
Abstract
Coenzyme Q10 (CoQ10 or ubiquinone) is an essential component of the mitochondrial electron transport chain and is also present in various cellular membranes and in plasma lipoproteins. Diabetes, cardiovascular, neurodegenerative, and preeclampsia diseases are all associated with an alteration of CoQ10 level or its redox status. During pregnancy, we note that the plasma content of CoQ10 is significantly higher than amniotic. In the fetal growth restriction group, amniotic total CoQ10 levels were significantly higher versus healthy, while the amniotic oxygen radical absorbing capacity level was significantly lower. A significant negative correlation was observed between amniotic total CoQ10 and birthweight. Our observation leads to the hypothesis that the amniotic midtrimester CoQ10 content may be a marker of subsequent obstetric complications. Antioxid. Redox Signal. 21, 1582–1586.
Introduction
P
This study investigated whether amniotic fluid CoQ10 levels could be altered earlier in pregnancies that subsequently were complicated.
Oxidative stress induced by reactive oxygen species has been implicated in many obstetric complications. This is the first report on Coenzyme Q10 (CoQ10) and oxygen radical absorbing capacity (ORAC) in midtrimester amniotic fluid. Overall CoQ10 amniotic fluid levels were nearly 10-fold lower than those found in maternal plasma with, on the other hand, the ORAC levels significantly lower. The concentration was related to pregnancy outcomes, and a negative correlation was observed between amniotic total CoQ10 and birthweight.
Results
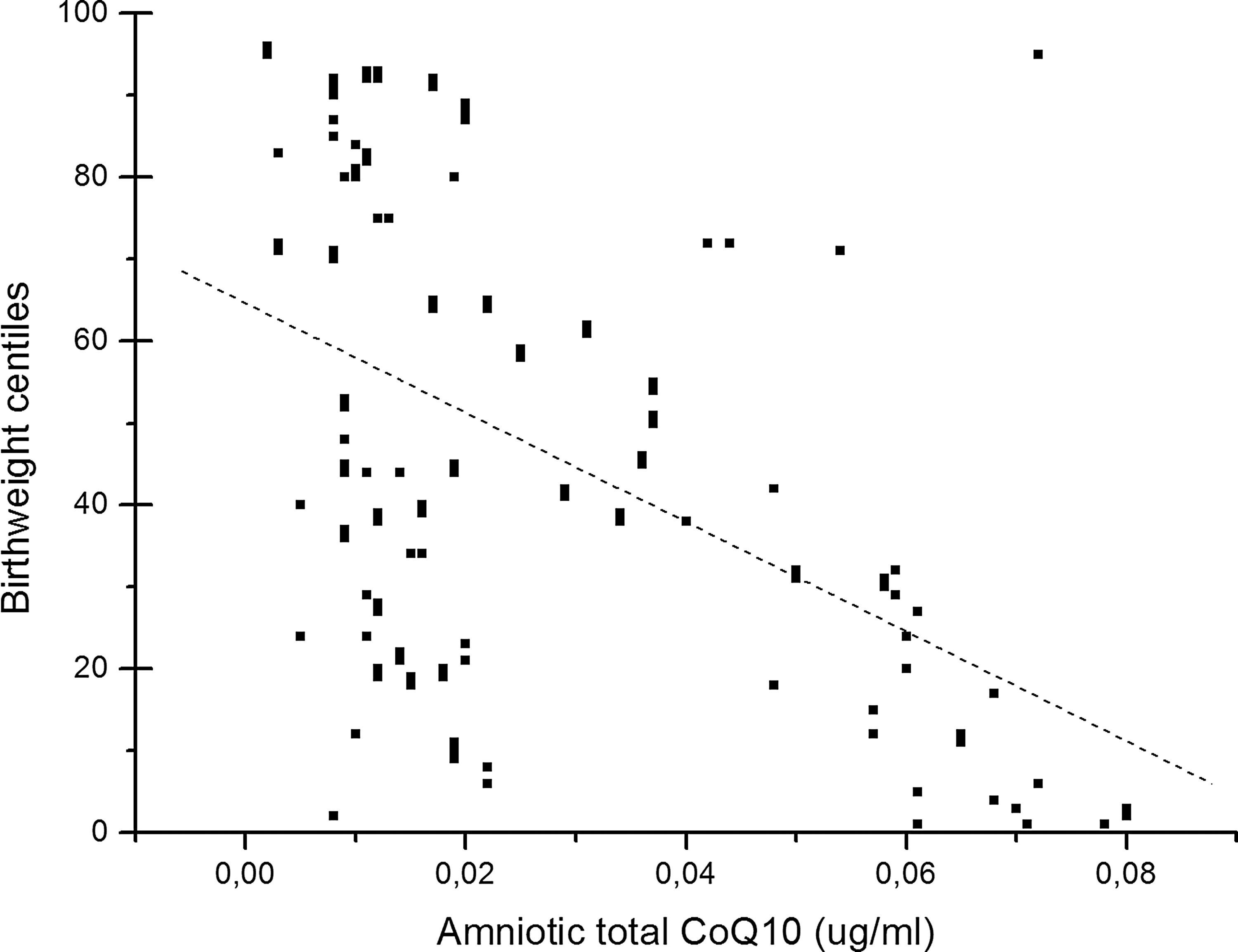
Table 1 presents the demographic, clinical, and nutritional characteristics of the groups studied. In the prospective cohort study, 204 patients were enrolled; complete data were available for 197 subjects. Exclusions included termination of pregnancy for chromosomal abnormalities, miscarriage after amniocentesis, delivery of a malformed newborn, and unknown pregnancy outcome. Among the 178 remaining patients who met the inclusion criteria, 139 women delivered at term after an uncomplicated pregnancy (Controls); 19 women experienced gestational diabetes mellitus (GDM), 11 women had fetal growth restriction (FGR), and 9 women delivered preterm after a pPROM. Table 2 shows CoQ10 and its isoform levels in plasma and amniotic fluid in relation to the outcomes of pregnancy. In the group of women who will develop FGR, the midtrimester amniotic fluid total CoQ10 levels were significantly higher versus healthy controls (0.05±0.06 vs. 0.012±0.007 μg/ml; p<0.001). In the same group, the amniotic oxygen radical absorbing capacity (ORAC) level was significantly lower than controls (1.02±0.31 vs. 1.65±0.48; p<0.05). In the group of women who will experience pPROM, plasma levels of CoQ10 in its oxidized form were higher than controls (0.14±0.08 vs. 0.07±0.03 μg/ml; p<0.05); in the same way were significantly higher also plasma CoQ10 oxidized/total ratio and plasma CoQ10 oxidized/reduced ratio (Table 2). In this group, no differences were registered for amniotic CoQ10 and ORAC. In the group of women who will develop GDM, no differences were found for plasma and amniotic levels of CoQ10 and ORAC. In all the groups studied, the plasma content of CoQ10 was always significantly higher than amniotic. A significant negative correlation was observed between amniotic fluid total CoQ10 levels and neonatal birthweight by data analysis of the whole population studied (r=−0.49; p<0.001) (Fig. 1).
Data are expressed as mean ± standard deviations.
FGR, fetal growth restriction; GDM, gestational diabetes mellitus; pPROM, preterm premature rupture of membranes.
p<0.05.
p<0.001 versus controls.
CoQ10, Coenzyme Q10; ORAC, oxygen radical absorbing capacity.
Discussion
Oxidative stress may have a role in several obstetric complications such as embryopathy from diabetes or substance abuse, pPROM secondary to bacterial infection or other insults, labor, FGR, and preeclampsia (6). In this study, we analyzed not oxidative stress, but the antioxidants in terms of total antioxidant power expressed as ORAC and in terms of CoQ10. Very few reports described CoQ10 in amniotic district during pregnancy (8). The main results of this small prospective study are that the overall CoQ10 amniotic fluid levels were nearly 10-fold lower than those found in maternal plasma; CoQ10 levels are significantly higher in the midtrimester amniotic fluid of women who will develop FGR later in pregnancy with, on the other hand, the ORAC levels significantly lower. The biologic significance of the increased CoQ10 levels is unclear. Oxidative stress and levels of redox-related molecules have reported increased FGR placentas (8). FGR, in fact, is associated to intrauterine hypoxia and impaired blood flow to the fetus; thus, chronic restrictions in uterine blood flow and the relative hypoxia may induce free radical generation and fetal oxidative stress. The link between hypoxia and oxidative stress is well documented and the evidence includes studies that identified increased biomarkers of oxygen free radical damage and reports that found abnormalities in the antioxidant defense of fetuses. Longini et al. found elevated isoprostane concentrations, as markers of oxidative stress, in the amniotic fluid between gestational weeks 15 and 18 of pregnancies with subsequent FGR (3). In our series, a high CoQ10 content in amniotic fluid may be interpreted as a compensative mechanism, again a higher oxidative stress in the absence of an antioxidant power suggested by low ORAC levels.
In this sense, the elevation of CoQ10 may be the response to an ambient excessive oxidative stress and is very interesting the negative correlation between amniotic fluid total CoQ10 content and birthweight found in the whole pregnant population studied. Regarding women who will develop gestational diabetes, this study confirmed our previous observation that maternal plasma CoQ10 is increased only in the late pregnancy (36–40 weeks); no differences were registered in amniotic fluid content. Even if some reports indicate that subclinical inflammation may start at midtrimester, as reflected by elevated levels of interleukin-6 (IL-6) in amniotic fluid samples from asymptomatic patients who subsequently delivered at <34 weeks of gestation (9), in our series, in women who will experience pPROM, the plasma CoQ10 levels, not amniotic levels, are increased in its oxidized form. The relevance of this finding is yet to be determined in future studies.
In summary, the amniotic fluid CoQ10 content may change in relation to obstetric outcomes, in particular is the strong association to fetal growth. As an antioxidant, CoQ10 production may work to restore the homeostasis in an ambient oxidative stress, not balanced by other antioxidant factors. In light of the presented results, the role of CoQ10 in response to maternal/placental/fetal pathophysiology and as a predictive marker of later complications needs to be further investigated.
Notes
Patients who underwent midtrimester genetic amniocentesis at the Salesi Maternal-Child Teaching Hospital (Ancona, Italy) between July 2012 and December 2013 were asked to participate in the study. Before the data collection, the protocol of this cohort study was approved by the Institutional Review Board, and all women were informed before the procedure and they provided their written consent.
A 5-cc sample of amniotic fluid was obtained through routine midtrimester amniocentesis, performed between 16 and 19 gestational weeks for various indications, including advanced maternal age, abnormal nuchal translucency screening, abnormal triple test, past history of a genetic disorder, and/or detection of an abnormality on second trimester ultrasound. The same experienced operator performed all amniocenteses using a 21-gauge spinal needle with the free-hand technique, under ultrasound guidance. Each amniocentesis was preceded by a detailed ultrasound scan to assess the fetal anatomy and determine the location of the placenta. In patients with anterior placenta, the thinnest portion of the placenta distant from the cord insertion was selected as the site for needle insertion. The gestational age was assessed either by the last menstrual period or by an early ultrasound scan if there was a discrepancy of more than a week. Amniotic fluid after collection was stored frozen at −80°C and thawed for 15 min at 37°C just before use. A 10-cc blood sample was concomitantly obtained from all patients recruited at the antecubital venous puncture site, immediately transferred into a polypropylene vial containing 3.15% sodium citrate (1:9, v/v), and then centrifuged at 4°C. The plasma obtained was decanted into 500-μl aliquots and then stored at −40°C until biochemical analysis. During processing, both plasma and amniotic fluid samples were protected from light using aluminum foil to prevent photodegradation of ubiquinones.
Demographic data were collected: age, smoking use, body mass index, and complete medical and obstetric records until term of pregnancy. Regarding possible pregnancy complications, preterm birth was defined as a spontaneous onset of labor with preterm delivery, between 24 and 36 weeks, 6 days of gestation age; pPROM was diagnosed, between 24 and 36 weeks, 6 days of gestation age, on examination by a sterile speculum while obvious leakage of amniotic fluid from the cervical orifice and confirmed by a positive fibronectine test. GDM was diagnosed based on the results of a 3-h, 100-g oral glucose tolerance test following an abnormal result on a screening 50-g glucose challenge test (plasma glucose >7.8 mM, 1 h postchallenge); FGR was defined on the basis of a decrease in fetal growth, and serial antenatal ultrasound biometry predicting a fetal abdominal circumference below the 10th percentile for gestational age (±reduced amniotic fluid volume); the final inclusion in the FGR group was based on the delivery of an infant with a birthweight below the 5th percentile for gestation and sex (4).
CoQ10 determination
CoQ10 levels were assayed in plasma and amniotic fluid with use of a dedicated high-performance liquid chromatography system with electrochemical detector (Shiseido Co. Ltd., Tokyo, Japan). Mobile phases were as described (7). Pumps 1 and 2 were model 3001, auto sampler model 3033, switch valve model 3012, concentration column Capcel I Pak C8 DD, and separation column Capcel I Pak C18 AQ (all from Shiseido Co. Ltd.). A peculiarity of the system was the use of a postseparation reducing column (CQ reducing column [Shiseido Co. Ltd.]; 202.0 mm inside diameter) capable of fully reducing the peak of oxidized CoQ10. The oxidation potential for the electrochemical detector was 650 mV. Plasma and amniotic levels of CoQ10 were expressed as nanograms per milliliter (ng/ml).
ORAC determination
The antioxidant activity of plasma was assessed with the ORAC assay according to the method described by Gillespie et al. (1). Briefly, 150 ml of 0.08 mM fluorescein dissolved in 75 mM phosphate-buffered saline was added in each well of a 96-well solid black microplate, followed by 25 L of plasma previously diluted (1:200). After a 10-min incubation in the dark, 25 L of 147 mM 2,20-azobis-2-methyl-propanimidamide, dihydrochloride (AAPH) was rapidly added to each well by using a repetitive multichannel pipette, and the microplate was immediately placed in a microplate reader (Synergy HT; Bio-Tek, Winooski, VT). Fluorescence was recorded every 120 s for 3 h, using an excitation wavelength of 485/20 nm and an emission filter of 528/20 nm. The net area under the fluorescence decay curve (AUC) for each compound was obtained by data processing using KC4 software (Synergy HT; Bio-Tek). To determine the antioxidant activity, a 10 mM stock solution of Trolox was used as standard to construct a calibration curve in the range 0–200 mM. The ORAC levels were expressed as the concentration of Trolox equivalent to the AUC of each plasma sample.
Statistical Analysis
Data are represented as mean±SD. The significance of differences between two groups was assessed by Student's t-test, and the differences between multiple groups were assessed by one-way analysis of variance (ANOVA). Values of p<0.05 were considered to be significant.
Footnotes
Author Disclosure Statement
All the authors declare that they have no conflicts of interest.