
Abstract
To test the hypothesis that implementation of a multicomponent, educational HIV pre-exposure prophylaxis (PrEP) intervention to promote universal PrEP services for cisgender women (subsequently “women”) in sexual and reproductive health centers would improve the proportion of women screened, offered, and prescribed PrEP, we implemented a multicomponent, educational intervention in a Washington D.C. Department of Health-sponsored sexual health clinic. The clinic serves a patient population with high-potential exposure to HIV. The intervention included clinic-wide PrEP trainings, an electronic health record prompt for PrEP counseling by providers, and educational videos in the waiting room. We collected preimplementation data from March 22, 2018 to July 4, 2018, including 331 clinical encounters for 329 women. Between July 5, 2018 and July 1, 2019, there were 1733 clinical encounters for 1720 HIV-negative women. We used mixed methods to systematically assess intervention implementation using the Reach Effectiveness Adoption Implementation Maintenance framework. Additionally, we assessed the interventions' acceptability and feasibility among providers through semistructured interviews. The proportion of women screened by providers for PrEP (5.6% preimplementation to a mean of 89.2% of women during the implementation period, p < 0.01), offered (6.2 to 69.8%, p < 0.01), and prescribed PrEP (2.6 to 8.1%, p < 0.01) by providers increased significantly in the implementation period. Providers and clinic staff found the intervention both highly feasible and acceptable and demonstrated increased knowledge of PrEP and HIV prevention associated with the clinic-wide trainings. Our results demonstrate the effectiveness of a low-cost educational intervention to increase provision of integrated PrEP services in an urban sexual health clinic serving women with high-potential exposure to HIV.
ClinicalTrials.gov ID NCT03705663.
Introduction
Despite the safety and efficacy of pre-exposure prophylaxis (PrEP) for HIV prevention, PrEP is underutilized by cisgender women (subsequently “women”). 1 –7 Underutilization is attributed to patient-, provider-, and health care system-level barriers. 8 –10 Patient-level barriers underlying the low utilization of PrEP among women include low awareness of PrEP, 11 –18 low perceived risk of HIV acquisition, 11 –24 lack of availability and access to PrEP, 11,15,25 concern for partners' reactions, 11,26 –29 and stigma. 11,15,26,28,30 –33 Provider- and system-level barriers intrinsic to the health care system further hinder PrEP uptake among women and include limited provider knowledge of indications for and how to prescribe PrEP, 11,30,34 –39 and racial biases in prescription practices, which disfavor Black women, who are disproportionately underserved by PrEP. 40
Despite the synergy of offering PrEP services as an extension of reproductive and sexual health care, most reproductive and sexual health centers do not routinely provide PrEP services. 34,41 –43 There remains a critical unmet need for PrEP services for women 3 and an imperative to integrate PrEP services into reproductive and sexual health care. In response, we created an educational intervention to improve provision of PrEP services in sexual and reproductive health centers, with the goal of building a reproducible, evidence-based, educational intervention to improve engagement in the PrEP cascade among women with potential exposure to HIV. The District of Columbia (DC) is a “hotspot” of the HIV epidemic in the United States; prevalence among women is eightfold higher than the national average. 44 We hypothesized that improving PrEP knowledge among providers around provision of PrEP services for women would improve the proportion of women screened for, offered, and prescribed PrEP—and ultimately engaged in the PrEP cascade.
Methods
Study setting
This implementation analysis was based in a comprehensive sexual health center run by the Washington D.C. Department of Health (IRB no. 2017-25). During the implementation period (July 5, 2018–July 1, 2019), the health center was staffed by four providers and 11 nonclinical/ancillary staff, and provided ∼2100 medical visits to women annually. Between the preimplementation period (March 22, 2018–July 4, 2018) and the implementation period, there were no changes in the clinic scope of practice, change in providers, or changes in PrEP accessibility. The majority of patients were presenting for evaluation and treatment of sexually transmitted infections (STI). Before this intervention, providers at the clinic were offering PrEP, but uptake was overwhelming among men-who-have-sex-with-men (MSM). The health center provides PrEP free of charge to un/underinsured patients. Thus, this intervention focused on provider education to overcome barriers of low provider knowledge in the published literature. 11,30,34 –38
Intervention
Before implementation at the health center, we conducted a 6-month pilot at a hospital-based family planning clinic providing services to a commensurate patient population in DC. 45 In the pilot, we developed, field-tested, and finalized the provider and staff training and the provider semistructured interview guide. The pilot findings suggested that implementation of an educational intervention to promote integrated, universal PrEP services in a sexual health clinic was highly feasible and had the potential to enhance HIV prevention efforts for women. 45 Implementation at the health center offered the opportunity to evaluate the effectiveness of the educational intervention in a larger clinical setting with more providers and a higher clinical volume.
The intervention consisted of three components, which were implemented sequentially: (1) structured provider and staff training(s) (July and November 2018 and April 2019), (2) incorporation of a prompt in the electronic health record (EHR) to encourage providers to offer counseling and education about PrEP (October 2018), and (3) looping educational videos in the waiting room to increase PrEP awareness and knowledge among patients to facilitate conversations with providers about PrEP (February 2019).
The provider and staff trainings were led by a local HIV/PrEP expert and attended by all clinic providers and staff as part of a standing, weekly clinic-wide meeting. The training focused on universal provision of PrEP education and counseling, logistics of PrEP prescription, techniques to encourage PrEP adherence and persistence, sample language, and role-plays around HIV prevention. The same expert conducted a refresher training 4 months after the initial training for all providers and staff, and again at 9 months for new providers joining the newly integrated tuberculosis clinic within the health center. We solicited feedback from both clinical and nonclinical staff, which was iteratively incorporated into the intervention. Although we chose to train both providers and staff to realize comprehensive support for PrEP services for women throughout the health center, in this article we focus on providers as the prescribers of PrEP.
At baseline, the clinic's EHR social history template (completed by providers) included screening for behavioral indications for PrEP (i.e., consistency of condom use, STI in the past 12 months, number and HIV-status of sexual partner(s), transactional sex, and injection drug use or needle sharing). Three months after the initial training, we added a universal EHR PrEP counseling prompt as a structured field for providers, inquiring if patients were interested in discussing starting PrEP as part of their current visit or at a subsequent visit.
In month 7, we introduced looping, short PrEP educational videos (
Implementation analysis
We used mixed methods to evaluate the five domains of the Reach Effectiveness Adoption Implementation Maintenance (RE-AIM) framework 47 (Table 1) to comprehensively assess our educational intervention to guide implementation of integrated PrEP services for women at the health center. The RE-AIM constructs, outcomes, measures, and data sources are summarized in Table 1. Additionally, we qualitatively assessed providers' evaluation of intervention feasibility and acceptability through semistructured interviews.
Reach Effectiveness Adoption Implementation Maintenance Constructs and Measures
EHR, electronic health record; PrEP, pre-exposure prophylaxis.
Data collection tools are detailed in Table 2. The IRB approval provided waiver of consent for collection of deidentified patient data; providers provided informed consent before completion of interviews and surveys. EHR chart review included all clinical encounters with patients who were (1) HIV negative and (2) identified as cisgender women; we excluded patients who identified as transgender women and encounters with missing data on provision of PrEP services (i.e., screening, offering, prescription).
Mixed-Method Data Collection Tools
PrEP, pre-exposure prophylaxis.
Quantitative analysis
We compared patient demographic characteristics and documented risk behaviors between preimplementation and implementation periods and performed descriptive analysis of the RE-AIM outcomes described in Table 1 using Chi-squared test, Fisher's exact test, and Student's t-test, as appropriate. We calculated group means for variables and confidence intervals for changes in provider knowledge and comfort providing PrEP services.
We performed interrupted time-series analyses with maximum likelihood estimates to evaluate the changes and trends in PrEP cascade, namely the proportions of women screened for HIV behavioral exposure(s) and offered PrEP by providers, and the proportion of women prescribed/initiating PrEP in the preimplementation period and the three subsequent stages marked by introduction of a new intervention component. A first-order autoregressive model was incorporated to account for serial autocorrelation. We set the level of significance for statistical analyses at 0.05. Although we describe changes in intercept and trends in the weekly proportions of women screened, offered, and prescribed PrEP by providers by stage, we evaluate the overall effectiveness of the intervention in its entirety; description of findings in stages is not intended to parse out the independent effects of the provider and staff training, the EHR prompt, and the waiting room video, given the continuation of the prior intervention(s) in each new stage.
Qualitative analysis
Surveys included closed- and open-ended questions. Responses to all surveys and interviews were coded using Dedoose software by two members of the research team using deductive, thematic coding and analytic practices, 48 guided by the RE-AIM framework. 47
Results
Reach
We collected preimplementation data from March 22, 2018 to July 4, 2018, including 331 clinical encounters for 329 women. Between July 5, 2018 and July 1, 2019, there were 1733 clinical encounters for 1720 HIV-negative women. Mean age was 29.3 years and the majority were Black (76%). The majority (79.5%) of women reported ≥1 CDC eligibility criterion for PrEP, in addition to living in a high HIV prevalence community and their sexual health complaint at the time of presentation (Table 3); the most prevalent risk factors were inconsistent condom use (54.1%) and multiple sexual partners (49.3%).
Demographic and Behavioral Characteristics of Cisgender Female Patients During the Implementation Period (n = 1720)
PrEP, pre-exposure prophylaxis; SD, standard deviation; STI, sexually transmitted infections.
We did not find significant differences in age or race in the preimplementation (n = 305) and implementation periods. There were significant differences in indications for PrEP; a greater proportion of women reported inconsistent condom use (73.8% vs. 54.1%, p < 0.01) and STIs (73.8% vs. 54.1%, p < 0.01), as well as a higher mean number of risk behaviors (1.5% ± 0.8 vs. 1.3% ± 0.9, p < 0.01) during the preimplementation period. Additionally, a lower proportion reported transactional sex in the preimplementation period (0.3% vs. 2.2%, p = 0.03).
Effectiveness
As shown in Table 2, to assess changes in PrEP knowledge and comfort prescribing PrEP, we implemented surveys before and after the initial training and after the 4-month refresher training; all questions used 5-point Likert scales. Providers reported a high mean baseline self-assessment of PrEP knowledge [mean 4.25, standard deviation (SD) 0.43] that remained stable after the initial training (mean 4.25, SD 0.83), but improved following the 4-month refresher training (mean 5, SD 0). Providers reported perceptions that PrEP was safe (mean 4.25, SD 0.83) before completing the trainings; views on safety improved over the course of the trainings (mean 5, SD 0). Providers reported feeling comfortable screening patients for eligibility for PrEP and counseling about PrEP use; this improved further following each training session (mean 4.75, SD 0.43–5.0, SD 0). At baseline, providers perceived women would be likely to increase sexual risk compensatory behavior after initiating PrEP; however, this perception decreased from the baseline to after the 4-month refresher-training (mean 4.0, SD 0.71–2.75, SD 1.48).
In response to open-ended question in the post-training survey, all providers reported that they found the PrEP training to be beneficial. Despite high baseline knowledge, providers recommended “updated and/or regular training should be offered twice per year,” citing the training as “a good review” and “a (helpful) refresher.” Providers additionally reported additive benefits of other two components of the intervention. Providers noted the structured EHR prompt served as a reminder to mention PrEP even during a complex patient visit: “[the EHR prompt] has provided a structured field in the patient encounter that better ensures that I mention it with all of my patients.” Similarly, providers noted that the waiting room educational videos increased awareness among women, which aided in discussions about PrEP: “I have had an increased percentage of patients asking regarding PrEP. Patients seem less unaware when I prompt the discussion.”
The proportion of women screened for HIV behavioral risk factors and PrEP eligibility increased from 5.6% preimplementation to a mean of 89.2% of women screened during the implementation period (p < 0.01). The proportion of eligible women offered PrEP also increased from 6.2% to 69.8% (p < 0.01). Lastly, the overall proportion of women prescribed/initiating PrEP increased from 2.6% during the preimplementation period to 8.1% (p < 0.01) postimplementation, and the proportion persisting increased from 1.6% to 4.8% (p < 0.01).
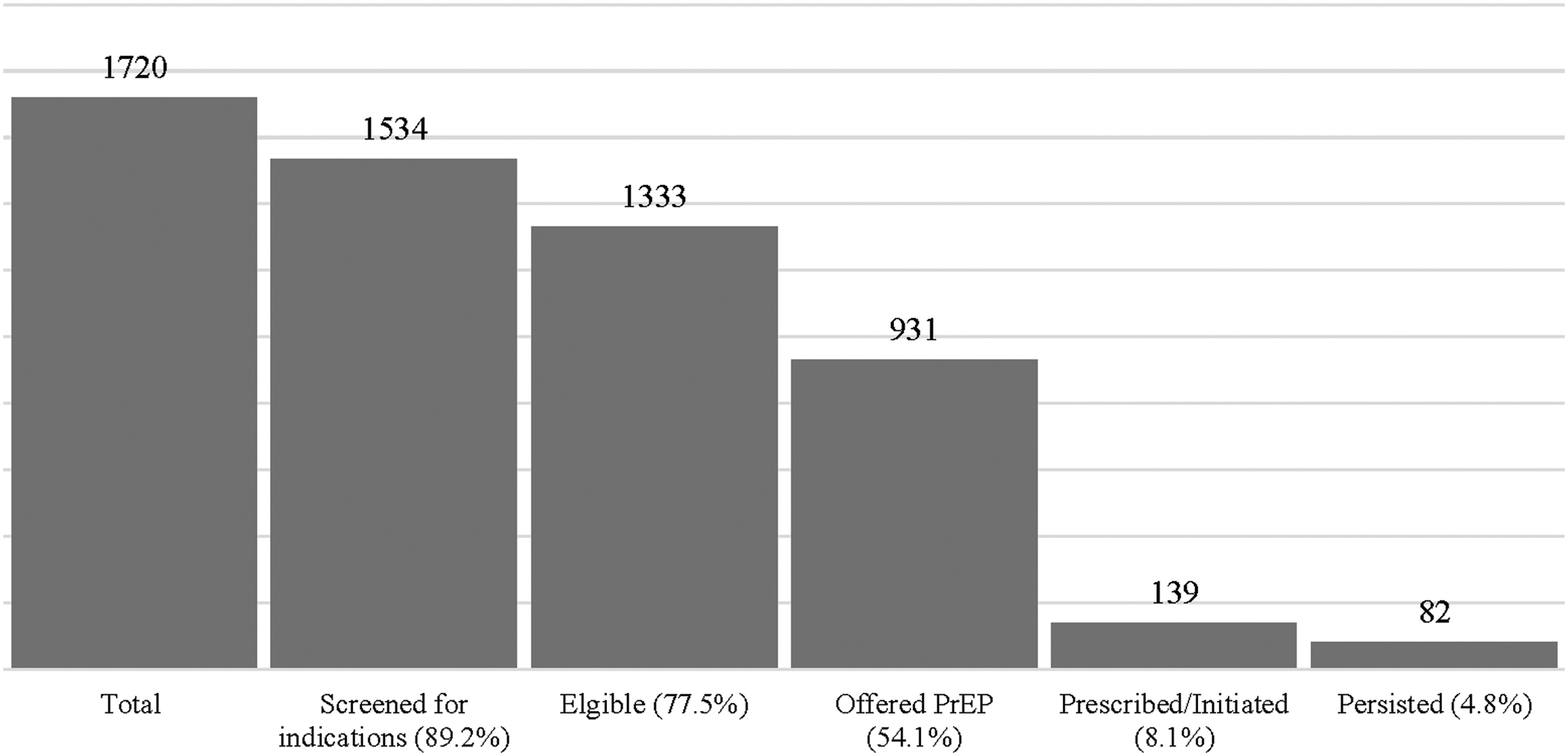
As demonstrated in Fig. 1, we observed increases in the weekly proportion of women initiating PrEP after introduction of each of the three components of the intervention: training (change in intercept 1.02, trend 0.28 NS), implementation of the EHR prompt (change in intercept 11.48, trend −0.76, p < 0.01), and introduction of the educational videos in the waiting area (change in intercept 5.12, trend 0.02 NS). Among eligible women who were offered PrEP (n = 931, 54.1%), 139 (14.9%) were prescribed PrEP/initiated; of women who prescribed PrEP/initiated, 82 (58.9%) persisted at their 3-month follow-up visit. The PrEP cascade is illustrated in supFig. 2.
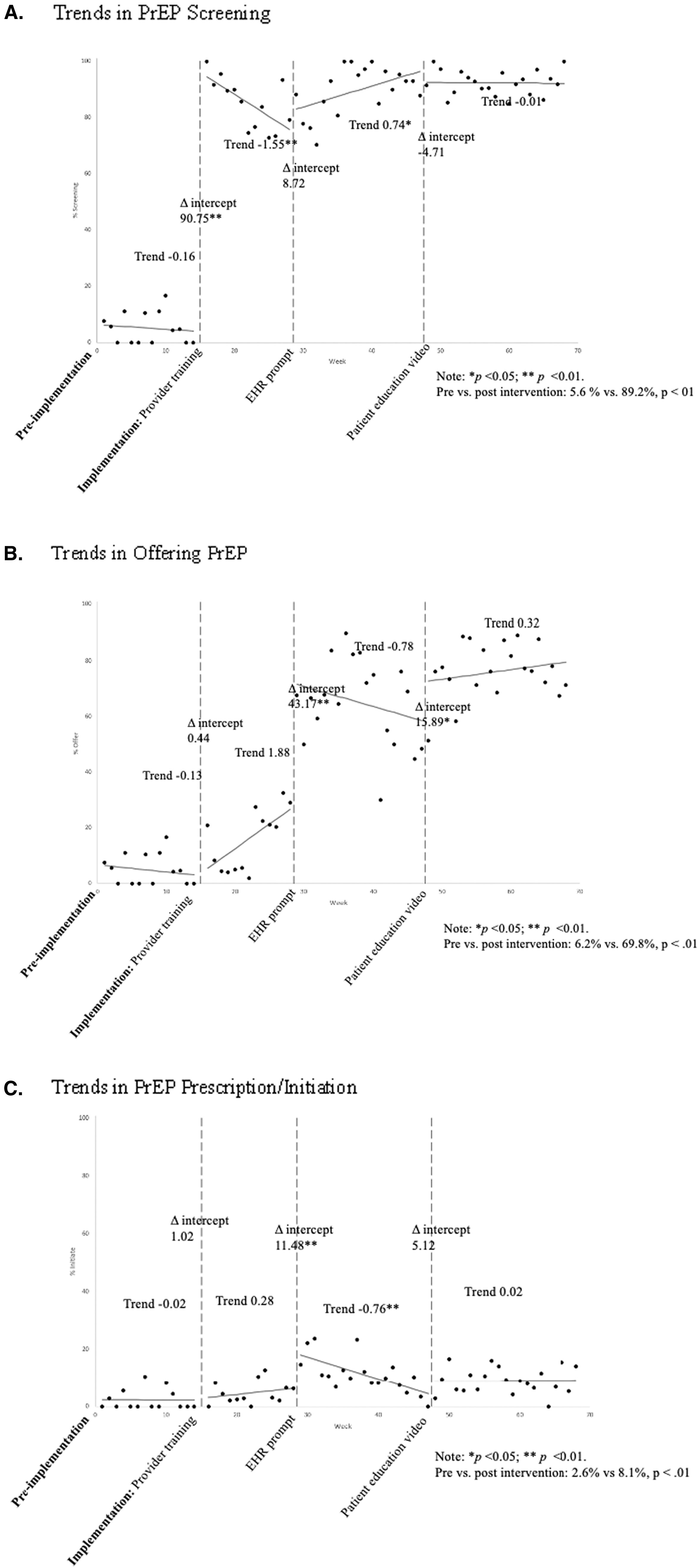
Weekly trends in
PrEP Cascade among women during the implementation period.
Adoption
All providers (one physician and three advanced-practice clinicians, n = 4) and nonproviders (n = 11) attended the initial training and all providers and seven staff attended the 4-month refresher training. In interviews 1 month into the implementation to assess the impact of the training, providers reported high feasibility and adoption of universal PrEP screening and counseling for women, noting: “It's gotten easier and more comfortable to bring up conversations around PrEP.” Providers found synergy in PrEP provision within a sexual health center and reported a seamless transition to universal PrEP screening for women. Despite this synergy and the ability to bill for PrEP services, multiple providers noted their counseling dedicated to PrEP was limited by the allotted visit time: “I talk about PrEP to all of my patients…. The only barrier (is) time considering we have appointments scheduled every 15 minutes.” Providers additionally described stereotypes and stigma surrounding PrEP as patient-level barriers to initiation.
A provider who attended both trainings noted: “[women] seem to think sexual identification plays a larger role in HIV risk and evaluating who should start PrEP than history of STIs.” A second provider voiced related concerns: “The fear of having it billed to their insurance and having other people find out they are on PrEP makes them unlikely to even want to have the discussion.”
Before implementation of the intervention, women were not routinely screened for or offered PrEP by providers (Fig. 1). We observed significant intervention effects on implementation outcomes. We observed the most substantial increase in the proportion of women screened (change in intercept 90.75) after the initial training, which waned in following weeks (trend −1.55). The declining slope in screening was reversed after introduction of the EHR prompt (trend 0.74), which was followed by relative stability (trend −0.01) in screening through the end of the implementation period.
The introduction of the EHR prompt was associated with a substantial and significant increase in the proportion of women offered PrEP (change in intercept 43.17), followed by a gradual decrease (trend −2.66). This downward trend stabilized with introduction of the waiting room educational videos (change in intercept 15.89, trend 0.32). Trends in PrEP prescription/initiation are described in Effectiveness.
Implementation
The greatest barriers to intervention implementation were logistical, as intervention costs were minimal. Coordinating trainings for providers and staff was facilitated by utilization of a mandatory standing meeting time. There were minimal adaptations to the planned intervention. Although we intended to roll out all components of the intervention simultaneously, introduction of the EHR prompt was administratively delayed until month-3. Mounting televisions in the waiting room to show the PrEP videos was delayed by 32 weeks due to construction in the health center. Still, providers and staff did not report finding components of the intervention disruptive. We added the 9-month training to accommodate the fusion of the DC Health-sponsored tuberculosis clinic with the sexual health clinic and the resulting incorporation of new providers.
Maintenance
In poststudy-period interviews (Spring 2020), providers reported continued high acceptability and satisfaction with the trainings, EHR prompt, and the PrEP awareness that the educational videos cultivated. Multiple providers commented on the increased awareness attributed to the waiting room videos: “I don't have to start from zero, partly because the videos are running in the waiting room, so they are exposed to the concept.” Providers noted that they have incorporated the training into their practice and screen for behavioral risk and offer PrEP to the vast majority of women seen at in the health center. “I bring [PrEP] up with essentially everyone. My mantra is…if you walk in our door, I'm going to at least mention it.” Despite the COVID pandemic, the health center continues universal PrEP screening and counseling of women, and continues to utilize tools of the intervention, namely the EHR prompt and PrEP training for new providers.
Discussion
This study evaluated the implementation of a multicomponent educational intervention to improve provision of integrated PrEP services for women in an urban sexual health clinic. The universal PrEP education and counseling promoted by the intervention is akin to what is now recommended by the 2021 Centers for Disease Control PrEP guidelines, but was not yet standard of care in the health center or nationally in 2018–2019. Providers found the intervention both highly feasible and acceptable and demonstrated increased knowledge of PrEP and HIV prevention associated with the clinic-wide trainings.
The majority of the women seen during the study period were reproductive-aged and Black, with ≥1 behavioral risk factor for HIV acquisition (in addition to living in a high HIV-prevalence community), consistent with the demographics of HIV incidence data in DC. Differences in indications for PrEP between the preimplementation and the implementation periods are likely attributable to the higher proportion of women screened for behavioral exposures to HIV in the implementation period (i.e., in the preimplementation period, standard of care was targeted screening of individuals perceived to be at “high-risk” for HIV acquisition versus universal screening in the implementation period, thus women screened in the preimplementation period were more likely to have more behavioral exposures due to targeted “risk-based” screening for behavioral exposure).
Higher proportions of indications in the preimplementation period, coupled with inversely lower proportions of women offered PrEP, demonstrate the unmet need for provider-level educational interventions to improve PrEP provision for women, even in a sexual health clinic already offering PrEP services and with demonstrably high levels of PrEP knowledge among providers before the intervention. The proportion of women screened by providers for PrEP, eligible women offered PrEP by providers, and prescribed/initiating PrEP, all significantly increased relative to the preimplementation period and remained stable during the latter portion of implementation period, suggesting sustainability. Although we implemented the intervention sequentially, our assessment of the impact of these activities assesses the intervention in its entirety; this intervention assumes that increasing PrEP uptake among women requires multipronged strategies to address structural-, provider-, and patient-level factors.
There is a conspicuous gap in the scientific literature on the PrEP cascade in women in the United States, largely due to the limited number of women who have initiated and persisted. The limited published scholarship centering cisgender women focuses on eligibility and intention to initiate PrEP, 8 –10,22,26,49 –51 with scant reports of the PrEP cascade among women. 45,52 –54 The result of this paucity of research and dearth of evidence-based guidance for successful PrEP services specific for women is that much of our current guidance is based on expert opinion and data from MSM. As a result, there is little evidence-informed guidance for social and structural interventions to improve PrEP uptake among women.
Medical providers play a critical role in HIV prevention and PrEP education, promotion, and provision for women. 34,55 Women identify provider support as both influential and logistically key to PrEP initiation. 12,28,34,55,56 Provider knowledge of and comfort prescribing PrEP continues to lag across specialties, 11,36 –38 as echoed in a national survey of family planning providers, 57 specifically insufficient education on HIV pharmacoprevention, lack of provider knowledge about when and how to prescribe PrEP, and ineffective communication between providers and patients related to PrEP. 30,42,51 Furthermore, racial biases may limit provider PrEP prescribing practices. 40,58
Clinical implications
This research is among the largest single-site experiences in a resource-rich setting to demonstrate the feasibility, acceptability, and preliminary effectiveness of a scalable educational intervention to implement universal PrEP services for women in a sexual health clinic. We found that our educational intervention was easily implemented and effective in increasing provider provision of PrEP services and PrEP uptake among women. Our findings are likely applicable to other reproductive and sexual health settings in resource-rich settings, particularly those with resources to provide PrEP services regardless of insurance status/coverage. Despite the synergy of offering integrated PrEP services to reproductive-age women as part of sexual and reproductive health care services, 11,34,42 most reproductive and sexual health clinics do not routinely counsel or offer PrEP. 43 Our educational intervention successfully improved provider practices around PrEP screening and provision and moved the needle on PrEP uptake among women—and speaks to the feasibility and imperative to increase HIV prevention services within sexual and reproductive health clinics.
This study, along with contemporary efforts at Planned Parenthood, demonstrate that sexual and reproductive health centers are uniquely positioned to improve PrEP utilization among women who stand to benefit from and desire to use PrEP. 59,60
Although our educational intervention successfully improved provider practices around PrEP screening and provision, prescription and uptake of PrEP remained low relative to reported indications for PrEP. We attribute this to the multitude of sociostructural barriers to PrEP initiation for women unaddressed by this intervention. In addition to lack of awareness of PrEP 8,9,28,32,33,49,50 and low perceived risk of HIV, 27,30,54 women identify PrEP-related stigma, lack of support from partners and medical providers, mistrust of the medical system, cost, and lack of access as deterrents to engagement in the PrEP cascade. 27 –34 Thus, in addition to education, we advocate for research to evaluate multipronged approaches to address sociostructural barriers.
The proportion of women persisting at 3 months (59%) are consistent with the limited literature on retention in the PrEP cascade. 52,54 Factors influencing PrEP continuation and retention in the PrEP cascade is understudied, however the existing literature has found that women largely discontinued PrEP due to low perceived risk of HIV, highlighting the importance of the concept of PrEP use during seasons of risk. 61 –63 Underestimated perceived risk and lack of understanding of optimal PrEP utilization (and discontinuation) underscore the importance of high-quality provider–patient communication regarding PrEP persistence, adherence, and ultimately safe discontinuation. 63
Strengths and limitations
This study is among the first to describe a successful intervention to improve PrEP services for and engagement in the PrEP cascade among women. Many of our lessons learned are applicable to areas where there is an unaddressed HIV epidemic among women. We recognize that generalizability is limited by inclusion of one clinical site with four clinical providers, however, it is the largest study of its kind to date with significant findings and important clinical implications. Furthermore, 100% of clinicians participated in the intervention and its evaluation. We acknowledge that acceptability bias on the part of providers may have initially influenced increased provision of PrEP services, however sustained improvement over the period of a year evidences a lasting change in practice to provide PrEP services for women. Arguably, our findings may be less generalizable to rural regions, regions with different sociodemographic composition of the patient population, or limited access to financial resources for patients to cover the costs of PrEP.
The training guide and EHR prompt are easily tailored to varied clinical settings and are highly scalable, the selected patient educational videos, however, would be best curated to reflect the sociodemographics of the local patient population.
Providers reported a high-baseline knowledge of PrEP and a self-described “PrEP-positive” clinic culture, thus the pivot from PrEP services disparately catering to MSM to universal PrEP services did not require a significant culture shift and was minimally disruptive to clinic flow. Such a culture shift may be more prolonged and more difficult to achieve at other sites. Additionally, the small provider sample size and high levels of provider comfort and knowledge preimplementation limits interpretation of the noted improvement associated with the intervention. Notably, the Department of Health funding to provide PrEP free of charge, without the need to rely upon insurance or patient assistance programs, allowed for evaluation of the PrEP cascade without these barriers. Next steps include evaluation of the intervention as part of a clinical trial in multiple geographically diverse domestic clinical settings.
EHR data are dependent upon and limited by provider documentation. Thus, the most notable increase in offering PrEP after introduction of the EHR prompt may reflect both increased documentation and increased PrEP counseling due to the introduction of the prompt.
Lastly, this study is limited by use of historical control data to demonstrate trends in provision of PrEP services to women. There were no changes in clinic scope, personnel, or PrEP accessibility between the preimplementation and implementation periods, however, we did not directly assess patient awareness of PrEP or changes in trends in awareness throughout the study period. Local public health initiatives were on-going before and during the study period and could confound our interpretation of the effectiveness of the intervention on engagement in the PrEP cascade. Similarly, it is plausible that seasonality and associated “seasons of risk” could factor into differences in uptake during the study period.
In conclusion, our educational intervention is among the first to demonstrate increased PrEP provision to women by providers and engagement and retention in the PrEP cascade among women. In the absence of comprehensive interventions to address such sociostructural barriers, PrEP utilization remains and will remain disproportionately low relative to the severity of the HIV epidemic among women, even in settings with low cost and high access.
Footnotes
Authors' Contributions
R.K.S. conceptualized the research study with M.C. and S.J.H. and acquired funding. M.D. and S.M. conducted the surveys and interviews and completed the qualitative analysis under the supervision of S.J.H. J.C.H. completed the statistical analysis. R.K.S., M.D., and S.M. wrote the original draft and R.K.S. finalized the article with input from all authors, who offered review and editing.
Author Disclosure Statement
R.K.S. is the recipient of investigator-sponsored research funding from Gilead Sciences and ViiV Healthcare managed by MedStar Health Research Institute.
Funding Information
Data reported in this publication was supported by an Investigator-Sponsored Research Award from Gilead Sciences (ISR-17-10227). S.J.H.'s time was supported by award 1K01DA050496-01A1 from NIDA.