
Abstract
Evidence-based HIV programming focused on populations at risk of HIV is critical for sustainable disease prevention. In response to the Tennessee Department of Health decision to reject federal HIV guidance, the present study examines the potential impact of Southern US states adopting policies that direct HIV prevention and testing efforts away from populations “disproportionately affected” (DA) by HIV toward populations “non-disproportionately affected” (NDA). Descriptive and projection analyses with publicly available data explored the influence of policies emphasizing NDA populations on HIV cases. Across the Southern US, DA populations (cisgender women, men who have sex with men, transgender persons, and people who inject drugs) represent the absolute majority (90%) of diagnosed HIV cases, whereas NDA populations (pregnant women, infants, first responders, and human trafficking victims) represent only a small proportion (2%) of diagnosed HIV cases. Estimated projections show avoidable HIV cases among DA populations in the Southern US alone could aggregate to over 32,000 by 2030 if prevention efforts exclusively concentrate on NDA populations, which approximates the current national annual incidence of 36,000 HIV cases. Prevention efforts aimed at DA populations compared with NDA populations could reduce new infections across the Southern US by 47% versus 1%, respectively, by 2030. Policies disregarding epidemiological data may hinder efforts to end the HIV epidemic, both regionally and nationally.
Introduction
In his 2019 State of the Union address, former President Trump announced an initiative known as “Ending the HIV Epidemic in the US” (EHE) with the goal of achieving a 90% reduction in new HIV cases by 2030. 1 EHE encompasses geographic focus areas for HIV across 48 counties, Washington, DC, and Puerto Rico and 7 states with substantial rural HIV transmission. 2 Of these geographic focus areas, 23 counties, 6 states, and Washington, DC are located within the “Southern Region of the US” as defined by the Centers for Disease Control and Prevention (CDC). 2 The Southern US has the highest rates of HIV of any US region and accounts for more than 50% of all HIV diagnoses 3 despite comprising only one-third of the US population. 4 As such, the Southern US has the potential to influence the direction of the national HIV epidemic.
HIV prevention programs are most successful when emphasizing populations at ongoing risk for HIV infection. 5,6 A central component of the EHE initiative is that HIV programming must prioritize those populations to meet EHE targets. Cisgender women, men who have sex with men (MSM), transgender people, and people who inject drugs (PWID) are disproportionately affected (DA) by HIV in the United States. In 2021, these groups collectively accounted for 94% of new HIV cases in the United States. 7
However, in January 2023, the Tennessee Department of Health (TDH) was prompted by the governor to propose a refocus of state-level HIV prevention, testing, and treatment activities toward groups non-disproportionately affected (NDA) by HIV, including pregnant women, infants, first responders, and human trafficking victims. 8,9 State officials also announced their decision to forgo nearly $9 million of CDC funding for HIV prevention, testing, and treatment activities. 8 Such politically motivated rather than science-based decisions could have compromised the health of populations at ongoing risk of HIV, but the CDC implemented a workaround by sending HIV prevention dollars directly to community-based organizations in Tennessee. 10 To date, the TDH has not reconsidered its position to reject CDC HIV prevention funding, which may also negatively impact the long-term sustainability of HIV programming, particularly among community-based organizations. Yet, coincidentally, the TDH recently announced an outbreak in Shelby County, Tennessee, where HIV rates have increased approximately 40% from 2018 to 2023. 11
Tennessee is not alone in disregarding federal guidance. Southern US states were among the first to reopen sooner than recommended by health officials during the COVID-19 pandemic and one of those states is currently flouting CDC guidelines in the midst of a measles outbreak. 12 These examples are part of a trend of Southern US states proposing to reject federal support for vital programs and services. 13 –16 This study explores how such a trend could affect HIV outcomes by quantifying the potential impact of programming that prioritizes NDA over DA populations in the Southern US. Although a previous analysis found that the TDH decision would increase HIV cases across the state, 17 we broaden the scope beyond Tennessee to the entire Southern US. We consider to what extent this shift would impact the 2030 EHE targets outlined in former President Trump’s EHE initiative and which populations and states would be most impacted.
Methods
This analysis leverages public data from AIDSVu, CDC HIV surveillance reports, and state departments of health from 2018, 2019, and 2021 to compare overall and future HIV cases among DA and NDA populations (2020 was excluded due to disruptions caused by the COVID-19 pandemic). The main sampling units are states in the “Southern Region of the US,” defined by the CDC. 18 Institutional review board approval was not required for this secondary analysis.
Our primary outcome variable is diagnosed HIV cases, disaggregated by population demographics within each state. State-level HIV case counts and new HIV cases for cisgender women, MSM, and PWID were obtained from AIDSVu. 9 Estimated cases for transgender persons were imputed from the CDC and US Census. 7,19,20 Black women, MSM, PWID, and transgender people were designated as DA populations in our analysis, based upon EHE implementation guidelines and CDC surveillance reports of populations at ongoing risk for HIV. Tennessee state officials proposed focusing HIV prevention efforts toward politically preferred populations such as pregnant women, infants, first responders, and human trafficking victims, whom we classify as NDA populations in our analysis. Data for NDA populations were collected from state-level health agencies and other sources.
Our secondary outcome variable estimates future HIV cases based on the HIV Optimization and Prevention Economics study as described by Chen et al. 21 The effective reproduction rate (Re) estimates the average number of additional infections introduced by a single individual in a partially infected population over their lifetime. A rate near 1.0 is considered endemic, and infection elimination requires a rate substantially below 1.0. Chen et al. estimate the Re for HIV in the United States at 0.92. 21
Statistical analysis
All data and projections are calculated using a 3-year average of HIV cases from 2018, 2019, and 2021. We compute the proportion of HIV cases among specific DA and NDA groups and subsequently summarize the total for both dichotomized populations in each Southern US state. Annual new HIV cases were estimated using a base rate that is held constant per year, with additive subsequent transmissions estimated on an annual basis. We classify subsequent transmissions as “avoidable” cases for our analysis since access to quality antiretroviral therapy (ART) treatment, along with other reproductive health services, can help people living with HIV avoid further transmission with an effectively “undetectable” viral load. 22 Annual avoidable cases were calculated by dividing Re by the average life expectancy of 28.7 years post-infection 23 in a partially (52.9%) treated population, assuming a mean age of 34.2 at year of infection (0.92/28.7 = 0.032). Each year’s avoidable cases were then used to calculate the following year’s additional cases using the annualized Re (e.g., 3-year average for DA populations is 16,824 × 0.032 = 539 additional cases included in the following year) for both DA and NDA populations. No deaths are estimated in our model since the 6-year window through 2030 is well below the anticipated 28.7 years of additional life expectancy for newly diagnosed individuals.
Finally, we compare annual new infections expected with current HIV programming—defined as the “status quo”—to varying degrees of emphasis in HIV prevention for DA and NDA populations. We projected annual HIV cases assuming that directing a given proportion of HIV prevention efforts toward certain populations would correspond to the same proportion of avoidable HIV cases being prevented within that population. The “status quo” was calculated as the 3-year average of new HIV cases for all states in the Southern US (18,959) plus annual avoidable cases in DA and NDA populations. Additional scenarios estimate the prevention of 100% of annual avoidable cases among NDA populations and the prevention of 20%, 50%, and 100% annual avoidable cases among DA populations by subtracting the proportions of either NDA or DA transmissions from the 3-year average of new HIV cases (18,959) respectively. Overall, these projections consider how the adoption of policies that direct HIV prevention and testing away from DA populations might impact progress toward 2030 EHE targets and, therefore, we did not conduct a formal cost analysis. Data were analyzed in Excel and visualized with Stata 16.1. 24
Results
Baseline results and descriptive trends
There were nearly a half-million (492,922) people living with HIV in the Southern US between 2018 and 2021, with a 3-year average of 18,959 new cases per year. The HIV rate per state/locality ranges from 0.12% (West Virginia) to 2.0% (District of Columbia), with an average rate of 0.43% across the Southern US.
Across the Southern US, HIV cases are most common among DA populations (Table 1). For nearly all states and the District of Columbia, HIV is most concentrated among MSM, accounting for 58% of new cases on average, except for West Virginia where more than half of all new HIV cases (51%) are among PWID. The regional 3-year average shows that 17% of new HIV cases occur among cisgender women, 9% among PWID, and 5% among transgender people.
HIV Cases by State and Population Groups
All of these values are based on the average of the latest surveillance data (e.g., 2018, 2019, 2021) and the sum of individual counts and percentages may not equal totals given rounding.
DA, disproportionately affected; MSM, men who have sex with men; NDA, non-disproportionately affected; PWID, people who inject drugs.
Table 1 also highlights that, among NDA populations, pregnant women accounted for the highest proportion of HIV cases (1%–2%). For all states, first responders represent 0% of cases. In all Southern US states, infants represent 1% or less of new HIV cases. All states and the District of Columbia have HIV rates of less than 1% for human trafficking victims.
Figure 1 highlights that DA populations make up the vast majority of all new HIV cases, ranging from 83% in Florida to 96% in Alabama, with a mean of 90%, whereas NDA populations account for between 1% and 2% of all new HIV cases across the Southern US.
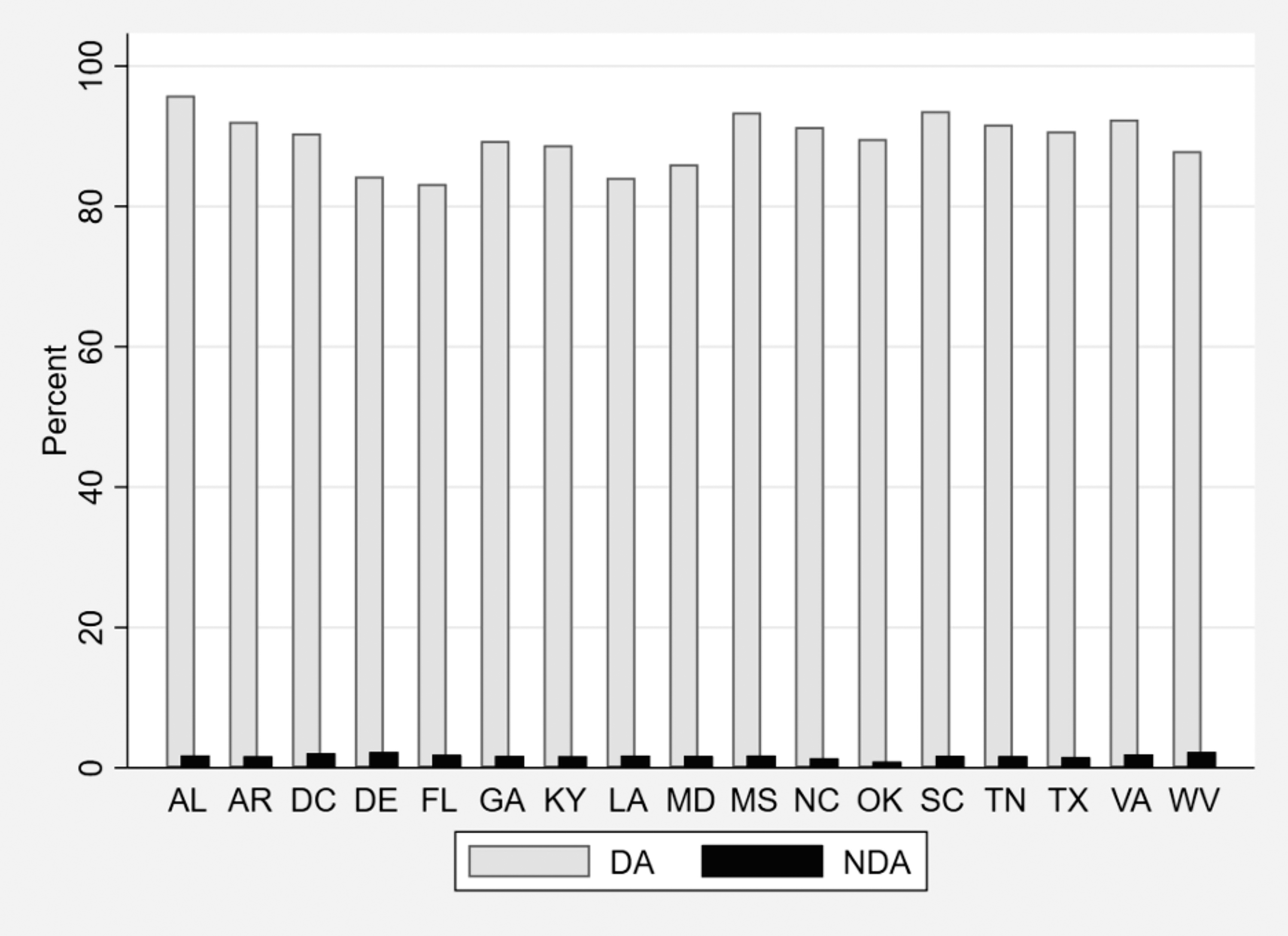
Percentage of mean new HIV diagnoses within each state in the Southern US attributable to disproportionately affected (DA) and non-disproportionately affected (NDA) populations, 2018–2021. All means are based on the 3-year rolling-average from 2018, 2019, and 2021 per state, summed across all groups for DA and NDA populations.
Projection of additional HIV cases through 2030
Figure 2 shows the exponential growth in avoidable HIV cases per year among DA compared with NDA populations. Avoidable HIV cases among DA populations could aggregate to 32,000 in the Southern US by 2030 if prevention efforts exclusively prioritize NDA populations. States with the most cumulative avoidable HIV cases in the South by 2030 among DA populations include Texas (24%, 7716), Florida (21%, 6773), Georgia (13%, 4212), North Carolina (7%, 2326), Virginia (5%, 1487) and Tennessee (4%, 1389) (analysis not shown).
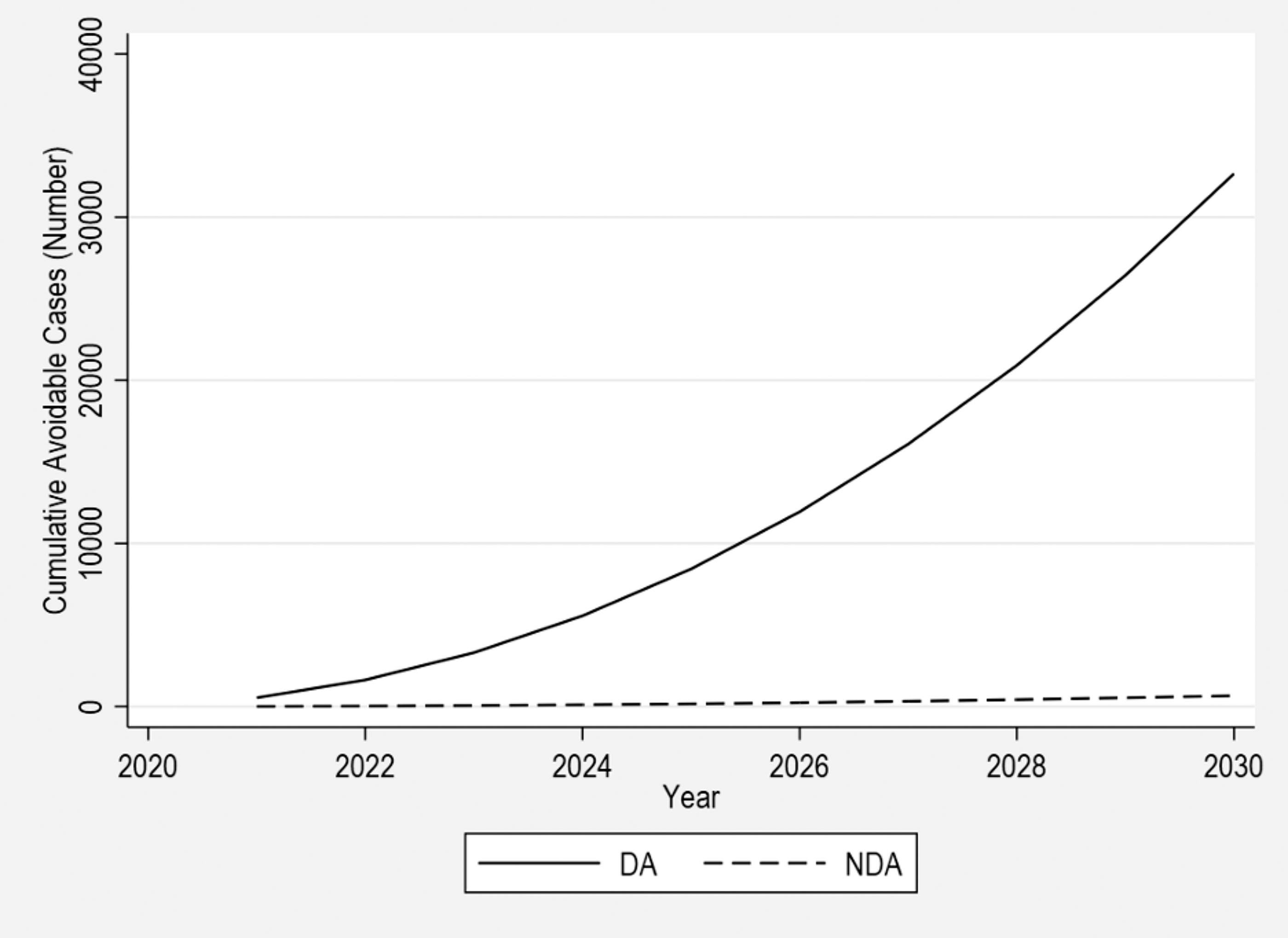
Estimated cumulative avoidable new HIV cases across all Southern US states among disproportionately affected (DA) and non-disproportionately affected (NDA) populations, 2021–2030. All cumulative, subsequent HIV transmissions—defined as avoidable cases—were calculated using an annualized reproduction rate and projected for DA or NDA populations to assess the avoidable cases that each group contributes from 2021 to 2030.
Figure 3 explores the effect of several HIV prevention scenarios on new HIV cases across the Southern US, including directing 100% of prevention efforts toward NDA populations compared with 20%, 50%, and 100% prevention efforts toward DA populations. Elimination of all annual avoidable cases among NDA populations only reduces the total number of new HIV infections by 1% by 2030. Meanwhile eliminating 20%, 50%, or 100% of annual avoidable cases among DA populations reduced total new HIV infections by 2030 across the Southern US by 27%, 35%, and 47%, respectively.
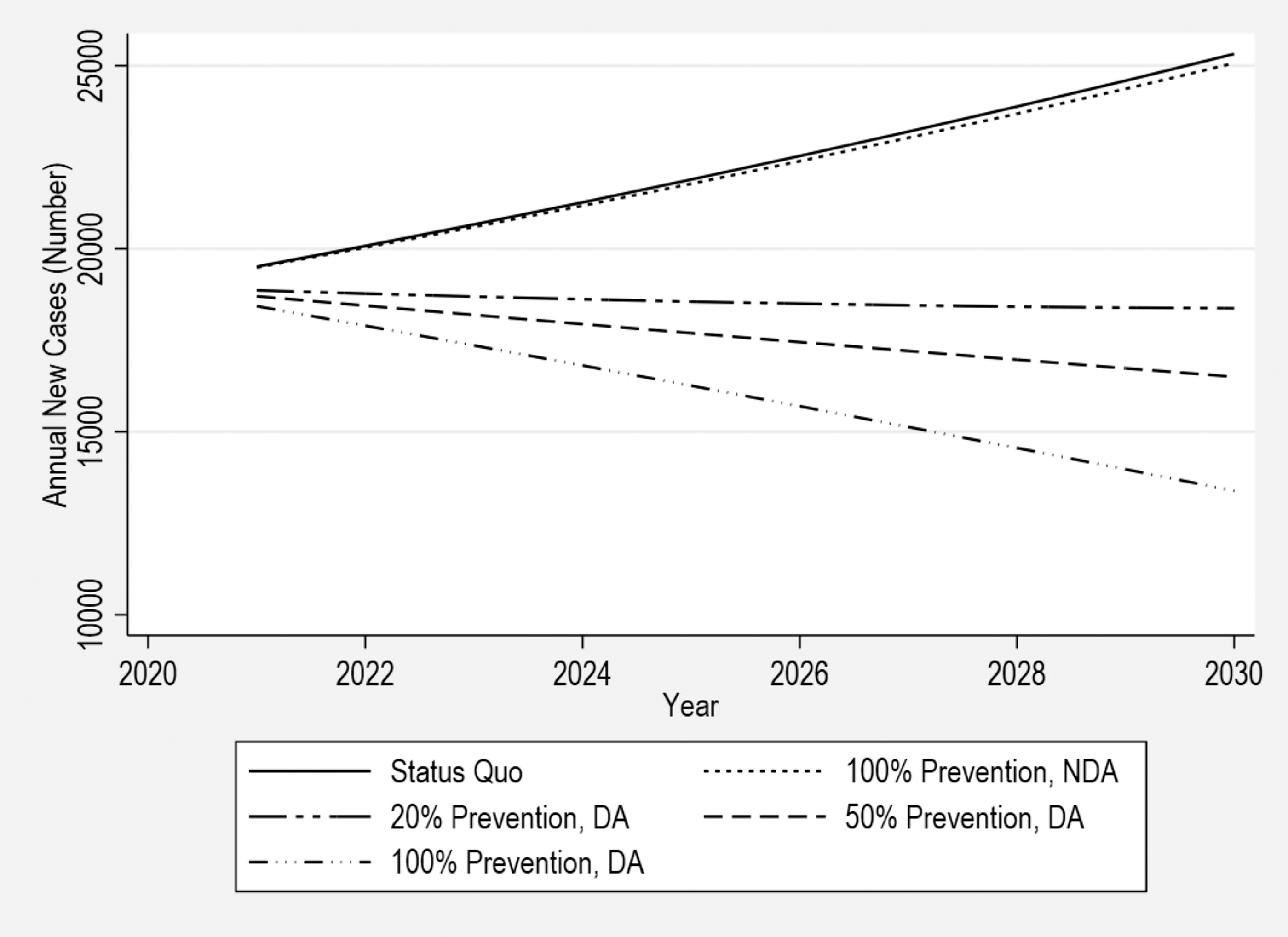
Projected annual new HIV cases across Southern US states by degree of prevention emphasis on disproportionately affected (DA) and non-disproportionately affected (NDA) populations, 2021–2030. All annual new HIV cases from 2021 to 2030 were projected at the levels of 20%, 50%, and 100% prevention of annual avoidable cases among DA populations with a counterfactual analysis examining 100% prevention of annual avoidable cases among NDA populations. The status quo was based on expected annual new HIV cases with current programming.
Discussion
Our analysis is the first to show how redirecting HIV prevention efforts as proposed by Tennessee could increase HIV cases across the Southern US and nationally if other states follow suit. Failure to focus HIV prevention efforts on DA populations could produce an estimated additional 32,000 avoidable HIV cases in the Southern US by 2030, which is nearly comparable to current annual HIV cases for the entire US, estimated at 36,000 per year. Moreover, we show that directing HIV prevention efforts toward DA populations (even marginally) would substantially reduce the trajectory of the HIV epidemic across the Southern US compared with prevention activities exclusively directed to NDA populations. These findings reinforce the importance of evidence-based prevention to reach EHE targets.
A 2023 study by Hamilton et al. 25 asserts that reaching the EHE goals is only possible with increased ART coverage and pre-exposure prophylaxis (PrEP) outreach in the Southern US, which has the lowest number of PrEP users per new HIV cases in the United States, the lowest rates of viral suppression among people with diagnosed HIV, and greater rates of HIV transmission. 26 –29 Given this performance on these indicators, the Southern US would not benefit from rejecting federal guidance to emphasize those at ongoing risk of HIV. It also underscores the importance of EHE, which despite having had bipartisan support when established, has never been fully funded. 30 In fact, the House of Representatives recently proposed a $800 million reduction in EHE funding for the 2024 fiscal year. 31 Consistent and adequate federal support is needed if our nation plans meet the HIV reduction targets for 2030 established by the Trump Administration.
Our HIV projections are likely underestimates as they do not consider several social and policy factors that impact HIV prevention and care in the Southern US. 32 For example, Southern US states that have not participated in Medicaid expansion have higher uninsurance rates than the national average, 33 which impacts individuals living in poverty who are often at greater risk of contracting HIV. 34,35 Further, wrap-around services, such as syringe service programs, can support HIV prevention among PWID, yet these programs remain unauthorized in four states in the Southern US and have been rolled back or limited in localities with HIV outbreaks among PWID. 32,36,37 Laws criminalizing HIV infection based upon outdated or scientifically disproven transmission scenarios heighten stigma and discrimination against people living with HIV across the Southern US and disproportionately impact communities of color. 38 Additionally, the recent wave of anti-LGBT legislation sweeping across the country further complicates HIV prevention and care for the populations most impacted across Southern US states and nationally. 39 –41
Our analysis has several limitations. First, the goal of our projections is to investigate how HIV policies prioritizing NDA populations might impact progress toward 2030 EHE targets, 2 not to provide detailed epidemiological models about HIV transmission, which are influenced by factors such as life expectancy, year of diagnoses, changes in treatment access and adherence, sexual contact, and comorbidities. Second, we assume that transmission occurs within DA and NDA populations separately; however, it is important to recognize that social networks may potentially lead to alternate transmission patterns not captured in our projections. Third, HIV cases that were disaggregated by population type included potential duplications for individuals who fit into multiple groups (e.g., cisgender women who use drugs are counted both as cisgender women and PWID when considered independently). Duplicate HIV cases were removed when calculating overall state-level incidence rates as well as pooled incidence rates. Last, we do not calculate costs associated with shifting HIV prevention efforts. Lifetime treatment cost of HIV alone could vary significantly depending on geography, demographic characteristics, adherence, diagnostic delay, comorbidities associated with long-term ART, etc. 42 –45 Future studies should consider the various financial repercussions of avoidable HIV cases on private, state, and federal institutions.
It is imperative that federal and state health officials design and implement HIV programs based on objective, scientific data about where the HIV epidemic is concentrated to ensure meaningful progress toward 2030 EHE targets.
Footnotes
Authors’ Contributions
The analysis was conceptualized by G.M., S.S., N.D.R., and L.B. Data collection was led by S.S., N.D.R., and L.B. Analysis was led by N.D.R., S.S., and L.B. All authors contributed to drafting and editing the final article.
Data Sharing
All data are publicly available and may be shared upon request to the corresponding author.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This analysis was not externally funded.