Natives, Native Hawaiians, or Pacific Islanders.
The presence of psychiatric and medical conditions was determined by diagnoses recorded in the EHR and were not necessarily validated by a standardized clinical exam or by chart reviews. There could be bias in how diagnoses are determined, for example, if physicians apply diagnostic criteria differently or are more likely to look for certain conditions depending on the race/ethnicity of their patient. 80 Thus, physician-recorded diagnoses may have imperfectly approximated the actual prevalence of these conditions in our study population.
Further, using body mass index to classify obesity may be less accurate than other measures of adiposity at capturing cardiometabolic risk for some racial/ethnic groups. 81 We also did not have information on disease severity and duration, which are also important facets of health disparities. Lastly, although our population was sociodemographically diverse and included a large number of autistic patients with government health insurance, the KPNC population is not necessarily generalizable to populations in other states or nationally.
Autism is widely underascertained in the adult population and obtaining a diagnosis as an adult is often challenging 82 and likely differential by race/ethnicity, as evidenced by the lower proportion of Asian and Hispanic individuals in our autistic versus non-autistic samples. Although we do not expect that misclassified autistic adults in our non-autistic sample would have been numerous enough to lead to appreciable bias, this low ascertainment may further limit our generalizability to the wider adult autistic population.
Thus, our findings likely underestimate the health disparities that exist in the broader population of insured and uninsured autistic adults in the United States, many of whom experience employment and financial difficulty that can impede consistent health care access. 29
More work is needed to understand these patterns of health vulnerabilities at the intersection of autism and race/ethnicity,28,83 with attention to disparities in health care utilization and/or quality of care. Qualitative studies will also shed light on the barriers and facilitators beyond what is observable in the EHR, including autistic camouflaging in health care settings, patient awareness of psychiatric and medical symptoms and deciding when to seek care, patient perception of the efficacy of available mental health treatments versus non-medical treatments, patient–provider relationships including racial concordance, and self-advocacy.
Footnotes
Authorship Confirmation Statement
J.L.A. engaged in the conceptualization, data analysis, and drafting of the study. L.A.C. mentored J.L.A. and engaged in the study's conceptualization and design and interpretation of results. E.H.M. engaged in the interpretation and editing of the article. M.G.O. engaged in the interpretation and editing of the article. Y.Q. conducted the data extraction and contributed to the data analysis. M.L.M. engaged in the interpretation and editing of the article. All authors revised the article and approved of the final version for publication. The article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Working for Inclusive and Transformative Healthcare (WITH) Foundation (formerly the Special Hope Foundation) and the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under the Autism Intervention Research Network on Physical Health, award UT2MC39440. The information, content, and/or conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US Government. The funders did not participate in the work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.