
Abstract
Latina Seasonal Farmworkers (LSFW) in South Florida are a community affected by human immunodeficiency virus (HIV) due to cultural barriers, stigma, and lack of awareness of pre-exposure prophylaxis (PrEP). Building on the PROGRESO study, this study sought to: (1) develop and pre-test scientifically supported and culturally tailored PrEP materials for PROGRESO and (2) assess the acceptability of these PrEP materials by LSFW who use alcohol and/or drugs. PrEP messages were selected based on a literature review, feedback from experts working on PrEP programs, and recommendations from a four-member scientific expert panel through a two-level Delphi method. A culturally tailored PrEP presentation was developed and presented to sixteen LSFW, who engaged in four focus groups. Materials were modified based on participants' suggestions. Thematic analysis was used to assess the acceptability and usability of these materials in the LSFW community. Participants responded positively to the PrEP messages and understood their importance for Latinx communities. Participants felt empowered and comfortable enough with the information to distribute the messages to partners, children, and friends with the aid of a physical pamphlet or flyer. A strong cultural context of familialismo and confianza was present in comments made by our participants. This study has the potential to increase LSFW's PrEP awareness and initiation. Future studies may implement a hybrid-interview approach, allowing individuals to self-select into a virtual or in-person focus group. Such flexibility may increase participation and discussion by allowing participants to attend in a format they are most comfortable with, as noted by participants in this study.
Introduction
Florida ranks among states with the highest human immunodeficiency virus (HIV) incidence in the United States, and in 2019 seven Florida cities were designated priority jurisdictions in the Ending the HIV Epidemic federal initiative. 1,2 Each year, Miami-Dade County (MDC) ranks among the leading US cities for new HIV diagnoses, with more than 800 being reported in 2021. 3,4
In the United States, Latinx-identified individuals (i.e., people who identify as Latino, Latina, Latinx, Latine, Hispanic, or have ancestry in Latin America) are disproportionately burdened by HIV, with a 2018 prevalence rate of three times higher than their White counterparts. 5 Among the adults diagnosed with HIV in 2021, Latinx accounted for ∼60% of cases in MDC. 4
This risk is even greater for Latina seasonal farmworkers (LSFW), a largely underserved and resource-limited community in South Florida. 6 Further, the rate of Latina females living with HIV in Florida is 2.5 times that of White females. 3 Several factors increase LSFW's vulnerability to HIV, including but not limited to low HIV risk perception, stigma, gender norms, cultural barriers, health care access, poverty, unemployment, education, and a lack of tailored interventions. 6,7
The literature suggests that there is a high prevalence of violence perpetrated against Latinas, which has been associated with HIV risk. 8 A mother-daughter dyadic study with LSFW living in MDC reported a prevalence of emotional abuse ranging from 13% to 20% of which one third of the mothers and half of the daughters reported the perpetrator to be their husband/partners. 9 Historically, there has been a dearth of accurate, linguistically appropriate, and culturally tailored HIV prevention resources developed for farmworkers. 10
Pre-exposure prophylaxis (PrEP) has had significant success in preventing new HIV transmissions, with efficacy as high as 99% with adherence. 11 Despite PrEP being on the market since 2012, minority populations such as Black and Latinx men and women continue to use PrEP at a lower rate than their White counterparts. 12 While the release of PrEP efficacy trial results has increased knowledge of the existence of PrEP in the general community, 13 many communities who are behaviorally vulnerable, including LSFW, are unaware of its existence and/or its efficacy. 14,15
LSFW low PrEP knowledge and awareness persists despite PrEP being available at Florida's health clinics, community organizations, pharmacies, and departments of health. Educating and creating culturally appropriate PrEP messaging is vital to increased PrEP initiation among LSFW. As such, the PROGRESO-II study sought to develop and assess the acceptability of PrEP messaging tailored for LSFW. Further, this work demonstrated the feasibility of implementing an online social network-based PrEP intervention during the SARS-CoV-2 pandemic.
The goals of this article are: (1) develop and pre-test scientifically supported and culturally tailored PrEP materials for a social network-based HIV prevention intervention and (2) assess the acceptability of these PrEP materials by LSFW. In the following section, we will present methods and results for four components: (1) a Delphi method with PrEP scientific experts for selecting messages for the new PrEP component, (2) the development of culturally tailored materials based on results from component 1, (3) the assessment of acceptability and usability of these materials in the LSFW community, and (4) the modification of messages and materials to address participant's concerns and recommendations.
One of the first social network-based HIV prevention programs for LSFW is PROGRESO, a two-group randomized clinical trial implemented in South Florida. PROGRESO tested the efficacy of a social network adaptation of an HIV prevention educational program aimed at increasing HIV knowledge and condom use. In PROGRESO, there were significant changes over time in cognitive factors (HIV knowledge, condom use self-efficacy, and adequate knowledge of condom use), behavioral factors (condom use, female condom use, and HIV testing), and communication factors (talking with friends about HIV prevention and intention to negotiate safe sex with male partners). 6,16
Additional details about PROGRESO, including the methods and results, are available elsewhere. 6,16 This article presents a follow-up study, PROGRESO-II, which integrated a PrEP component into PROGRESO's social network-based model.
Methods
This study includes four components (Fig. 1).
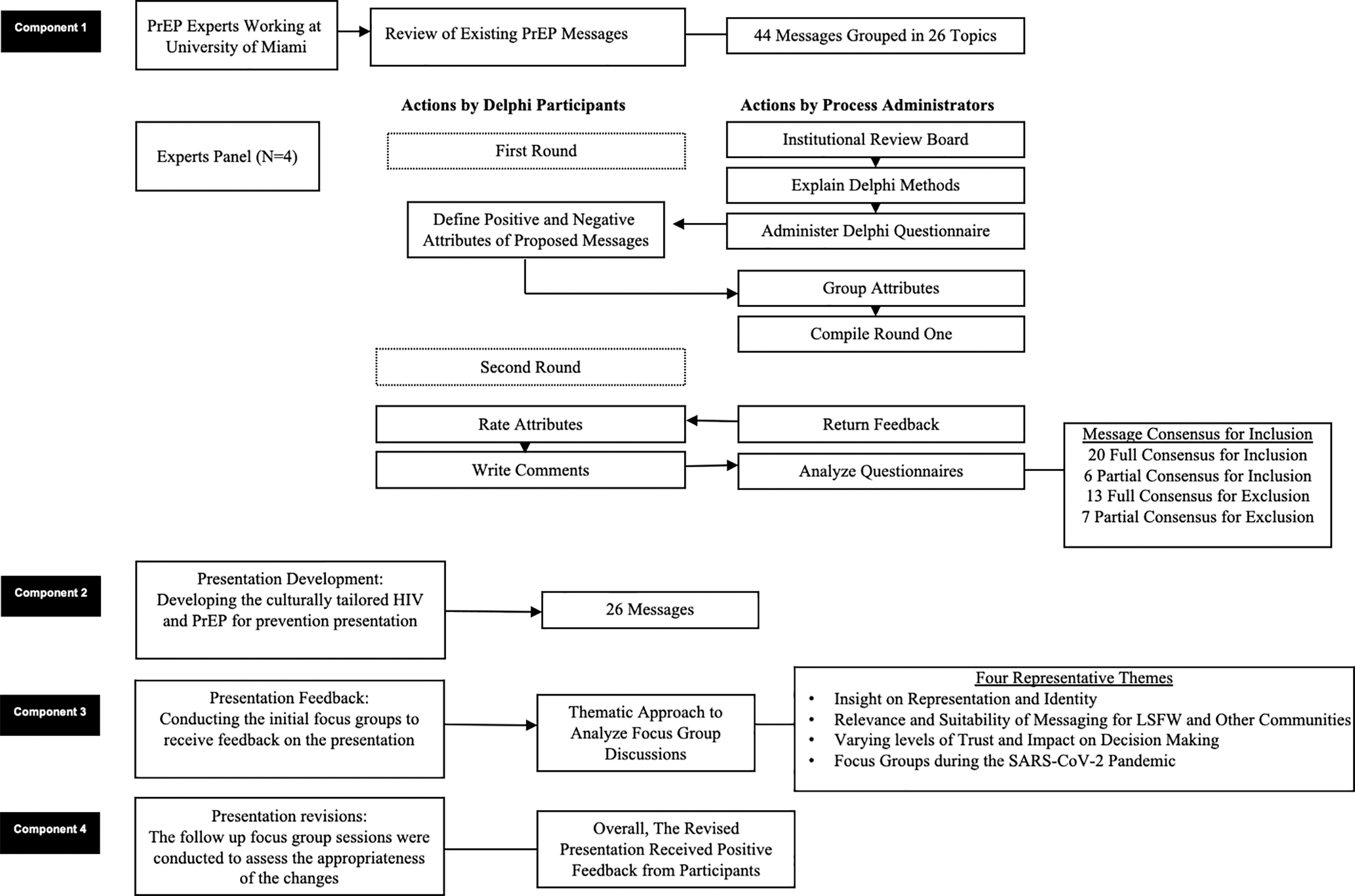
Conceptual diagram of the four components.
Component 1: implementation of a Delphi method for selecting PrEP messages
Component 1 was guided by the Delphi method, in which a panel of experts are convened to provide their feedback and insight into a selected topic, via anonymous surveys. 17,18 This iterative process begins with the expert panel providing their initial feedback to the study materials (e.g., PrEP messages); all comments (e.g., positive and negative) are shared with all other panelist. Subsequently the research team revises the materials, sending the revised materials back to the panel for additional review and feedback; this process continues until a consensus is researched by the expert committee.
Below is a detailed description of how this project employed the Delphi method. A list of 44 PrEP messages grouped in 26 topics was developed based on a literature review and the feedback from experts working on PrEP programs at the University of Miami Miller School of Medicine (Table 1). In addition, a four-member scientific expert panel provided their insight on these messages through a two-level Delphi method.
Themes Covered by the Original Pre-Exposure Prophylaxis Messages
FDA, Food and Drug Administration; HIV, human immunodeficiency virus; PrEP, pre-exposure prophylaxis; STD, sexually transmitted diseases; STI, sexually transmitted infections.
These experts were involved in the implementation of PrEP programs for minority communities in academic settings, health departments, and community organizations. Invited experts were contacted through an e-mail invitation that included the first-round questionnaire and the consent form. They were asked to complete the questionnaire and return it by e-mail.
First round of analysis
The initial questionnaire included open-ended questions regarding their initial comments on the inclusion or exclusion of each of the proposed messages. Participants were given an opportunity to suggest additional messages as comments. For each message, all expert responses were consolidated into a single list. A grouping procedure was performed to eliminate the overlaps between responses. A response that was not strictly related to the features of the message was excluded from the analysis. Next, the scientific team rejected messages that were exact duplicates.
The second round of analysis
Messages were returned to the experts for their evaluation. In addition, all panel members were able to review the feedback provided by the other members during the first round. Participants were asked to do a simple ranking to evaluate if they agreed or disagreed with the inclusion or exclusion of each message. A 7-point Likert scale was used (0 = strongly disagree, 7 = strongly agree). For example, if a message should definitely be included, researchers rated a higher score to support this statement or a lower score to refute the feature. Answers from the second round were analyzed using descriptive analysis. Based on these results, the scientific team selected the list of messages that reached full consensus for inclusion (n = 20), partial consensus for inclusion (n = 6), full consensus for exclusion (n = 13), and partial consensus for exclusion (n = 7).
Component 2: development of the culturally tailored presentation
Only the 26 messages that received panel approval during the second round of component 1 were translated into Spanish and then back translated into English to ensure the validity of the translations. To further increase the validity of the content, residents of a South Florida community where many LSFW reside along with their community leader and a Latinx scientist revised the Spanish language to ensure messages addressed diversity related to culture and literacy within the LSFW population.
The graphical content of the materials was developed by a Latinx scientist with over 20 years of experience developing social marketing materials for low-income Latinx, and who has been working with LSFW for over 10 years. The content of the presentation was developed using PowerPoint and included 74 slides (Supplementary Appendix Table S1).
The presentation incorporated Latinx cultural values of familialismo and confianza into a conversational interaction between characters representing health care providers and community members. 19 Familialismo focuses on the importance of one's family, both immediate and extended. 19 This cultural norm speaks to the collectivistic nature that often plays a role in health care decisions and practices. The topic of confianza refers to trust.
Using this approach, the characters progress through a sexual health focused conversation, discussing HIV (e.g., risk and knowledge) and ways to prevent HIV through PrEP. Through this dialogue, community member characters raised questions that were addressed by health care provider characters. This dialogue-based approach was used as a way of creating comfort around a topic that is often stigmatized in the Latinx community. Each character interacted respectfully with others, creating a forum that allowed the conversation to progress.
Component 3: assessment of the acceptability and usability of the materials
In the fall of 2020, a South-Florida female community health worker (CHW) recruited participants (n = 16) for four focus groups. Participation eligibility criteria for each individual was: be over the age of 18 years, identify as a Latina, work as a seasonal farmworker or have a family member who does, understand Spanish, and have self-reported having at least one episode of sex and one consumption of alcohol and/or other drugs within 3 months before recruitment.
The CHW was a well-respected member of this community, which facilitated recruitment and retention. The CHW utilized a convenience sampling method to recruit women from various community health organizations and community events. Focus groups were conducted in Spanish by three bilingual moderators using Zoom. 20 Zoom was selected as a safer alternative to in-person interviews as community spread of SARS-CoV-2 was present in this area, and social distancing mandates were still in place.
Each structured focus group discussion lasted between 1.5 and 2 h and involved the presentation of the PrEP messaging materials. Presenting the PrEP messages was ∼15 min of the overall focus group session. Participants were asked to join the Zoom call in a distraction-free environment, away from others, to enhance confidentiality. Following the presentation, facilitators guided a discussion about the presentation, including details regarding the message, appropriateness, relevance, strengths, improvements, and PrEP acceptability.
Questions in focus group 1 sought to understand the participant's overall perception, for example: (1) “What was the message of the presentation?,” (2) “How relevant to you are the topics discussed?” and (3) “Do the people you see in the pictures remind you of your friends, or are these people different from your friends?” The structured focus group guide is provided in Table 2.
Question Guide Utilized for Focus Group Discussions
The question guide was written in Spanish and translated for the purposes of this report.
PrEP, pre-exposure prophylaxis.
Based on the feedback provided during the initial round of focus groups, presentation revisions were made. Participants were then invited to partake in a second focus group session to review presentation revisions that were based on the feedback provided in the first focus group sessions. Interviews were audio-recorded and subsequently de-identified, transcribed by the CHW, translated and back-translated by the research team, and stored on protected servers.
In addition, a moderator wrote descriptive notes during and following the interview. Participants received $40 for each focus group session they participated in for a maximum of $80 from the two sessions. The University of Miami Miller School of Medicine Institutional Review Board reviewed and approved the study protocol (IRB No. 20180958), consent form, and all supporting materials.
Before the start of each focus group, the CHW reviewed the consent form in detail, allowed participants to ask questions, and highlighted that any information shared was confidential and participation was voluntary. To protect the participant's privacy, we only collected sociodemographic information in aggregate form, without any connection to their name or quotes.
Data analysis
We used a thematic approach to analyze focus group discussions. 21 Raw transcripts guided the development of a preliminary codebook. Through reading the transcripts, data saturation was confirmed, and a few new codes were developed after the initial two focus groups and transcripts. 22 A final version of the codebook was developed with the input of the study team after independent coding and consensus discussions. The following are some examples of included code names: cultural significance, message importance, audience appropriateness (Latinos, age, race), presentation captivation, and provider trust.
The study team was split into two pairs of raters and assigned two transcripts (two per pair) to code. After independently coding the assigned transcript, coders met to discuss codes and iteratively coded until they reached 100% consensus on the final codes. All final coded transcripts were stored, organized, and analyzed using QSR (2018) Nvivo12 Pro software. 23 Analysis of the codes resulted in four key themes emerging; these themes were inductive of the data and not identified in advance.
Component 4: presentation revision and appropriateness of changes
Following the completion of the first set of the four focus groups, the project staff revised the presentation to incorporate the feedback from session one. A key component of these revisions was addressing concerns regarding the images and phrases.
Specific revisions included new character images being selected, as some participants identified certain characters as too young, and rephrasing some materials to be more accessible to a larger audience. Appropriateness of the revisions was assessed during the second focus group session. Supplementary Appendix Table S1 includes the final Spanish messaging alongside the English translation.
Results
Components 1 and 2
Components 1 and 2 resulted in the development of the initial presentation shown to participants during their first focus group session. From component 1, the scientific team selected the list of 26 messages for inclusion of which: 20 reached full consensus and 6 reached partial consensus for inclusion. Resulting from component 2 was the initial PrEP presentation. This is the presentation shown to participants during focus group 1, with subsequent revisions made based on the participant's feedback.
Component 3
Of the 16 participants, most participants were born in Mexico (62.5%) or in the United States (31.3%). Of those born outside the United States, the range of years living in the United States was 11–50 years. Participants' mean age was 40 years (standard deviation: 9.23, minimum to maximum: 21–55). Eighty-one percent of participants were employed before the pandemic, and at the time of the study, only 37% were employed. Seventy-five percent of women reported having at least 1 or at most 4 children under 18 years old living with them, and 10 women reported having between 1 to 3 children over the age of 18 years living with them.
Seventy-five percent identified as Catholic and 25% as Christian, with most women (87.5%) reporting that religion very much influenced their lives. All participants reported being heterosexual, and the majority (81%) were either legally married or living in a common union.
Thematic analysis
Rating pairs applied ∼30 codes to the four focus group transcripts and collapsed the codes into four representative themes: Insight on Representation and Identity; Relevance and Suitability of Messaging for LSFW and Other Communities; Varying levels of Trust and Impact on Decision Making; and Focus Groups during the SARS-CoV-2 Pandemic.
Theme 1: insight on representation and identity
Participant responses to questions regarding the images of female characters used in the presentation (identified with numbers 1–10) indicated that they appreciated being able to identify with the characters in multiple ways, based on characteristics such as age and race/ethnicity (Fig. 2). Participant 12 stated: “Honestly in my opinion, each person was suitable for the slide because you chose different ages, different colors, that is, you made all the people involved.
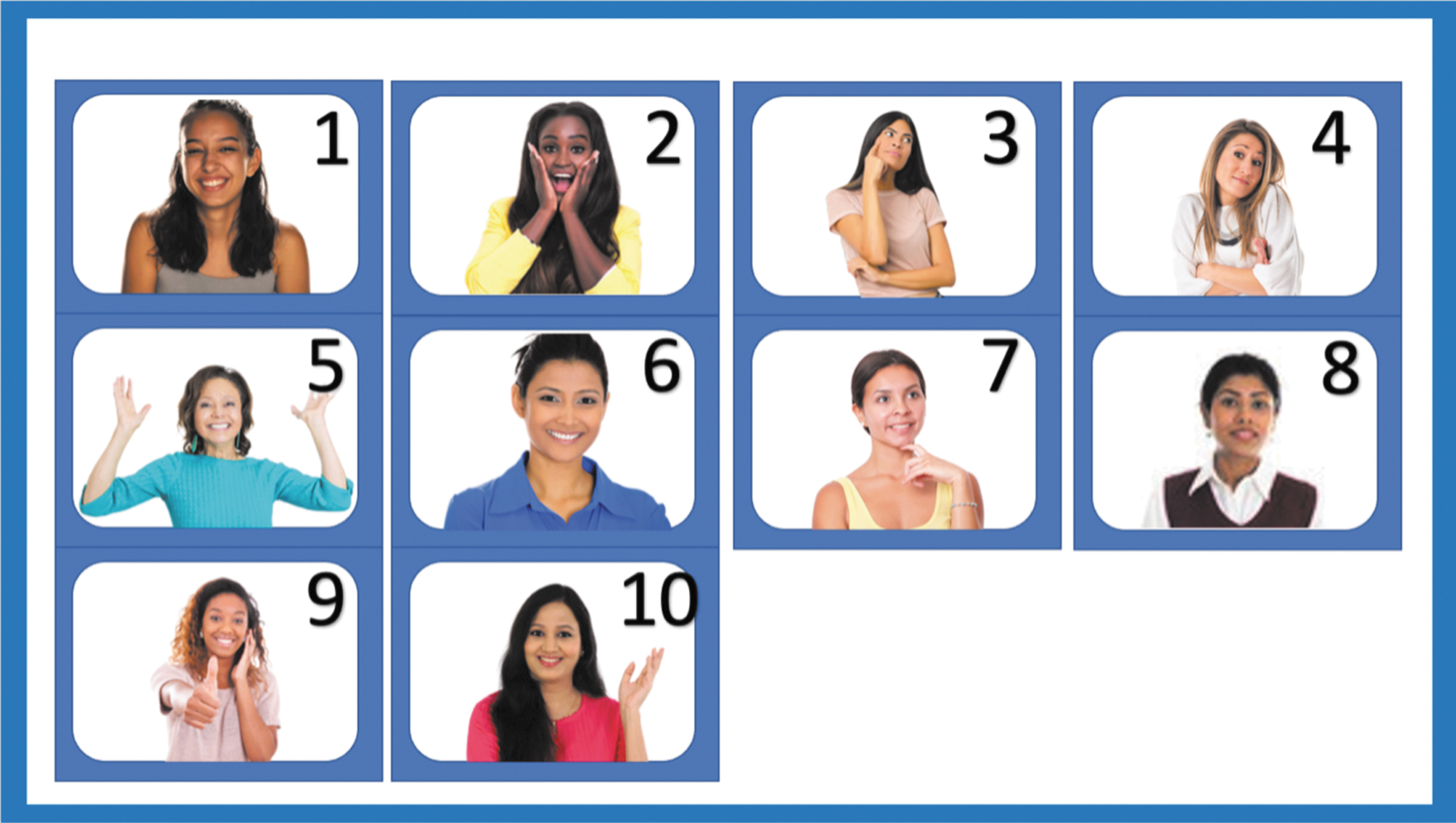
Images of female characters who were pre-tested.
So, like I said, each slide had the right person, and it showed the facial expression for each thing they said.” Participant 4 focused on age: “It will be because the others are more or less my age. I identify more with them. More or less we have some problems almost the same as I had (laughs).” Participants articulated reasons to exclude specific images or representatives for the presentation based on images depicting women of younger ages. For example, Participant 10 stated: “Well number 3 does seem a little too young to me. So it seems to me that an older person would look more trustworthy.”
Subtheme 1.1: insight on representation and identity in the presentation and in the community
Participants communicated their perceptions on who may be at highest risk of acquiring HIV as well as the importance for the presentation to be a safe talking space and representative for anyone who may be experiencing abuse. Participant 13 conveyed an understanding of sexual stigma or shame attached to HIV/AIDS when communicating with a partner and the importance of communicating prevention with a partner, “I also feel that passing on the information and that we understand that we have to protect ourselves, even if the husband says, ‘why are you taking that, no, who are you sleeping with, what can happen in these situations, why are you doing that?’ … As it is clear that AIDS can be spread in other ways, not just through sex.”
On another note, Participant 7 stated “We see Americans, well those who are on the street and stuff and I imagine that well I said maybe it is Americans who have this disease more.” Participants were also presented slides with a character in an abusive situation. In response to this, Participant 2 and 10 expressed how women who are experiencing abuse should be included in the presentation as it is important for these women to have avenues to express needs if they would feel comfortable: Participant 2 voiced, “Yes, it is good so that those who are afraid to speak or something see that, the photo and identify themselves and then maybe they talk more. Either they know that there is also help for them, or that they are not the only ones who are going through it.”
Participant 10 similarly said, “Well the message for me is that they want to make PrEP known so that women, especially women who have or are suffering abuse within their homes, can protect themselves from contracting HIV.” These concerns and issues raised by the participants can be linked to the concept of marianismo, which is a cultural norm for women to be sexually naïve. 8 Marianismo has been identified as a risk factor for intimate partner violence and for sexually transmitted conditions such as HIV. 8
Theme 2: relevance and suitability of messaging for LSFW and other communities
Participants agreed that messages were appropriate and wanted to share them with other groups, including other Latinx community members and across age groups. Participant 4 stated, “I say yes if the women is free to or wants to acquire more knowledge, she is going to accept it.”
Subtheme 2.1: audience appropriateness for LSFW
Participants described the messages in the presentation as beneficial, noting the potential for others in the community to learn from them. Participant 5 said it was “very good information because I didn't even know that the pill for HIV [prevention] existed.” Participant 5 echoed that sentiment and stated that the presentation was “good to help other people who do not know. Because there are many Latinos that do not know that this pill exists. So yes, I would feel good to help other people to [know how to] use it.”
Subtheme 2.2: audience appropriateness based on age
The information presented emphasized its benefit to multiple age groups, including children or younger people, to inform them of the use of PrEP medication. Participants 5 and 7 respectively stated that “it is very important” for “young people … it is best.” Participant 2 said, “Oh yes, I have a 19-year-old, and I would like him to receive one of those talks because there are times when he goes to be with his little girlfriend” and that watching the presentation “helped us, that is so that we can help other people, our children, family members. To inform other people.”
However, Participant 10 expressed that they would not feel comfortable or think it is inappropriate to share this information with their child. “… but in my point of view, it would be better between women because for me my children I am teaching them other things such as abstinence, so if I there, not my point of view I would not allow my children to receive this information.”
Subtheme 2.3: audience appropriateness based on race
Participants believed that it was essential to give these messages to other racial groups, including non-Hispanic Whites and Blacks. Participant 8 asked, “why not American or African women? Um, we are Latinas, but American and African women might know that about the pill too.” Also, Participant 3 stated, “My friends that are African American, because they also have a high number of HIV, so they can benefit from that too.”
When asked if they should aim to include White American or African American characters, the participants affirmed that the material should include characters from other racial/ethnic groups. Some participants questioned why Latinx were the only ones addressed in the material because they were not aware that members of the Latinx community were the most affected by HIV in their county.
Theme 3: varying levels of trust and impact on decision making
Trust was identified as an essential component of developing and implementing an intervention with LSFW. Specially, we identified how trust varies and impacts an individual's choices, we have termed this: Varying levels of Trust and Impact on Decision Making, which includes the following three subthemes.
Subtheme 3.1: trust in PrEP
Participants reported that they trust PrEP, as one respondent (Participant 7) reported: “What I liked is that it is approved by the FDA … When they tell me that it is approved by the FDA, it is more than enough.” The mention of federal agencies within the presentation seemed to provide a sense of trust in regard to the medication and overall accountability of the information.
While many women reported feeling a sense of trust with the information presented, some women described individuals who will always doubt the information provided. For example, Participant 2 stated, “Oh yeah. There are always people who think it's a lie,” and Participant 4, “There will always be negativity in everything.”
Subtheme 3.2: provider trust
Many of the participants stated that they felt a medical doctor should deliver the message. Participant 7 noted the following: “She's a doctor, right? I think that I ask my doctor about everything, I think I would feel more comfortable talking to my doctor, so,” and Participant 14: “I will always trust the doctor in what she is telling me, that she has more information than she knows, that she has more knowledge.”
While the majority of participants selected the female medical doctor as the person from whom they would most feel comfortable hearing this information, some reported that gender was not a major component of this decision. Some participants stated that if the provider was male and a medical doctor, they would still feel comfortable.
Subtheme 3.3: hesitancy versus confidence in PrEP
Hesitancy regarding PrEP as medication was seen among the women due to modality of medication and distrust among medication and side effects. This can be represented by one Participant 15: Obviously, I agree with Participant 13, I do not like to take many medications, so for me personally, I would not take it. But unfortunately, there are many women in the end who feel the same way. As my family, we depend on more, how do you say, “natural medicines.” Do you get me? We think more about that than going to the doctors and taking medicines that, in the end, can also damage your kidneys or something. That is my fear of taking a medicine that in the long run can cause me harm with something else.
Similarly, participant 14 expressed hesitancy to use oral PrEP: … But nothing. I think the message they want to get across is to know more about what the PrEP pill is. [Participant 13's name] I laughed with you because I have to be dying, I am honest, to take medicine. And I am very honest, I do not take medicine for a headache or pain at all, unless I really have 3 days with the headache and I cannot stand it. But I think the message is, nothing, to let us know more about what the PrEP pill is. I think, uh, that maybe if it were an injection, that they give it to me all at once and not have to be taking pills, maybe I will accept it there. But, I agree with [Participant 15's name] that taking pills, of course not. But hey is good information. I think that well, yes what is information that we should know and I like it. I like it.
Present throughout the focus groups was the impact SARS-CoV-2 had on the participants lives. Specifically, participants reported gaining new health-relevant knowledge because of the ongoing Centers for Disease Control and Prevention (CDC) pandemic response and from the information provided in the presentation, including becoming familiar with the organization. This newly gained knowledge was reflected in participants' response, comfort, and confidence in the PrEP information provided by the presentation and the CDC. Participant 3 reported: I think that now more with the Coronavirus, a little more was mentioned [about the CDC] and now they understand a little what that [CDC] is about, but previously I do not think that many people knew.
Theme 4: focus groups during the SARS-CoV-2 pandemic
Participants differed in their preference of group modality, with some indicating preference for a virtual modality and others for in-person groups. In response to “… imagine comparing a meeting in person and a meeting here online. How do you guys compare it?,” women expressed their comfort with both types of modalities: Participant 1: For me it is the same. Participant 2: I would like in person more. Participant 4: Me too, in person more. Participant 4: We are 2 vs. 2 (laughs) Participant 12: I would say in person because at home how they are distracted sometimes some have children, so sometimes children come to ask questions, or it can be more easily deduced than being in an office or in a class only with people who they are in class.
Stemming from the prompt about preferred modality (e.g., in person or virtual groups), Participant 3 raised concerns about virtual accessibility: “but more people do not have the virtual option. Do you understand what I am saying?.”
Other participants suggested that virtual focus groups may enhance comfort for some, including younger adults: Participant 12: I say more with children because sometimes children do not want their parents to talk to them about this topic of protecting themselves and then sometimes they prefer that other people talk to them about that topic. So I say it will be easier for the children to go to this meeting like this in Zoom. Participant 11: … for me personally, both ways are fine. If I had to choose one, then yes always in person these topics are better because sometimes people dare to speak more. Oh vice versa, because also by zooming, why are other people not seeing they can have the confidence to speak.
Component 4
All 16 participants who attended session 1 were invited back, with 9 electing to participate in the second focus group. Overall, the revised presentation received positive feedback with participants reaching a consensus that their suggestions from session one were addressed. Thematic analyses of this session were not conducted as participants were only asked to approve of the changes.
Discussion
This study, implemented during the SARS-CoV-2 pandemic, sought to (1) develop and pre-test scientifically supported and culturally tailored PrEP materials for a social network-based HIV prevention intervention and (2) assess the acceptability of these PrEP materials by LSFW. Emergent themes related to representation and identity, relevance and suitability of messaging, and trust underscore important elements to consider in developing a tailored PrEP component for a social network-based intervention for this unique population.
Most participants identified with the characters and noted this as key to engagement. Further, participants reported that having a CHW was important in garnering their willingness to participate in the project. LSFW also shared their thoughts about the appropriateness of PrEP messaging, how best to deliver the information, and with whom they would disseminate the information. Notably, most participants reported that these messages are important for Latinx and would be interested in sharing the information with their community.
Lastly, participants reported that the presentation conveyed the information in a trustworthy manner, citing doctors (as depicted in the presentation) as a trustworthy source of information. This is particularly notable as a previous study with cisgender women who have initiated oral PrEP highlights the importance of having high-quality communication between the individual and the provider. 24 Further support is provided by a previous intervention for cisgender women involving provider training, electronic health record prompt, and educational videos demonstrated to be effective to increase provision of integrated PrEP services. 25
Acceptability of PrEP message
Overall, women involved in the focus groups responded positively to the messages. This positive reception is particularly noteworthy as some participants reported being unaware of PrEP before these sessions. These findings are consistent with previous studies, indicating minority populations are more often unaware of their HIV risk and PrEP. 26 Once they are made aware of PrEP, however, they become receptive to the messaging. 27,28
In our study, some participants cited hesitancy to initiating PrEP. Our materials, including information on side effects, pros, and cons of PrEP, etc., may more easily reach a community that fears the side effects of allopathic medicines. Most of the conversations referred to administering PrEP in the form of a pill, however one participant mentioned that they would be interested in taking PrEP in the form of an injection.
This is important for a few reasons: recently, injectable PrEP was approved; considering the nature of the study population, injectable PrEP may be more appealing due to the long-lasting effects and discretion. However, we must consider the existing inequities in the dissemination of oral PrEP messaging in the southern United States, and how it may indicate further disparities with the long-lasting injectable in minority communities unless new approaches are taken.
Important in aiding the acceptability of this presentation was (1) participants identifying with characters and (2) clear message language. Participants reported feeling empowered and comfortable enough with the information to distribute the presentation with partners, children, and friends with the aid of a physical pamphlet or flyer.
This has important implications for the distribution of knowledge, as social networks among Latinas play an influential role. Our study also found a strong cultural context present in comments made by our participants, similar to findings in the literature that focus on Latinx. 29 Throughout themes, we found elements of familialismo and confianza. 19 Participants often thought about and expressed who among their family, friends, and community the information should be shared with.
The topic of confianza, which refers to trust, was also mentioned across focus group discussions. It was important to have a trustworthy community member such as the lay health advisor to relay information. This built-in trust garnered a more open mind for participants and helped them feel more comfortable discussing sexual health topics with their medical doctors. The importance of sharing this presentation with victims of human trafficking was discussed in one focus group session. Raising this topic demonstrates the utility of this work for future expansion.
Limitations and future directions
In its original conception, this project was designed for in-person focus groups. Due to the start of the SARS-CoV-2 pandemic, these focus groups had to be reformatted to be done via Zoom, an online video platform. To facilitate recruitment during the pandemic, we worked with a lay health advisor who has ties to the community.
We selected this approach because of its effectiveness to reach LSFW during a time when traditional approaches were not feasible due to social distancing mandates. This convenience sampling approach allowed us to achieve our goals but does limit the generalizability of our results. Further, there were concerns that LSFW would not have access to the necessary technology to adequately participate in these focus groups and discuss the topics at hand.
However, all participants in the four focus groups were able to watch the presentation and respond to the conversations. This project provides support for the feasibility of conducting virtual focus groups with LSFW. Of important consideration are discrepancies in the technology used by members of the focus groups, such as the difference between cell phones and computers.
Participants who use smaller screens such as a cell phone may be limited in what they are able to view. In addition, connectivity issues and audio difficulties can inhibit the cohesiveness of the session. Future studies may implement a hybrid-interview approach, allowing individuals to self-select into a virtual or in-person focus group. Such flexibility may increase participation and discussion by allowing participants to attend in a format they are most comfortable with, as noted by participants in this work.
Future works should also incorporate messaging about injectable PrEP and willingness to use PrEP for prevention. The presented project focused on developing a culturally tailored and accepted PrEP presentation but did not access the participant's willingness to use PrEP or the ability for the presentation to encourage PrEP use. At the time this study was designed and implemented, injectable PrEP was not approved by the Food and Drug Administration (FDA) and therefore was not incorporated into this project. Now that long-acting injectable PrEP has FDA approval, it should be incorporated into future revisions of this presentation.
In addition, a randomized control trial of our newly refined presentation should take place, in which both oral and injectable PrEP are discussed and willingness to use either form of PrEP is assessed. Having established the acceptability of this presentation, it is now essential that we establish effectiveness of this work presentation to improve HIV and PrEP knowledge, and its ability to move LSFW along the PrEP cascade continuum.
This project presented culturally tailored educational materials for a social network-based intervention designed to prevent HIV through PrEP. Following the presentation, participants provided their insights toward PrEP and their acceptability of implementing PrEP educational materials in the Latinx community. These findings were used to refine and to enhance the presentation message and appropriateness. The final, revised presentation will educate LSFW as we seek to increase PrEP awareness and initiation, which can lead to reduced HIV transmissions in this affected community.
Footnotes
Acknowledgments
The authors would like to thank the participants of this study. They also acknowledge Kyle J. Self for his work translating the presentation from Spanish to English.
Authors' Contributions
M.K.: conceptualization, resources, writing—review and editing, investigation, supervision, and funding acquisition; E.R.: writing—original draft and formal analysis; D.J.B.: writing—original draft and formal analysis; J.A.-F.: conceptualization, methodology, and data collection; C.H.S.: conceptualization, methodology, data collection, and writing—review and editing; and Y.R.: validation, investigation, and resources.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Parts of this project were supported by the National Institute of Health-National Institutes on Drug Abuse (No. R00DA041494), the National Institute of Minority Health and Health Disparities (The University of Miami Center for Latino Research Opportunities No. U54MD002266), and the National Institute of Mental Health (The University of Miami AIDS Research Center on Mental Health and HIV/AIDS—Center for HIV & Research in Mental Health No. P30MH133399). Additional support was provided by the National Institute of Minority Health and Health Disparities (Nos. R01MD018343 and F31MD015988), National Institute of Drug Abuse (No. R25DA050687), National Institute of Allergy and Infectious Diseases (No. T32AI114398), and National Institute of Mental Health (Nos. T32MH126772 and R01MH125727).
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplementary Material
Supplementary Appendix Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.