
Abstract
In Massachusetts (MA), partner notification is routinely offered for new HIV and infectious syphilis cases, but there are no formal partner notification services for gonorrhea and chlamydia. Electronic partner notification (ePN), which allows patients to anonymously notify their partners of sexually transmitted infection exposure, could fill this gap. We evaluated the acceptability of and ideal characteristics for a statewide ePN service in MA. We performed semistructured interviews with patients at a Boston area sexual health clinic and conducted focus groups with clinicians and Massachusetts Department of Public Health Field Epidemiologists (FEs). We developed a codebook and thematically analyzed interview and focus group data; 25% of interviews were double coded. We identified six main themes from our data: (1) partner notification is a relational process and (2) partner notification is situation dependent. There are three pairs of challenges and core values for an effective ePN system: (3) stigmatization versus inclusivity, (4) trust versus mistrust, and (5) privacy versus helpful information sharing. Therefore, (6) a statewide ePN platform must be customizable at each possible step. Although ePN was acceptable across all three groups, the likelihood of individual use was grounded in a patient's sociocultural context, interpersonal relationships, trust in the platform and health authorities, desire to avoid stigmatization, and privacy needs. These factors are best accommodated by a platform that adapts to users' preferences and needs. ePN presents an opportunity to link partners at risk for gonorrhea or chlamydia to clinical care that is complementary to the more labor-intensive FE role.
Introduction
Gonorrhea and chlamydia diagnoses have risen rapidly both nationally and within Massachusetts (MA). Nationally, gonorrhea increased by 45% between 2016 and 2020; chlamydia cases decreased by 1.2% in this timeframe, likely owing to underdiagnosis as a result of the COVID-19 pandemic. 1 In MA, between 2000 and 2020, chlamydia cases rose by 251% and gonorrhea cases by 381%. 2 Although both are curable, these sexually transmitted infections (STIs) are often asymptomatic and may go undiagnosed. Untreated infection can cause complications including chronic pelvic pain, infertility, and increased transmission of other STIs, including HIV. 3,4 Partner services are crucial for identifying asymptomatic or early-stage cases to prevent complications and onward transmission. 5
Analogous to disease intervention specialists in other states, field epidemiologists (FEs) at the Massachusetts Department of Public Health (MDPH) help people with HIV and syphilis notify their partners and link partners to care. 6,7 However, FE-led partner notification is too resource intensive for responding to uncomplicated diagnoses of gonorrhea and chlamydia. The MDPH does not typically provide partner notification services for gonorrhea and chlamydia; current recommendations are for patients to notify their partners about these STIs, with the exception of complex cases (such as antibiotic-resistant gonorrhea). 7,8
Technology-based partner notification can support FE-led partner services. A 2018 review of US-based studies investigating technology use in STI partner notification found that the number of partners screened, tested, or notified and the number of new infections detected increased with the use of technology for partner services. 9 However, these studies showed mixed results regarding its acceptability. 10 –14 One technology-based partner notification strategy is electronic partner notification (ePN), whereby partners are anonymously notified via text message or e-mail about their exposure to an STI. Although there is no uniform method of messaging through ePN, and different platforms offer patients the ability to notify partners independently or with the assistance of a clinician, most ePN messages include a link to a website with information about sexual health and local STI testing options. ePN has been successfully implemented in Europe. 15,16
ePN for gonorrhea and chlamydia could expand the reach of partner services without straining resources. Designing an effective ePN system requires understanding the facilitators and barriers to its implementation in social, clinical, and epidemiological contexts. Yet no studies have jointly investigated the attitudes of patients, clinicians, and FEs toward ePN, and few studies have assessed the acceptability of specific ePN features. We conducted a qualitative exploration of ePN design and implementation in MA among patients and clinical staff at a Boston area sexual health clinic (SHC), as well as MDPH FEs.
Methods
Study setting
Patient recruitment and the clinician focus group occurred at the Massachusetts General Hospital (MGH) SHC, a low-threshold safety net clinic with sites in Boston and Chelsea, MA. Patient interviews and the MDPH FE focus group occurred over Zoom. Patient recruitment spanned August to November 2022 and the focus groups occurred in October and November 2022.
Study participants
Study participants included patients and staff at the MGH SHC and MDPH FEs. Patient participation was initially restricted to English-speaking adults with an STI diagnosis, exposure, or treatment history in the past 5 years. In September 2022, we expanded enrollment to all adult SHC patients, regardless of their STI history, in response to mpox vaccinations comprising most clinic visits during the recruitment period.
A research assistant (S.I.) reviewed the SHC schedule before each recruitment day to identify eligible patients for the study. During appointments on recruitment days, clinicians introduced the study to eligible patients. Interested patients were contacted by the research assistant to consent and schedule interviews. Owing to clinic volume, patients receiving mpox vaccinations were provided with flyers explaining the study along with study contact information.
All SHC staff and all MDPH FEs were eligible to participate in focus groups. Focus group participants were recruited through e-mail invitations sent to SHC staff and MDPH FE leadership.
Data collection
We developed semistructured interview and focus group guides in collaboration with leadership at the MDPHs Division of STD Prevention (Tables 1 and 2). Questions were informed by features of existing ePN platforms, extant literature on partner notification, and discussions between the research team and MDPH leadership. We designed a mockup ePN platform (adapted from two active platforms) that was presented to participants. The mockup ePN platform was designed to send partners anonymous SMS notifications and included options for both clinician-directed and self-directed notification, as well as an option for patients to specify the STI to which the partner had been exposed; these decision points reflect different ePN platforms currently in use in the United States. As most ePN platforms are not integrated with social media platforms, we did not include a social media message option in our mockup.
Sample Individual Patient Interview Questions and Probes
ePN, electronic partner notification; MDPH, Massachusetts Department of Public Health; STI, sexually transmitted infection.
Sample Clinician and Field Epidemiologist Focus Group Questions and Probes
ePN, electronic partner notification; ePT, expedited partner therapy; MDPH, Massachusetts Department of Public Health; PrEP, preexposure prophylaxis; STI, sexually transmitted infection.
We also designed two example ePN notification messages, which contained different levels of information about the specific STI in question, the platform's affiliation with MDPH, and steps partners could take if they felt the message was sent as a form of harassment. Individual interview guides focused on comfort with technology and social media, barriers to STI care in MA, perceptions of and experiences with the current notification process, the acceptability and perceived utility of ePN, and preferred location for ePN use (in the clinic vs. out of clinic). The focus group guides also included questions about ePNs potential role in the current partner notification process. We collected demographic information and STI history from patients. To preserve workplace confidentiality, we did not collect demographic data from clinicians or FEs.
Patients and SHC staff received $25 gift cards for participating in the study; FEs did not receive compensation per MDPH policy. Individual interviews were conducted by one study staff member (S.I.) and lasted 30–60 min, whereas the focus groups were conducted by two study staff members (S.I. and D.L.Z.) and lasted 40 min to 2 h.
Analysis
Interviews and focus groups were audio-recorded on Zoom, then professionally transcribed. We created a single codebook for all three groups using inductive and deductive approaches. Coding was facilitated using Dedoose; two research assistants (S.I. and A.T.) double-coded 25% of patient interviews to ensure inter-rater reliability. The research assistants met regularly to compare codes, discuss discrepancies, and establish an audit trail. Coded transcripts were analyzed using a thematic analysis approach as described by Braun and Clarke. 17 After coding, we organized our findings through the lens of a social-ecological model to connect interview and focus group data to the intergroup and systemic interactions that are key to partner notification (Fig. 2). 18 C.P. led the qualitative analysis process; C.P., J.J., L.P., K.L.A., D.L.Z., A.H.K., and I.V.B. provided guidance on content. This study was deemed exempt from review, and all procedures were approved by the MGB Human Subjects Research Committee (Protocol 2022-P000847).
Results
Participant characteristics
The numbers of patients who were identified as eligible, approached, and enrolled in the study are given in Fig. 1. The sociodemographic characteristics of the patient participants (n = 20) are given in Table 3. The SHC staff focus group (n = 8) included one administrative staff member, three registered nurses, three nurse practitioners, and one data coordinator. The MDPH focus group (n = 9) included eight FEs and one FE supervisor.
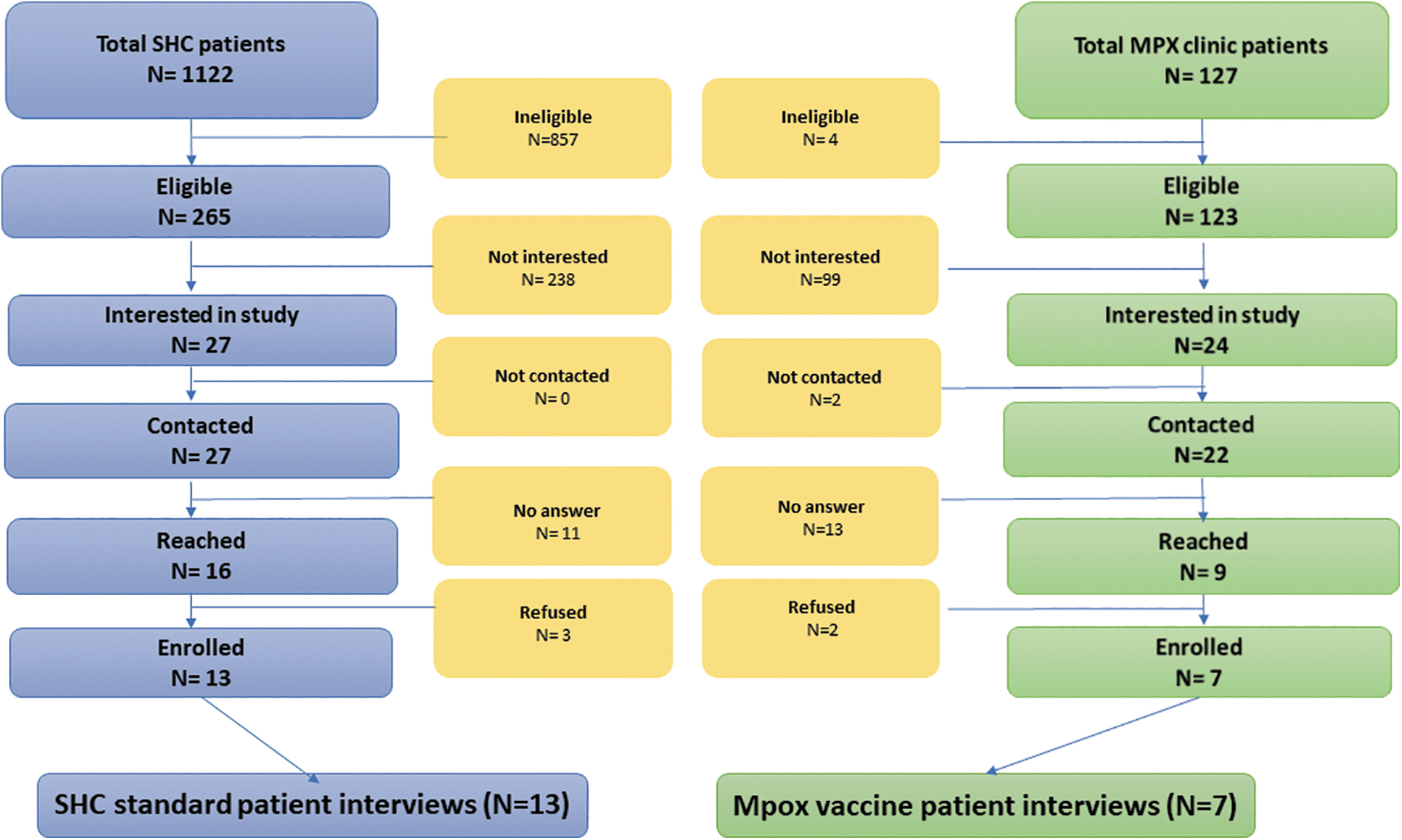
Recruitment flow diagram for individual patient interviews. This diagram details the number of patients in both recruitment groups (the SHC and the mpox vaccination clinic) at each step of the recruitment and enrollment process. Owing to high clinic volume, we were unable to collect data on patients' reasons for declining participation. Accordingly, within the SHC group, patients listed as “not interested” either explicitly declined participation or were identified as eligible for participation but then not referred to the study team by providers. SHC, sexual health clinic.
Sociodemographic Characteristics of Patient Participants
Qualitative results
We examined our dataset using parameters defined by Hennink et al. to evaluate saturation across themes, and determined that meaning saturation was met across core codes. 19 Data were organized around six themes. The first two themes contextualize the partner notification process: (1) partner notification is a relational process, and (2) user needs for a partner notification platform are situation dependent. The next three define opposing pairs of challenges and core values within an ePN system: (3) stigmatization versus inclusivity, (4) distrust versus trust, and (5) privacy versus information sharing. The sixth theme integrates the previous five to address ePN implementation: (6) To respond to the wide range of user needs and experiences, ePN platforms must allow user customization.
Relationality
The traditional partner notification process for HIV and syphilis involves multiple interactions between index patients, their partners, health care providers, and FEs. Owing to the lack of a statewide partner notification system for gonorrhea and chlamydia, partner notification is a relational process, with dynamics in the relationships between all four groups shaping engagement in and satisfaction with the notification process (Figs. 2 and 3).
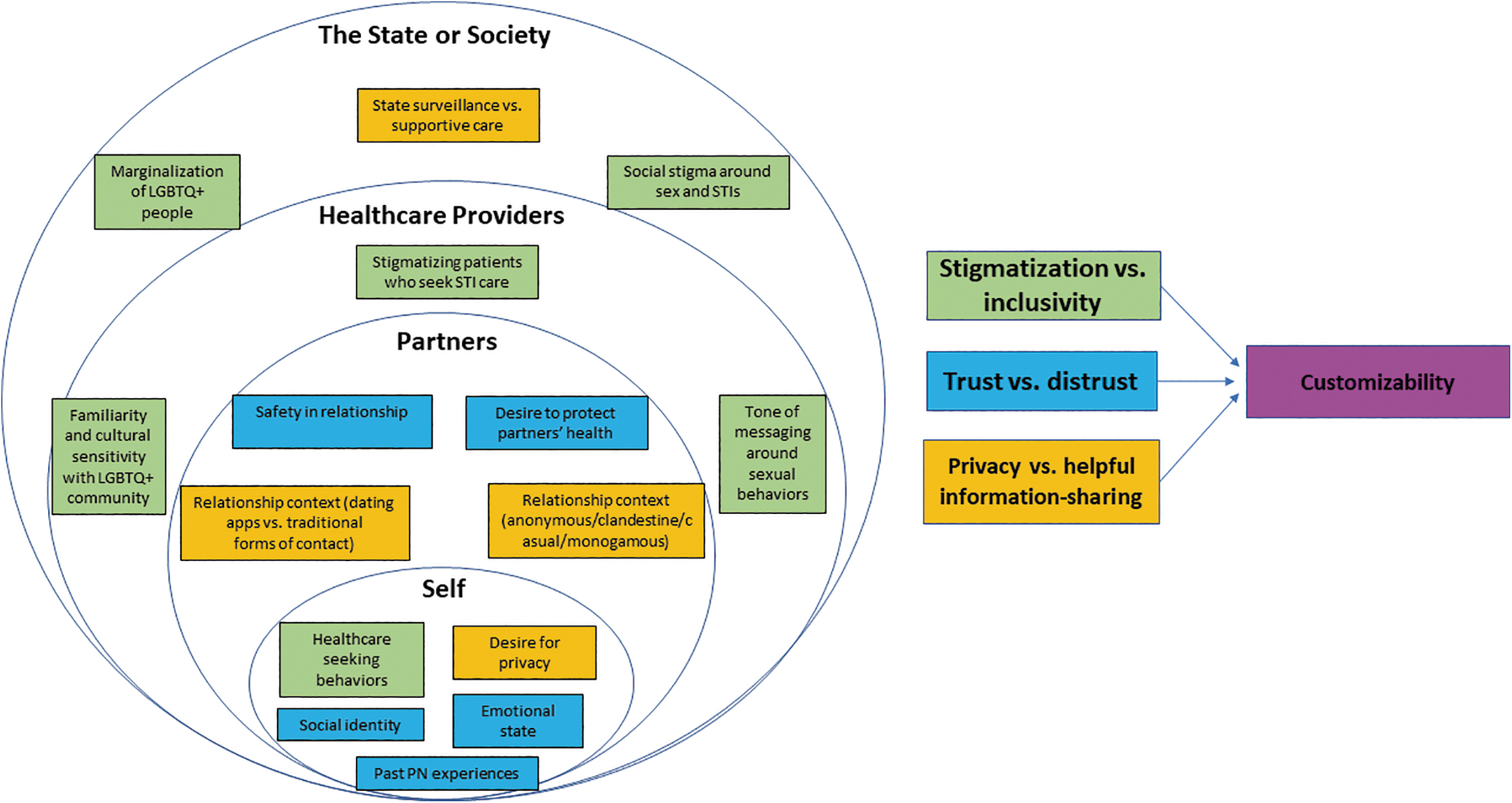
A social-ecological model of the ePN process and platform. This figure connects the interactions between parties in the ePN process with the relevant challenges and core values for an ideal ePN system (as indicated by corresponding colors). ePN, electronic partner notification.
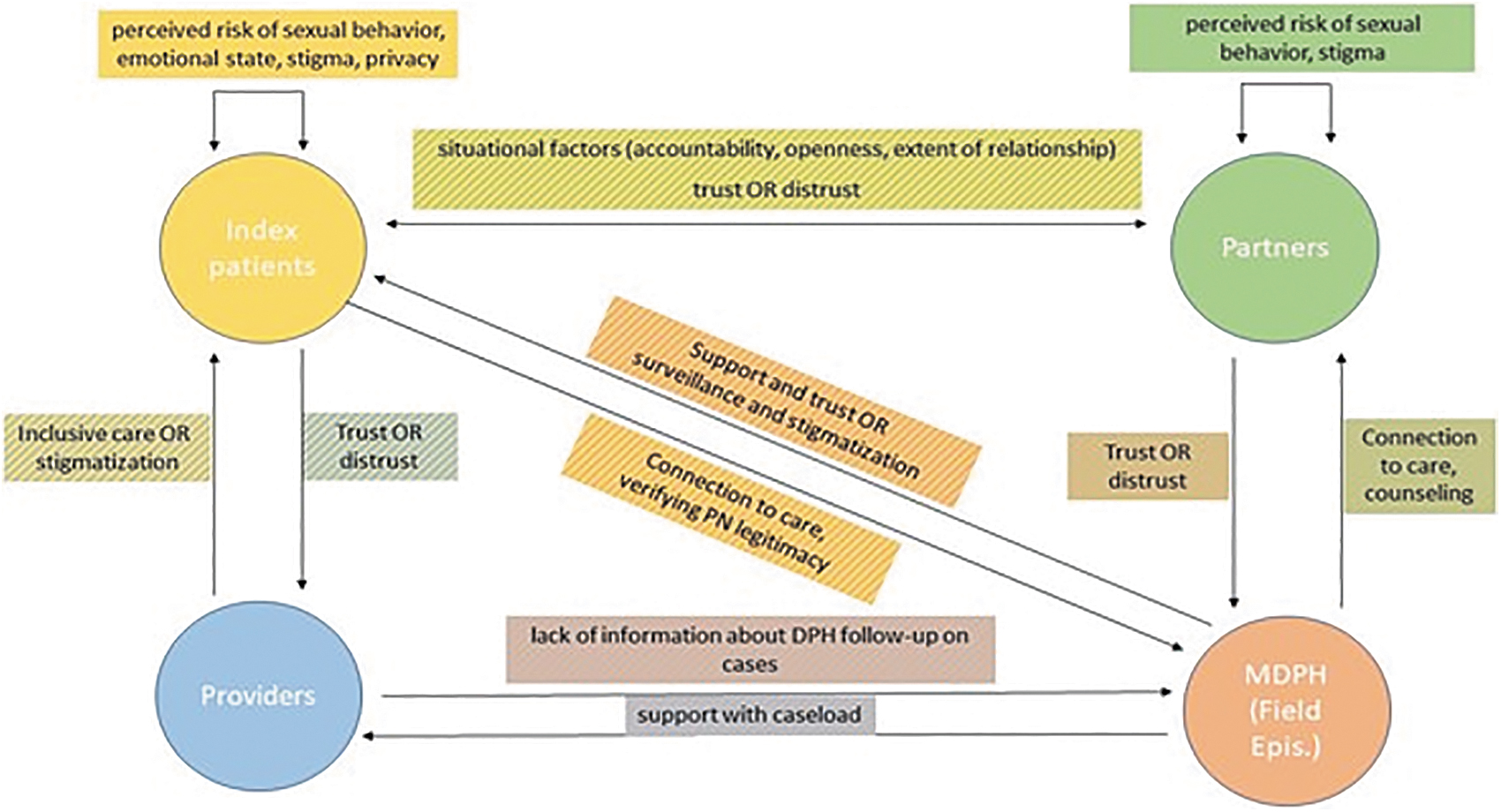
The relational dynamics between actors in the current partner notification process. This figure describes the details of the relationships between all four groups in partner notification. The arrows point toward the recipient or object of each dynamic (e.g., partners feel trust or distrust toward FEs, whereas FEs feel that they provide partners with connection to care and guidance). The colors of the text boxes correspond to the actors involved in the relational dynamic (e.g., a blue-and-yellow striped box describes a relationship between index patients and partners). FE, field epidemiologist.
Relational factors determined how patients might use ePN to notify their partners. Many patients preferred to notify monogamous or serious partners directly, “Because we have had intimacies, and I feel like that obligates one to a certain degree of continued intimacy around… STIs” (White, lesbian female, age 31). Patients who reported engaging in casual sex or not wanting to personally contact their partners cited difficult interpersonal dynamics as a reason to use ePN.
“… if … I wasn't comfortable [reaching out], then this would be the great feature to be able to still let them know that [then?] they need to go get tested without having to have that conversation.” (White, gay male, age 34)
Patients described their experiences with clinicians as driving their preferences for both receiving and sending ePN messages. Patients who received inclusive care endorsed using ePN with a clinician's support: “Maybe I have had really good doctors in the past… So having the option of telling her what to do would be great like, ‘You do it. These are the numbers. Let's get at it. Let's get it over with’” (White, gay male, age 38). However, for patients who have perceived judgment from clinicians, the opportunity to notify partners on their own using an anonymous platform was appealing. When asked whether they would prefer receiving a notification from a clinician or through ePN, some voiced a preference to be notified without clinician involvement, some voiced a preference to be notified without clinician involvement: “Not all clinicians are great. I've been lucky, and I've had a lot of great ones, but some [lean?] more to that, ‘This happened. You need to take better care of yourself. You need to—’ and so I don't want [a call?] from a clinician like that….” (White, gay male, age 34)
To be successful, an ePN platform must accommodate relational dynamics, particularly if clinicians are to facilitate platform use.
Situation dependence
Although participants emphasized the importance of making ePN available to the largest possible userbase, situational factors (including their preferred ways to connect with partners, emotional states, and geographic locations) impacted their individual preferences for ePN (Fig. 2). ePN was perceived as less relevant to those who do not collect phone numbers from their partners or who meet partners in more casual contexts: “…let's say someone meets on Grindr or
One participant described meeting partners online as a challenge for ePN implementation, saying: “…thinking about the LGBTQ community and how people meet up with one another…People who are meeting on other apps or platforms might make this a little more challenging” (White, bisexual male, age 31). Even if ePN were a practical possibility for notification, participants emphasized that their emotional state would impact whether, where, and how they would like to use ePN: “I think it would have to do with my emotional response to knowing that I have an STI at the doctor's office….” (White, gay male, age 38)
Members of all three groups noted the geographic locations of patients and partners as a key contextual factor to consider. Crucially, if an ePN message was sent from a MA phone number by an out-of-state patient or to an out-of-state partner, then the message recipient might be able to guess the sender's identity.
As one clinician stated, “you see that a lot of patients, either their permanent addresses are out of state or they have partners that are out of state or out of the country…” (SHC clinician).
Ultimately, patients' individual situations impacted the acceptability and specific use needs for an ePN system; this sentiment was echoed by clinicians and FEs in their discussions of challenges to ePN implementation.
Stigmatization versus inclusivity
Stigma around STIs was a barrier to engaging in the existing notification process and informed perceptions of ePN (Fig. 2). One patient described his past experiences with MDPH-led partner notification: “I wouldn't like the state worker calling me…. When I got syphilis and they called me, I was like, ‘Ew. Why do you know this?’ … it made me feel like an AIDS patient in the ‘80s, like you were calling me because you thought I was a danger to society.” (White, gay male, age 36)
Participants described the relationship between STI-related stigma and their interactions with ePN: “I think the fear of having to be lectured or told that you were in the wrong is deterring from wanting to talk to a provider.” (Black, straight female, age 24)
When asked to choose their ideal notification format, patients who previously expressed concerns about stigma often preferred ePN messages. These participants emphasized the need for a nonstigmatizing platform in all aspects of design. For example, several participants discussed the need for messaging from the platform to be nonjudgmental, and suggested that patients who engage in casual sex with more than one partner should only need to use the platform once while messaging multiple phone numbers, rather than defaulting to individual entries: “….if there is a choice of adding multiple phone numbers at one go, that'll be even better.” (Another race, gay male, age 39) “I really want [the platform] to…not assume things about people's orientation, gender, what they define as sex, whether or not they have multiple partners, whether or not it's one person that needs to be notified or seven….” (White, heteroflexible male, age 33)
Accordingly, an ideal ePN platform must be inclusive in both its language and functionality.
Distrust versus trust
All three groups identified distrust in the legitimacy of the platform and concerns around harassment as a potential barrier to ePN use. Several participants believed that partners would perceive ePN messages as spam and recommended methods for conveying legitimacy: “I definitely would want to somehow verify that it's real…just making sure it looks like a verified site and maybe that it has some support by professionals or kind of other expert institutions.” (Black, straight female, age 24) “Maybe having something in the text saying like, ‘If you want to learn more about this program, go to the Massachusetts state website, type in partner services, which will provide you all the information and the main number, and you can sort of corroborate through that process’.” (MDPH FE)
Clinicians and patients also spoke about the likelihood of patients using ePN to harass partners by sending inaccurate notifications. Both groups suggested emphasizing ePN's connection to the MDPH and including harassment-deterring measures: “….harassment is a big thing as well. And that was actually something that I really was concerned about, because, ‘Okay. What if somebody's going to keep blowing up my phone?’” (White, gay male, age 34) “I don't know if you're going to [include], ‘From the DPH,’ but hav[e]something like that in the beginning… and not leaving it open to interpretation about is this an old partner texting you [inappropriately].” (SHC clinician)
Although most participants stated that a clear connection to the MDPH would confer legitimacy on ePN messages, other patients expressed distrust and skepticism around MDPH involvement in partner notification, rooted in a fear of government surveillance based on a patient's personal or cultural beliefs, immigration status, or past partner notification experiences. As one patient noted, “… in my experience, most people don't want the government involved in their personal business…it's kind of scary … getting notified through them.” (White, bisexual male, age 57)
FEs noted that cultural norms and fear of government involvement can specifically impact immigrants' trust in partner notification: “Folks that are currently going through [the] immigration process have declined [partner notification services] because they believe that it's going to impact their immigration status… somebody coming from the state and asking these questions, that can feel very intrusive, especially for somebody that comes from a different culture… [where] they're not used to talking about their sexual behavior.” (MDPH FE)
For an ePN platform to gain users' trust, fears of inappropriate platform usage or surveillance must be assuaged. Suggestions included connecting ePN to clinics or the MDPH, explaining what would be done with personal information, and emphasizing confidentiality throughout the notification process.
Privacy versus information sharing
ePN's dual role in protecting patient privacy while providing partners with health information complicated the platform's acceptability, especially when patients were asked to imagine sending ePN notifications.. In the words of one participant: “…that'd probably be my biggest concern, that this really sensitive information is being communicated in a way that is being tracked …” (White, bisexual male, age 31). One patient explained how MDPH involvement in the partner notification process amplified privacy concerns: “Am I entered into a database forever now? … I know that I'm in the state system as someone who's had syphilis, and I have this feeling that anyone who works at the Department of Public Health can search me and see that I've had syphilis.” (White, gay male, age 36)
Yet when asked to imagine receiving an ePN notification, most participants preferred to receive specific information. Although some patients suggested that the platform should include an option for patients to provide partners with their name or a window of exposure dates, most patients were more interested in learning about the STI to which they were exposed. As one participant noted, “…the first [sample notification message] does list the specific STIs…That's really important as well, so [partners] know exactly what they're being contacted about.” (Black, gay male, age 29)
The conflict between privacy and information sharing was further emphasized when SHC staff and FEs discussed how ePN might impact their workflow. When recounting their experiences with patients who had received ePN messages from other platforms, a clinician explained the emotional distress caused by nonspecific notifications: “…it gets them quite upset, because they have no idea if it's something simple like chlamydia, or something more serious that's life-long.” (SHC clinician)
Unlike many patients and clinicians, FEs unanimously wanted the notification to provide as little information about the original patient as possible. Although naming the specific STI does not involve as significant of a privacy risk as including the partner's name or the date of exposure, FEs still found the inclusion of this information to run counter to the traditional notification process, thus compromising anonymity and privacy: “We text partners all the time, but we never say what the STI is… So it's a little jarring for me to see [the STI specified in notification messages]…” (MDPH FE)
Although the original patient's privacy and anonymity is essential to preserve in an ePN system, there is no consensus on how much exposure information should be shared with partners, within or across groups.
Customizability
To accommodate different needs of potential users, an ePN platform would ideally include customization throughout the notification process. For example, based on participant answers about the ways in which they meet partners, ePN could reach users in different relational contexts if offered through dating apps and social media.
When participants offered suggestions to make the ePN system more inclusive and effective, they often spoke of creating more options for notification. One participant spoke about the importance of customizing notifications for partners from international or non–English speaking backgrounds: “…maybe you can also have an option to send out a WhatsApp message. Among Europe, Asia, Africa, Latin America…. people rely on that more than iMessage… And…have a language option.” (White, straight male, age 30)
Another patient affirmed the importance of allowing patients the choice between using ePN with clinicians and sending ePN notifications independently: “I'm glad that that's something that you could do when you're in a clinical setting, although that might be kind of a difficult time for people… having a second option to go in later electronically is very good once they digest things a little bit.” (White, bisexual male, age 57)
Another desired area for customization was the level of information provided to partners (STI, the original patient's name for those who wanted a nonanonymous option, and/or window of exposure).
The principle of context-based customizability could extend beyond notification delivery to the level of care recommendations. Depending on the information patients enter into the ePN platform, notification messages could provide partners with customized resources; for example, if a patient enters an STI exposure that is an indication for preexposure prophylaxis (PrEP) for HIV, the ePN message could include links to information on PrEP. In this way, customizability could allow for more optimal notification and tailored linkage to care.
Discussion
In this study, patients, clinical staff, and FEs expressed generally positive views of ePN despite having a wide range of attitudes toward using ePN. The platform was frequently described by all three groups as a helpful tool for expanding sexual health services and empowering patients to notify partners. Although all three groups identified similar areas of focus for an ePN system (including emphasizing the platform's legitimacy and trustworthiness and ensuring patient privacy), the desired details of implementation differed within and between each group, reinforcing the importance of a flexible, customizable ePN platform for partner notification. For ePN to be optimally supportive, each patient should be able to tailor notification delivery to reflect their personal contexts.
The majority of studies on ePN systems focus on the platform's general acceptability, with several studies finding that ePN systems are acceptable to patients and have a moderately positive impact on partner notification outcomes. 10,20,21 Although there are a limited number of more targeted qualitative investigations of user preferences for ePN, our themes of relationality, customizability, and situation dependence align with the existing partner notification literature. Two US-based studies of attitudes toward partner notification systems found that participants wanted to notify their partners personally or anonymously based on the type of relationship they had. 22,23 In one study investigating the perspectives of men who have sex with men (MSM) on geosocial networking app-based partner notification, some participants wanted customizable notification messages, whereas others worried about the potential existence of inappropriately customized messages. 23
In terms of trust versus distrust and situation dependence, a study interviewing Black and Latinx MSM and transgender women who had previously completed traditional partner notification found that success resulted from state DPH workers addressing patients' distrust of state surveillance, which was often tied to the participants' experiences with marginalization. 22 These findings were echoed in another US-based partner notification study, in which patients expressed distrust and anxiety about being notified directly by the DPH. 23 A Chilean study exploring provider attitudes toward Internet-based partner notification for syphilis similarly found that providers were concerned about this approach's interactions with local sociocultural stigma around STIs. 24 Accordingly, our investigation integrates themes found within existing independent investigations of ePN in various cultural contexts to arrive at a novel conclusion.
This study has several strengths. Most qualitative studies of ePN focus on the attitudes of one participant group. To our knowledge, this article is the first to synthesize perspectives from the clinical and epidemiological partner notification processes. Therefore, we captured data about several ePN domains less explored by the current literature, including opportunities for customization.
Our analysis was limited by the low demographic diversity of our participants. Patients we recruited for interviews were predominantly White MSM. However, in addition to MSM, transgender women who have sex with men, Black and Latinx people, and people younger than 25 years old all have higher rates of STIs. 25 Our pool of 20 patients included only 3 women and did not include any transgender or nonbinary participants. In addition, given the eligibility requirements for our study, we were not able to work with adolescents; however, in 2020, over half of all reported STIs were in people aged 15–24 years old. 1 Future qualitative work on ePN should include cisgender women, transgender women who have sex with men, adolescents, and members of the Black and Hispanic/Latinx communities.
This study presents a comprehensive view of user preferences for ePN. We found that while individual ePN usage may depend on a patient's personal circumstances, the platform would be acceptable across groups if it were inclusive, trustworthy, confidential, and customizable. ePN could help expand the reach of partner services.
Footnotes
Acknowledgments
The authors thank Kathleen Roosevelt, Kathy Hsu, Liisa Randall, and Brenda Hernandez at the Massachusetts Department of Public Health (MDPH) for their support in designing this study and connecting us with the Field Epidemiologist team. The authors also thank the staff at the MGH Sexual Health Clinic for supporting study recruitment initiatives and participating in the clinician focus group, as well as the Field Epidemiologists who participated in the MDPH focus group for their contributions to our research.
Authors' Contributions
S.I.: Investigation (supporting); formal analysis (lead); writing original draft (lead). D.L.Z.: Investigation (supporting); project administration (lead); supervision (supporting); review and editing (equal). C.P.: Conceptualization (supporting); methodology (lead); formal analysis (supporting); review and editing (equal). A.T.: Formal analysis (supporting). J.J.: Conceptualization (supporting); review and editing (equal). L.P.: Conceptualization (supporting); review and editing (equal). A.H.K.: review and editing (equal). K.L.A.: Conceptualization (supporting); review and editing (lead). I.V.B.: Conceptualization (lead); supervision (lead); funding acquisition (lead); review and editing (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received funding from the National Institute of Allergy and Infectious Disease (K24 AI141036 T32 AI00743) and from the Massachusetts Department of Public Health (6 NH25PS005167, CDC sub-grantee). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the Massachusetts Department of Public Health, or Massachusetts General Hospital.