
Abstract
As in the general population, autistic adults may need residential care in their old age. Little is known about the needs of older autistic adults in residential care, and how to support them within these services. Care homes for older people play a central role in their social, physical, and psychological well-being, and it is important to identify and understand what factors can contribute to this for autistic adults, who may have specific and unidentified needs. A researcher and two experts via lived experience identified key topics for inclusion in the first round of an abbreviated Delphi study. Twenty-six experts in autism, aging, and residential care completed the two-round Delphi study, which involved identifying and prioritizing key areas of interest, and generating and providing feedback on interview content. This co-creation process gave rise to the Autistic Satisfaction with Care Holistic Interview (ASCHI), a four-part interview schedule designed to be used with autistic adults in residential care homes. The ASCHI covers topics identified as being important to autistic adults living in residential care, including social time with others, daily routine, activities, environment, independence, advocacy, physical health, and well-being. The ASCHI is an open access tool that can be used in future studies to explore the experiences of older autistic adults in residential care and help shape future research, practice, and policy.
Lay summary
Why was this study done?
As in the general population, autistic adults may need residential care in their old age. Little is known about the needs of older autistic adults in residential care, and how to support them within these services. Care homes for older people play a central role in their social, physical, and psychological well-being, and it is important to identify and understand what factors can contribute to this for autistic adults, who may have specific and unidentified needs.
What was the purpose of this study?
To learn more about the experiences of older autistic adults who live in residential care, we co-created an interview schedule called the Autistic Satisfaction with Care Holistic Interview (ASCHI).
What did the researchers do?
We worked with autistic people, their families and allies, researchers, service providers, and clinicians to co-create this interview. This involved finding out about what their priorities were in relation to residential care for older adults, then finding out which questions mattered to them most, and which questions were most accessible to be used in an interview with autistic adults.
What were the results of the study?
The authors created the ASCHI tool, which can be used in future research to find out more about what residential care is like for older autistic adults, and which areas of services are not meeting their needs. This can, in turn, be used to inform policy and practice in residential care services, improving the quality of life of older autistic adults.
What do these findings add to what was already known?
Currently, there are no research tools to find out what residential care is like for older autistic adults. We have worked with the autism community to create a new tool so that future researchers can learn more about older autistic adults' experiences of residential care.
What are potential weaknesses in the study?
Due to limited resources, we have not been able to pilot test the interview with older autistic adults in residential care yet; however, we have published the interview under an open access license to allow researchers in the future to make the adaptations needed when using the interview. Also, the interview has been designed for autistic adults who use verbal language and are able to consent to taking part in research, and so its design limits participation to this subgroup of autistic people.
How will these findings help autistic adults now or in the future?
This study provides a new tool to help researchers learn about what residential care is like for autistic people. This means that in the future, we will be able to understand what areas of support need more research and development to improve the care and lives of older autistic people.
Introduction
In the United Kingdom, the largest area of population growth is in adults aged older than 60 years, 1 and this trend brings with it challenges for health and social care services to meet the needs of a rapidly expanding number of older adults. Health and cognitive capacities almost inevitably decline in later life, and for 3.5% of UK older adults, this has resulted in living in residential care homes. 2 Satisfactory standards in residential care are a basic requirement of good quality of life for people who are not living in their own home. An increasing number of autistic people will enter old age in the coming decades, in part due to a rise in the number of children and young adults who have received an autism diagnosis in recent years. 3
A recent workshop to set priorities for research into autism, physical health, and aging highlighted the need for investigation of autistic people's use and experiences of residential care. 4 A range of common elements of the autistic experience may make moving into, and living in residential care especially challenging for autistic people, for example, having a social and communication profile that differs from the neurotypical model, experiencing sensory sensitivities, and disliking transitions and change. 5 As in the general population, as autistic adults grow older, they may need residential accommodation to support declining physical or mental health. This includes autistic people who already live in residential or supported settings and may need to move into a different kind of service as they get older and their needs change.
Very little is known about older adults' experiences of transitioning to and living in residential care, and the standard and suitability of existing residential care services for older autistic adults has yet to be explored. 4 One of the fears expressed by autistic people who live independently is that should they need to enter a generic residential care home, they are likely to find little understanding of autism, and no autism trained staff or autism adjustments. 6 This fear may be well founded—while we do not have data on the knowledge level of staff working in care for older people, certainly, there is evidence that a range of generalist practitioners such as GPs and teachers do not have good autism knowledge or training.7,8
In the general population, transition to residential care is often a result of acute health crisis and the absence of family support. A significant percentage of autistic adults are supported by aging parents, who will reach an age where they can no longer manage: many of these aging autistic adults will then most likely rely on residential care. 9 Older autistic adults have significantly poorer health than the rest of the population 10 and be at higher risk of a multitude of medical conditions, 11 with a recent study finding that autistic adults experience high prevalence of deafness and hearing loss (17.5%), blindness and sight loss (12.1%), mental health conditions (33.00%), and physical disability (30.7%). 12 These co-occurring conditions may result in a higher than average number of autistic people requiring residential care services in old age. For autistic people with learning disabilities who are already in lifelong residential care, a transition to a generic care homes in their old age may still apply. This may be because their existing care home is not licensed to support people aged over a certain threshold, or because commissioners may move people into a cheaper nonspecialist service when a lower age-limit eligibility criterion is met. For both groups (moving from home or from another residential care setting), support designed for generic physical and cognitive health deterioration in old age may not meet their autistic needs.
It is possible to improve the well-being and quality of life of nonautistic older adults in residential care through specialized worker approaches and targeted training, 13 and it is possible for older people to thrive in residential care. 14 However, the specific needs of autistic adults transitioning to residential care are as yet unknown, coupled with the fact that moving into residential care is a big transition requiring major adjustments to environment and lifestyle. 15 There is a lack of knowledge and understanding about the needs of autistic older adults in general: there is a conspicuous scarceness of studies following autistic adults into middle age and beyond and even less research relevant to older autistic adults.6,16–18 A small body of research into autism in older age suggests that many cognitive skills (including executive, memory, and speed of processing) show a similar pattern of decline as in neurotypical aging19,20; however, older autistic adults show reduced visual memory differences compared with neurotypical older adults and reduced theory of mind impairments compared with younger autistic people. 21 However, this research is limited by the heterogeneity of autism, the suitability of standardized assessments for autistic adults, and varying environmental factors that may play a role in lifelong outcomes, 22 as well as by the cross-sectional designs used and relatively low sample sizes. Older autistic adults have prioritized the need for future research to focus on long-term support and care in the community rather than etiology and treatment. 23 There is clearly a pressing need for more research into the care and support provisions made for older autistic people as more people diagnosed with autism reach the age where they need residential care. Currently used interview scripts for use in residential care services do not include questions likely to be of relevance for autistic older adults, and thus, their use with this group may not unearth important themes specific to their experiences.24,25
Capturing the experiences of older autistic adults in care is an essential part of any such research. This is challenging: even when informants have been able to express their wants and needs through speech, or assisted communication, in the past, this ability may have declined with older age. Written measures such as questionnaires and surveys are not easily adapted to changing communication profiles, while independent observation cuts out the direct perspective of the autistic person. Therefore, following a multiperspective workshop discussion, 4 it was decided that an interview schedule would provide the best way to start to capture the experiences of older autistic adults in residential care. Here, we describe a two-phase Delphi study to co-design and develop an interview schedule to be used with autistic adults aged older than 60 years who are living in residential care. The goal was to create a tool, which can be used to learn more about the experiences of older autistic adults in residential care: whether the environment and support around them meet their needs and provide them with the tools for an autonomous, comfortable, and meaningful life. We anticipate that future researchers can use this method to create a picture of what life is like for older autistic people in residential care, and in doing so, create greater understanding of what specific support they may need, which in turn can inform staff training and service guidelines.
Methods
The design approach
An abbreviated Delphi method was used 26 to iteratively derive an evidence-based interview tool from expert opinion. The Delphi process involves collecting and distilling the anonymous judgments of subject experts through data collection and analysis and is suited to developing psychological tools or measures where there is limited background information about a phenomenon.27,28 Typically, a Delphi study involves 15–30 participants who are experts in their discipline.29,30 The number of participants varies according to the complexity and purpose of the study, although increasing the number of participants beyond 30 has not been found to improve results.31–33 The structure of this Delphi study is outlined in Figure 1. Participants were older autistic adults, their children and siblings, care service providers, researchers, and health care practitioners recruited through professional networks and through recommendations from the autism community (Table 1). Over two phases of a web-mediated co-design process, they created and refined interview questions about autistic experiences of residential care for the older, arriving at the most important and accessible questions for older adults. These questions are designed to be used in future research with relevant stakeholders.
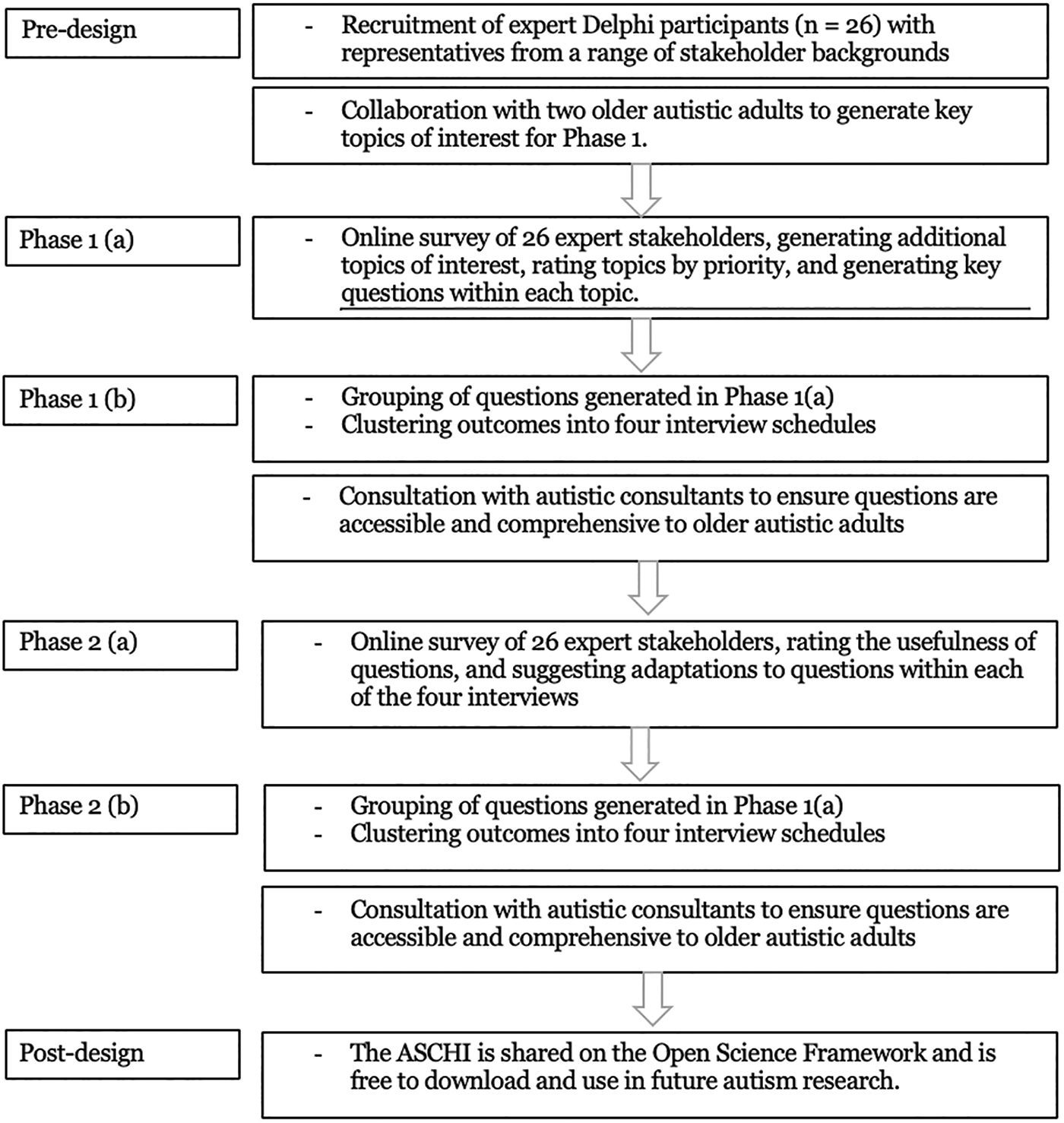
The interview design process using a reduced Delphi method.
Phase 1 Participant Backgrounds and Number from Each Background, N = 26
This research was reviewed and approved by the University of Edinburgh Psychology Research Ethics Committee. Each participant gave informed consent to participate in both waves of the study.
Predesign phase
As very little research has been carried out in this area before, a predesign discussion took place to identify key topics to be included in the Delphi Phase 1. This discussion involved the first author in direct consultation with two autistic advisors, both aged older than 50 years, with extensive community links. They identified and generated eight key topics to be covered in an interview with older autistic adults in residential care. These topics were as follows: appropriateness of the physical environment; comfort of the sensory environment; physical health care; advocacy and managing potential decline in capacity; social interaction within and beyond the residential care setting; self-determination, autonomy, independence, and choice; hobbies, interests, and expertise; and food, fitness, and hygiene. In addition, some topics included a number of subtopics (Table 2): for example, the topic “appropriateness of the physical environment” incorporates comfort of surroundings, activities, and safety and privacy.
Phase 1b Themes and Example Questions Generated for Each Topic
Phase 1: Prioritizing topics and generating questions
The first research phase was designed to generate and gather ideas for interview questions from relevant stakeholders.
The design of this phase was exploratory and used mixed methods: participants were asked to quantify the importance of topics (identified during the predesign discussion) on a rating scale and to generate questions to be analyzed thematically. The research questions for this phase were:
What are the key topics for research into autistic adults' experience of residential elder care? Which of these key topics are priority areas to be included in a research interview? What are the questions generated by community stakeholders to explore these key topics?
Participants
Twenty-six stakeholders from relevant backgrounds were recruited to participate in this study. All participants took part in both phases of the Delphi study, and there were no missing data. Participants were recruited through recommendations from the autism community for those with relevant expertise and experience to ensure representation of those with a range of support needs. Although many participants met more than one relevant background (e.g., were both an older autistic adult and a sibling of an older autistic adult, or were both researcher and had worked in residential care services), their primary background is listed in Table 1.
Materials and procedure
Each participant completed an online survey, administered through Qualtrics over a 2-week period, in which they were asked to rank each of the topics generated in the predesign phase by priority, before suggesting any additional topics that they felt should be covered in an interview schedule. They were then asked to provide examples of the specific questions that they would ask an older autistic person in residential care to gather information about each of the topics.
Results: Prioritization of topics
Participants ranked each of the eight key topics, from highest priority to lowest priority, with one indicating the most important topic and eight indicating the least important topic (Fig. 2). Self-determination, autonomy, and choice was highlighted as the most important (mean rating = 2.26), followed by physical health and health care (3.65), advocacy and managing decline in capacity (4.13), appropriateness of the physical environment (4.26), sensory environment (4.65), food, fitness, and hygiene (5.48), hobbies, expertise, and interests (5.52), and social interaction within and beyond the home (6.04).
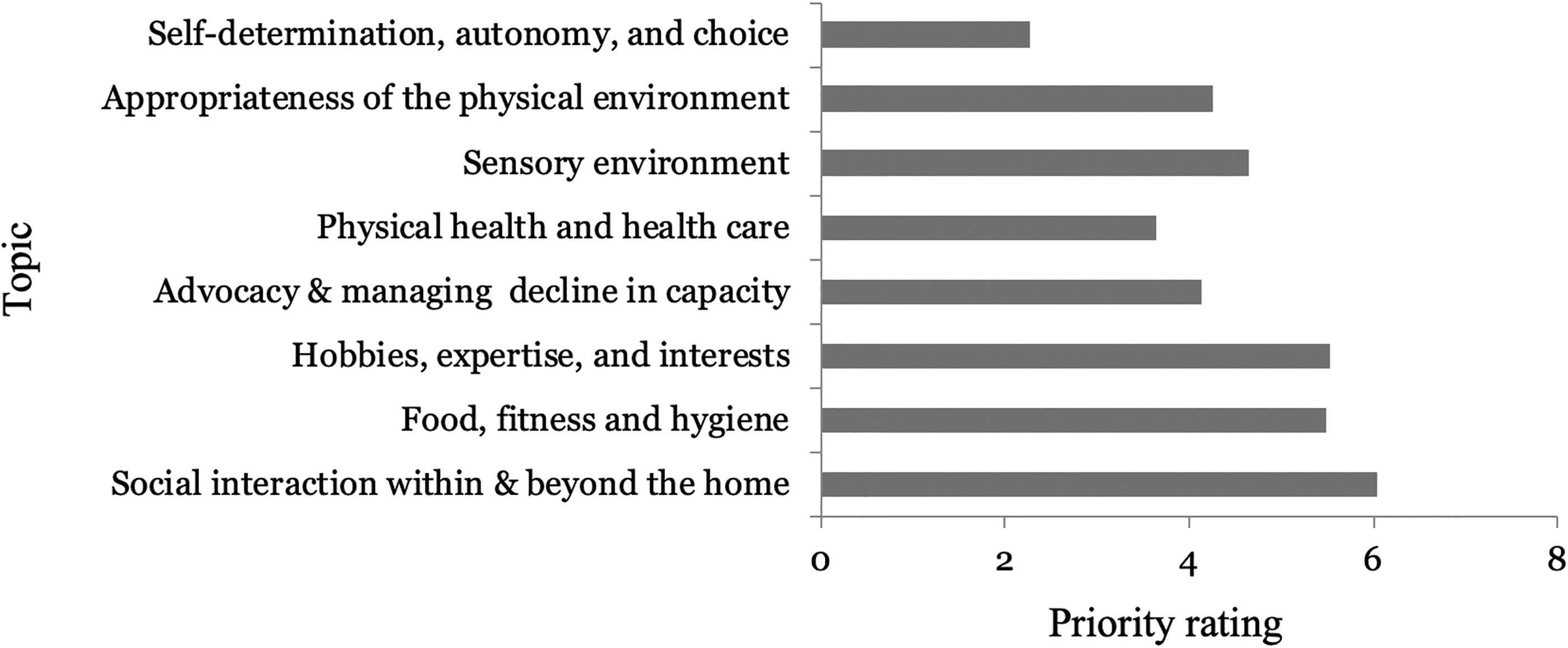
Mean priority ratings for the right interview topics, ordered by mode: 1 indicates highest priority, 8 indicates lowest priority.
Additional topics
When asked to suggest other key topics for inclusion in the interview, multiple (in each case, five or more) participants suggested the suitability of the geographical location, staff training, and end-of-life planning, and were given the opportunity to generate specific questions for these topics. These topics and questions were included in the second phase.
Generated questions
Participants had the opportunity to propose sample questions for each predefined topic. Proposed questions were labeled by the first author to indicate the content of that question. For example, physical health care includes question labels such as “current medical conditions,” “accessibility of healthcare,” and “future planning.” In many cases, multiple participants proposed new questions, which fell within the same label and had closely overlapping wording, in which case the first author constructed an archetypal question from the participants' submissions. Table 2 lists all the questions generated in this way, including those proposed by just one of the participants. These are presented within the a priori topic and subtopic structure, alongside their researcher-defined label.
Following review of these participant-generated questions, and new suggested topic areas, the interview was restructured into four, linked interview scripts, with the original topics and new topic areas grouped into (1) daily activities and spending time with others, (2) environment, (3) independence and advocacy, and (4) physical health and well-being. After this, two autistic consultants edited the wording of the questions to be more accessible for autistic people. The resulting set of four linked interviews with edited questions was presented to participants in Phase 2.
Phase 2: Refinement of topics and questions
The second research phase was designed to refine the topics and questions included in the interviews to design a tool that yielded useful information about the experience of older autistic adults and to ensure that this tool was usable by researchers and accessible for informants. This phase again involved mixed methods: participants were shown the list of questions collated from Phase 1, asked to numerically rate how useful they thought each block of questions were, before suggesting edits, additions, or removal of individual questions. The research questions for Phase 2 were:
What are the most useful topics to include in an interview tool to investigate the experience of older autistic adults in residential care?
Within each of these topics, what is the best way to frame and present the interview questions to maximize accessibility for informants?
What are possible ways to adapt this tool for future use with informants with learning disabilities, who are nonverbal, or unable to articulate their preferences?
Participants
The participants from Phase 1 also completed Phase 2.
Materials and procedure
Each participant completed five mini online surveys administered through Qualtrics over a 2-week period: one based on each of the four interview schedules and one that focused on suggestions for adaptations to be made to the interviews to enable the future participation of older autistic adults with learning disabilities. In each of the first four surveys, participants were asked to rate whether they thought the questions would elicit useful information on a 1–10 scale (not useful to very useful). They were then asked to edit, delete, or add questions in each topic area to create their suggested version of each interview.
Analysis methods
Quantitative responses were collated, and descriptive statistics generated to show participants rating of perceived usefulness of each set of questions. Qualitative responses were analyzed through a “rapid assessment” version of thematic analysis, labeling and identifying overlapping content between open-ended responses to the survey, and merging this into new content, which represented the common theme.34,35
Results: Quality of interview questions
Participants were asked to rate how useful the existing questions were at eliciting meaningful responses from autistic adults in their current format, before suggesting improvements for the questions. Ratings were out of a maximum of 10, and an a priori mean threshold of 7 was set to indicate good endorsement of an item and its inclusion in the interview, in line with a 0.7 threshold indicating good reliability using Cronbach's alpha. 36 Participant ratings of the questions are shown in Table 3, with all questions scoring above the threshold of 7, and therefore, all question areas were included in the final interviews.
Participant Ratings of Interview Questions in Round 2
Qualitative input
Participants provided re-worded and re-framed suggestions for questions which they recommended be re-structured. These suggestions were analyzed and grouped by the first author as in Phase 1 and used to create the final version of the four-part interview, shown in the Supplementary Data and available open access at https://osf.io/3m8gh
The finished interview
The finished interview has four component interviews. Interview 1, “Daily Life,” explores the important people in the informant's life and the time they spend together, as well as daily routine and hobbies. Interview 2, “Environment,” asks about comfort in the surroundings, including personal space, shared spaces, moving around the home, and access to the wider community. It also asks about the sensory environment and how suitable and pleasant it is for the informant. Interview 3, “Independence and Advocacy,” investigates how much control the informant feels they have over their life, and the presence and role of advocates. Interview 4, “Physical Health and Well-being” covers current physical health, the provision of autism appropriate health care and health autonomy, as well as food, fitness, and hygiene. Phase 2 results indicated that these topics are all high priority for inclusion in future research with older autistic adults. Throughout the interviews, language has been designed to be as accessible as possible to older autistic adults.
Adaptations for accessible versions
Our final research question asked Delphi participants to propose possible adaptations for the interview so it could be used with informants with learning disabilities or who do not express themselves verbally. We asked participants to suggest methods of adapting the interview in the future to create accessible versions. Their suggestions are outlined in Table 4.
Methods of Adapting the Interview for Future Use
Discussion
This article has reported on the development of an interview schedule designed to be used by researchers to capture the experiences of older autistic adults in residential care. Our goal has been to describe the process involved in the design of this interview, and how we have integrated the views and concerns of relevant stakeholders during this process to create a research tool that aligns with their priorities. A range of expert stakeholders including older autistic adults, the children and siblings of older autistic adults, staff and leaders from elder and autistic residential care services, researchers, and physicians all played a key role in the design process, with autistic adults guiding the earliest design decisions, and included in key leadership roles within the study. This process was essential to ensure that the interview directly addresses areas of key importance to the autism community and can yield information about an underresearched and undersupported group. Future research using this interview will elicit rich qualitative data covering key areas of life for autistic adults in residential care, which will help services and policymakers understand how they can be best supported.
We anticipate that, when used in future research studies, these four interviews would be carried out in separate sessions and would recommend that they are part of a six-session, flexible participation process, where the first session involves introductions, consent, and familiarization with the residential service, sessions two to five involve one of each interview, and the final session is used to share any additional information that the informant would like to, and to answer any final questions.
This interview differs from most interview scripts exploring the needs of older adults in residential care,24,25 as it incorporates specific concerns important and relevant to autistic adults, including the sensory environment, communication, and particular interests and hobbies. It also addresses experiences of social interaction, and whether preferences for this are respected within the residential care service. This may be particularly important to autistic adults: since older adults can experience loneliness and isolation,37,38 residential homes often encourage social activities. This may not always be welcome, as autistic people may particularly value time alone, away from the effort often involved in being with other people. This interview seeks to provide information about the needs of autistic older adults: where they diverge or converge with the known needs of older people from the general population.
Limitations
The abbreviated Delphi design involved a relatively small number of expert participants, and only two rounds of feedback, which may have limited the range of topics and questions identified. However, given the variation in participant backgrounds and the high proportion of autistic adults within the group, representation should be sufficient for the creation of an accessible and meaningful research tool. Certainly, there was considerable agreement within the group and the resulting set of four interview scripts covers a wide range of topics in substantial depth. The creation of the ASCHI is the first stage of a development process, which may be adapted and edited in the future as a knowledge base about the experience of older autistic adults is developed.
While autistic people with high support needs (including as a result of aging) were not included in this research, we did include proxy representatives for this population.
The interview has not yet been piloted, due to limited resources and capacity, and there is a need for further research and testing with potential consequent modification. The interview has been published under an open access license to facilitate this. Future evolutions and adaptations of the interview may happen and could include a questionnaire version with rating-scale responses, exploring its potential for use in internal service evaluations, or adapting it for use with those who receive support from a care worker at home. Additional items could be added if deemed necessary following future work, for example, the ASCHI does not currently include questions about mental health, partly because other measures are available, but these, or others, could be integrated in the future.
This interview has been designed for autistic adults who use verbal language (including nonverbal equivalents such as text-to-speech devices) and are able to consent to taking part in the study, and so its design limits participation to a subgroup of autistic people. As a result, findings from the interview may only be relevant to this subgroup. However, as part of the process, we asked experts for their suggested methods for adapting the interview to increase accessibility and have provided these suggestions here. We hope this provides a springboard for further, more broad-based research, as there is a growing and urgent need to provide effective care for the aging autistic population, until it matches the standard of support expected by the general population and oversight bodies. Our evidence-based approach means that the key topics identified during the process should be relevant to most autistic older adults and so can be applied to other methods.
Conclusion
Creating evidence-based guidelines and policy for care and support for older autistic adults requires research; and this research should align with the priorities of the autism community. In creating this research tool, we are initiating the first methodology for gathering evidence of the experiences of autistic older adults in residential care. By reporting on the process of creating this interview, we hope to have a broader impact on the future design of research and guidance tools for autism research and practice.
Footnotes
Acknowledgment
The authors would like to thank the range of anonymous expert contributors for the input into this process.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a Collaborative Research Grant (grant reference 7259) from Autistica to the authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.