
Abstract
In response to rising rates of bacterial sexually transmitted infections (STIs) in the United States, this evaluative study of the implementation of four evidence-based interventions was developed and implemented. In three STI and HIV high-incidence jurisdictions of the United States, nine federally funded Health Resources and Services Administration Ryan White HIV/AIDS Program clinical demonstration sites implemented (1) audio computer-assisted self-interview sexual history taking, (2) patient self-collection of urogenital and extragenital site chlamydia/gonorrhea nucleic acid amplification test specimens, (3) sexual and gender minority welcoming indicators, and (4) provider training, to make STI screening, testing, and treatment routine in their HIV primary care clinics. The priority populations of young adults, men who have sex with men, and sexual and gender minority patients were found to have risk behaviors identified in the self-interview sexual history, to prefer to self-collect urogenital and extragenital site specimens for STI testing, and to notice and like the sexual and gender minority welcoming indicators. Testing positive for a bacterial STI was significantly associated with using alcohol or recreational drugs before sex, being younger than 50 years, and having two or more sexual partners with other concurrent sexual partners. Of 255 cases of chlamydia, gonorrhea, and syphilis infections, only 13.73% of patients reported related symptoms when screened and tested.
Introduction
In the United States (US), the incidence of Chlamydia trachomatis (CT), Neisseria gonorrhoeae (GC), and syphilis has increased each year since 2014. By 2019, the incidence increased by ∼20% for CT, 50% for GC, and 70% for syphilis. 1 Between 2019 and 2021, the rates have continued to increase for GC and syphilis. 2 Disparities in the rates of these bacterial sexually transmitted infections (STIs) exist for those US subpopulations with the highest incidences. These subpopulations include adolescents and young adults, men who have sex with men (MSM), transgender individuals, Black, Latinx, American Indian/Alaskan Native, and Native Hawaiian/Pacific Islander individuals. 1,2
These same subpopulations experience disproportionally higher rates of HIV attributed to nonbehavioral reasons, including social networks and limitations to accessible health care. The continual rise in STI rates in the US is attributed to multiple factors, but as more people with HIV (PWH) are engaging in condomless sex because of being virally suppressed and unable to sexually transmit HIV, 3 and more persons at risk of HIV are engaging in condomless sex as result of using HIV pre-exposure prophylaxis, 4 –6 STIs remain a health concern within these subpopulations.
Despite these disparities, routine assessment (screening) of patients with HIV for STI risk and testing need (urogenital and/or extragenital sites) is not consistently performed in many clinics in the US. Although annual testing of CT/GC and syphilis is recommended for all adolescents and adults with HIV, the US Centers for Disease Control and Prevention (CDC) recommends that patients reporting having had two or more sexual partners, using alcohol or other drugs with sex, and those engaging in commodity sex be screened and tested every 3–6 months. 7,8 For those who test positive for CT, GC, or syphilis, CDC-recommended treatment is essential along with follow-up and retesting. 7,8 However, many STI vulnerable people are not routinely screened and tested at appropriate urogenital and/or extragenital sites for STIs in the US. 9 –11
Multiple barriers have been identified that prevent the routine screening and testing of people for STI. Health care provider discomfort with discussing sexual behaviors, limited time, limited STI testing and treatment knowledge, and patient reluctance to disclose sexual behaviors. 12 Stigma, affecting patients and health care providing teams, has been found to be a large barrier to routine STI screening, testing, and treatment. 13 Creating a welcoming clinical space regarding sexual and gender minority persons, providing patient-centered ways of reporting sexual behaviors and getting bacterial STI testing performed on a regular basis (as per CDC guidelines), and providing provider and clinical team member trainings on STIs and sexual health all seem to be needed interventions in primary care clinics to address the increasing rates of bacterial STIs in the US.
This study evaluated the implementation of four evidence-based interventions—(1) use of an audio computer-assisted self-interview (ACASI) sexual history, 14,15 (2) patient self-collection of CT/GC nucleic acid amplification test (NAAT) specimens, 16,17 (3) use of sexual and gender minority (LGBTQ+) welcoming clinical space indicators (WCSIs), 18,19 and (4) provider training—to routinize STI screening, testing, and treatment in HIV primary care settings. All interventions were selected based on a baseline needs assessment performed in year-1 (2018–2019) of this study. 20 The purpose of this study was to evaluate patient satisfaction, provider acceptability, and outcomes of integrating provider training, ACASI-based sexual history taking, CT/GC NAAT self-collection, and LGBTQ+ welcoming clinic space indicators to make STI screening, testing, and treatment a routine component of clinical care.
Methods
Study design
Nine Health Resources and Services Administration (HRSA) Ryan White HIV/AIDS Program (RWHAP) clinics in jurisdictions with higher than national average incidences of CT, GC, syphilis, and HIV (Florida, Louisiana, and Washington, DC) implemented the four evidence-based interventions. The three interventions directly encountered by patients (ACASI-based sexual history; self-collection of CT/GC NAAT specimens; LGBTQ+ WCSIs) were evaluated collectively for improvement in routine STI screening, testing, and treatment among all clinic patients as well as among subpopulations (young adults, transgender women, MSM) known to have higher incidence rates of STIs. The fourth intervention, provider training, also impacted the results since all four interventions were implemented simultaneously.
Both quantitative and qualitative data were collected sequentially to evaluate the entire study. The ACASI-based sexual health question responses and the ACASI-based Patient Satisfaction Survey responses were numerically coded for quantitative analysis. For each LGBTQ+ WCSI, the date of implementation (or if it was implemented before the study start date) was noted in a data portal by each clinic. However, for the purpose of this study, only the quantitative aggregate data were used for analysis.
All patients at each clinic were provided with the interventions, but only patients who provided consent had their de-identified data used for analysis. Participant eligibility included being 18 years or older, being a patient in the RWHAP-funded HIV primary care clinic, or for Bureau of Primary Health Care (BPHC)-funded Health Centers, a patient eligible for HIV pre-exposure prophylaxis. Consent allowed the use of de-identified data on that patient from the ACASI-based sexual history, the ACASI-based Patient Satisfaction Survey, and select data from the clinic electronic health record (EHR) from the date of consent through the end of the study (August 31, 2021).
Subpopulations
To identify if the interventions were effective in identifying those at risk and with bacterial STIs among participants from subpopulations known to have higher incidence rates of bacterial STIs, the following three subpopulations were operationally defined for analysis purposes.
Young adults were defined as any participant 18–29 years old inclusively.
MSM were defined as any male identifying person (cisgender or transgender man) who reported having oral, vaginal, or rectal sex with a person with a penis.
Transgender women were defined as participants who identified as women (either “woman” or “transgender woman”) and reported being assigned as male sex at birth.
Provider trainings
Four virtual provider trainings were conducted (one every 3 months): Epidemiology, Diagnosis, and Treatment; Culturally Responsive Care to Reduce Stigma; Taking a Comprehensive Sexual History; and Success Stories in Improving STI Care. The Culturally Responsive Care to Reduce Stigma training was provided separately to each of the three jurisdictions (jurisdictional clinical demonstration sites and convener site) within the same month, and the other three trainings were provided to all three jurisdictions simultaneously. The trainings were provided by the National Network of STD Clinical Prevention Training Centers.
Outcome measures
ACASI-based sexual history
There were 32 questions with subquestions included in the sexual history for this study (see Project Introduction), 21 which included gender identity, sexual identity, assigned sex at birth, STI-related review of symptoms, and occurrence of specific sexual behaviors and related factors since the patient's last clinic visit.
Eight survey items were used to assess the STI-related risk behaviors, based on CDC recommendations. 6,7
ACASI-based Patient Satisfaction Survey
A 6-question survey, with 10 subquestions for the question related to LGBTQ+ WCSIs, was available to participants after clinic visits to measure comfort level with use of the ACASI-based sexual history, the self-collection of specimens for throat, rectal, and genital CT/GC NAATs, and whether specific LGBTQ+ WCSIs were noticed and liked, disliked, or neither liked nor disliked. This survey was developed specifically for this study.
Electronic medical records (demographics and STI test results)
Patient demographic information, clinic visit dates, CT and GC NAAT results, syphilis serology results, and STI treatment records were extracted from each clinic's electronic medical record (EMR). For each clinic visit date during the data collection period, the patient's age (in years), health care coverage type, racial identity, and Hispanic/Latino identity were collected from the EMR. For discrepancies in data, the Rutgers team would consult with the clinic research coordinator to identify the correct data or clarify the discrepancy (e.g., the wrong participant ID number was used or the health care coverage changed).
LGBTQ+ WCSIs and cost data
A HIPAA-protected portal was developed (see Project Introduction) 21 for manual input of LGBTQ+ WCSIs (date implemented or designated as implemented before start of this study) by each clinic. The costs for providing STI-related care were estimated over a 2-week period at the initial implementation of the interventions, and again at 4–6 months after the date of intervention implementation initiation (see Project Introduction). 21 Clinical team members totaled the time they spent over a 2-week period doing STI-related direct (e.g., face-to-face encounters, telephone, text, and email contact) and nondirect (e.g., STI staff training, charting, making patient referrals or appointments, ordering/stocking supplies) patient care. The roles of the clinical team members included: prescribing provider, nurses, medical assistants, receptionist, phlebotomist, health educator, case manager, and research coordinator.
Data analysis
Descriptive statistics were used to summarize the intervention outcomes. Due to the small sample of multiple ACASI-based survey responses, only the most recent response of ACASI-based survey responses of all participants were used for analysis. Both chi-square and Fisher's exact tests were used to assess the associations between ACASI-based sexual history responses, Patient Satisfaction Survey responses, STI test results, and patient demographic information to evaluate the effectiveness of the interventions. Mann–Whitney U testing was performed for staff time effort cost differences at the start of intervention implementation and 4–6 months after the implementation start date.
Results
Participant demographics
Study participants (n = 1382) had a mean age of 44.6 years (standard deviation = 13.0) with an age range of 18–83 years. Participants primarily identified as Black or African American (n = 953, 68.9%). The sample composed chiefly of self-identified males (n = 859, 63.7%) and heterosexual participants (n = 739, 54.8%). Although 33.6% (n = 465) of male participants identified as gay/same-gender loving/bisexual/pansexual, 37.7% (n = 324) of the men reported being MSM. In addition, only 2% (n = 27) of participants identified as transgender and 14.5% (n = 201) identified as young adults. Approximately half of the participants (n = 664, 48.1%) had public health care coverage (Medicare and/or Medicaid) (Table 1).
Demographic Characteristics of Study Participants
Percentages may not add to 100 due to missing data and rounding.
ACASI, audio computer-assisted self-interview; ADAP, AIDS Drug Assistance Program, a US federally funded initiative.
ACASI-based sexual history
There were 2203 ACASI-based sexual history surveys completed by 1348 participants during the intervention period. Based on the sexual history results, a total of 531 (39.4%) participants identified STI behavioral risk at one or more ACASI-based sexual histories (participants were asked to complete at each routine clinic visit during the study period). Recommended STI testing included: 472 pharyngeal CT/GC NAATs, 505 urogenital CT/GC NAATs, 303 rectal CT/GC NAATs, and 727 syphilis tests. Based on identified behavioral risk(s) responses on the sexual history, the need for an annual CT/GC and syphilis test, post-treatment follow-up testing, or provider/participant request, a total of 2862 CT NAATs, 2816 GC NAATs, and 2146 syphilis tests were completed among the 1348 participants. One clinic mistakenly used the laboratory code for only CT testing instead of CT/GC testing for a short period until the error was identified. Therefore, more CT NAATs than GC NAATs were completed.
There were 457 STI-related symptoms reported on ACASI-based sexual histories. Of the 255 episodes of GC, CT, and/or syphilis infection identified, only 13.73% (n = 35) of the participants reported related symptoms on the ACASI-based sexual history. Having sex (including oral or vaginal or rectal), having only 1 sexual partner but that partner is new since the last clinic visit, having had ≥2 sex partners, using alcohol and drugs before sex, having a partner with a prior STI, and having a partner who is (or might be) having sex with others were each significantly related to testing positive for CT, GC, or syphilis (Table 2). The Patient Satisfaction Survey was completed 1740 times by 1094 different participants. Using the most recent completed survey responses, 93.5% (n = 1023) of the participants reported that answering questions about their sexual behaviors on a computer or tablet was “easy” or “very easy.”
Associations Between Reported Behavioral Risk Factors and a Positive Sexually Transmitted Infection Result(s)
p Values ≤ 0.05, in bold, are statistically significant.
ACASI, audio computer-assisted self-interview; STI, sexually transmitted infection.
CT, GC, and syphilis testing and results
During the study, there were 2862 CT NAATs performed and 3.04% (n = 87) were positive. There were 2816 GC NAATs performed and 3.13% (n = 88) were positive. For syphilis tests, 2146 tests were performed during the intervention period. Although 18.45% of the syphilis test results were reactive, only 6.66% (n = 143) of participants needed treatment (Table 3). We also examined the associations between STI testing and participant age and health care coverage status. Of the participants, 54.9% (n = 821) reported that they were younger than 50 years, and 39.1% (n = 541) reported that they were older than 50 years.
Sexually Transmitted Infection Testing Results
Depending on sequencing, either the RPR test was performed first, and if reactive, a treponemal antibody test (FTA-ABS) or TPPA was performed. Alternatively, the FTA-ABS or TPPA was completed, and if reactive, the RPR was completed.
Of 396 reactive cases, 80 (3.73%) were new/untreated cases.
CT, Chlamydia trachomatis; FTA-ABS, fluorescent treponemal antibody absorption; GC, Neisseria gonorrhoeae; NAAT, nucleic acid amplification test; RPR, rapid plasma regain; TPPA, Treponemal pallidum particle agglutination.
The results revealed participant age (those younger than 50 years were more likely to have a positive result) was significantly associated with a positive GC urine NAAT, GC rectal NAAT, and syphilis test result (p = 0.017, p = 0.009, and p < 0.001, respectively). However, positive STI test results were not associated with health care coverage status in this study (Table 4). Of the 3 subpopulations studied, MSM were found to have 85 cases of CT and/or GC, young adults 65 cases, and transgender women 8 cases (Table 5). For syphilis, 39% of MSM, 35.8% of young adults, and 28% of transgender women had reactive serologies.
Sexually Transmitted Infection Test with Age and Health Care Coverage Status
p Values ≤ 0.05, in bold, are statistically significant.
There were no GC-positive results for cervical and vaginal tests.
CT, Chlamydia trachomatis; GC, Neisseria gonorrhoeae.
Positive Sexually Transmitted Infections by Subpopulation
CT, Chlamydia trachomatis; GC, Neisseria gonorrhoeae; MSM, men who have sex with men; STI, sexually transmitted infection.
Self-collection of CT/GC NAAT specimens
For urogenital CT/GC NAAT specimens, 61.8% (n = 1343) reported preferring to collect urine, 18.9% (n = 411) preferred self-swabbing, and 19.3% (n = 420) preferred provider-swabbing. For rectal CT/GC NAAT specimens, 57% (n = 1234) reported preferring to self-swab and 43% (n = 935) preferred provider-collected swabs. For pharyngeal CT/GC NAAT specimens, 33.1% (n = 719) preferred self-swabbing and 66.9% (n = 1452) preferred provider-swabbing (Fig. 1).
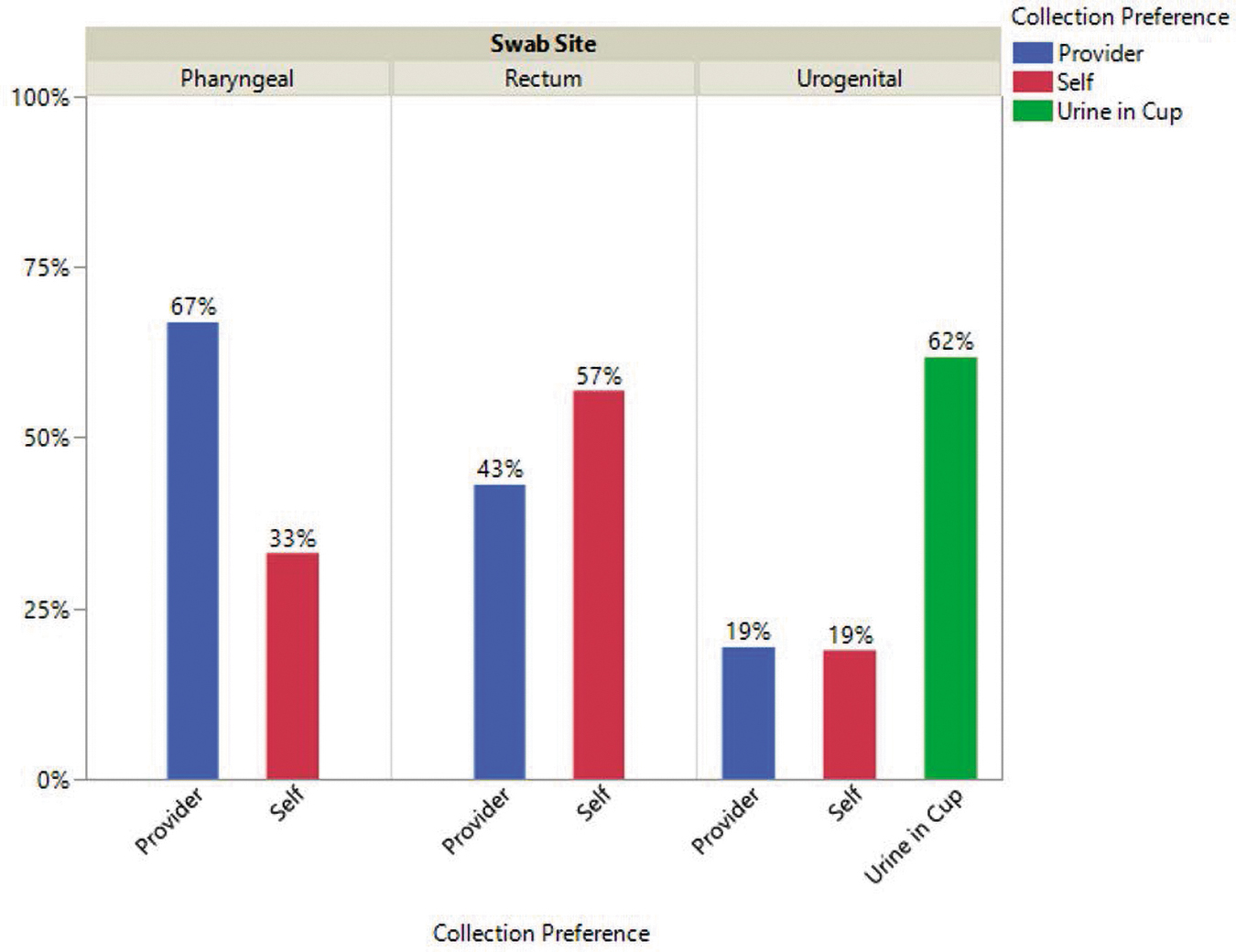
Collection preference by swab site.
The collection preference was asked with each ACASI-based sexual history in case testing was needed. Participants had the option of completing the Patient Satisfaction Survey at the end of each visit, which included questions related to comfort of self-collection of NAAT specimens. Clinical staff reported that often patients were reluctant to self-collect, but once instructed on how to self-collect, were willing to try. For those having completed self-collection of CT/GC NAAT specimen(s), comfort levels were as follow. For throat specimens, 67.7% (n = 681) of participants reported agreeing or strongly agreeing that they were comfortable collecting their own CT/GC NAAT throat swab, whereas 32.3% (n = 325) reported disagreeing or strongly disagreeing. For rectal specimens, 70.5% (n = 713) of participants reported agreeing or strongly agreeing that they were comfortable collecting their own CT/GC NAAT rectal swab, whereas 29.5% (n = 299) reported disagreeing or strongly disagreeing. For non-urine genital specimens, 65.8% (n = 559) of participants reported agreeing or strongly agreeing that they were comfortable doing their own CT/GC NAAT genital swabbing, whereas 34.2% (n = 291) reported disagreeing or strongly disagreeing (Fig. 2).
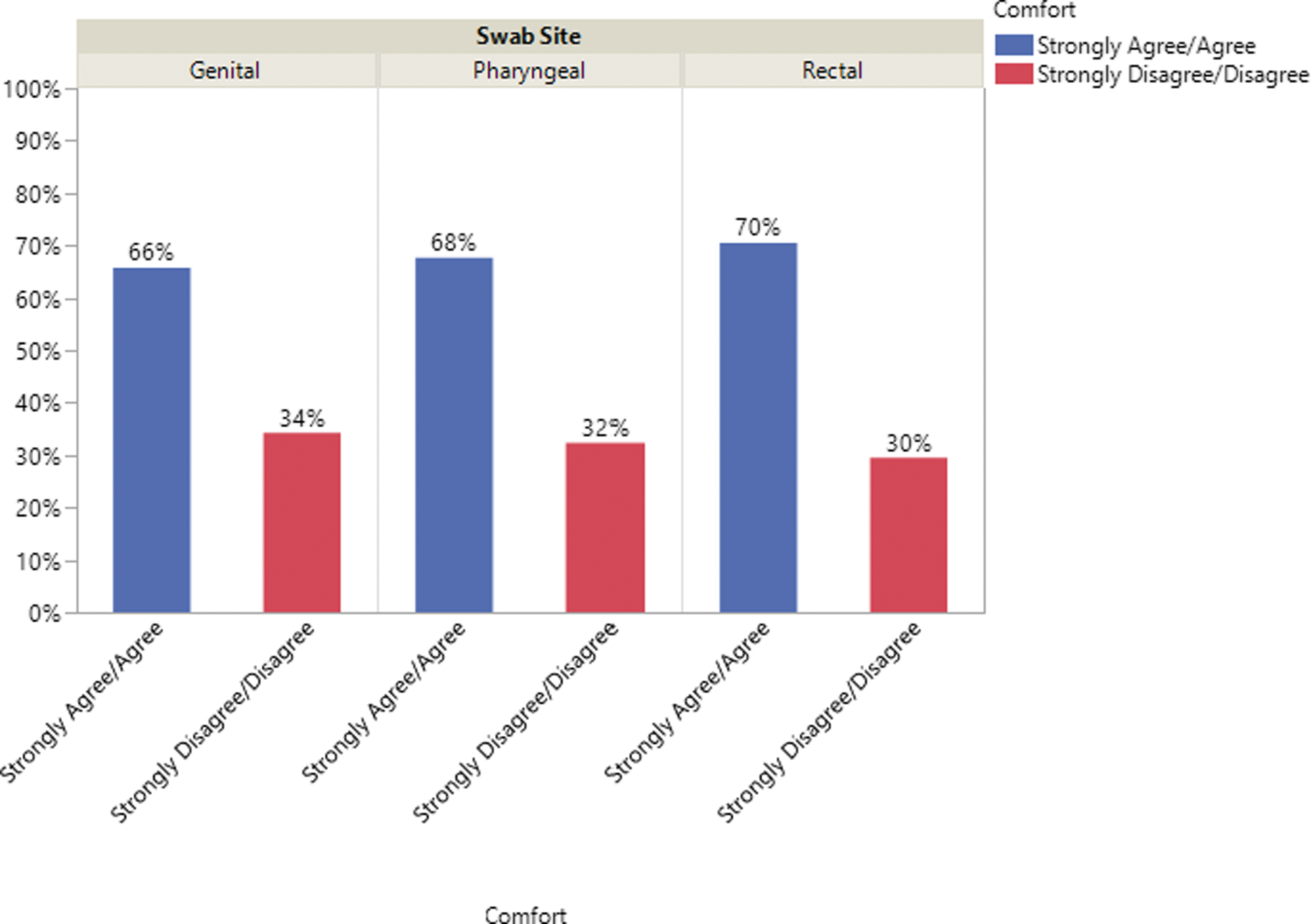
Comfort in swabbing self by site.
LGBTQ+ WCSIs
Of the 12 LGBTQ+ WCSIs, 44.4% (n = 4) clinics implemented 12 indicators, 22.2% (n = 2) implemented 11 indicators, 11.1% (n = 1) implemented 10 indicators, and 22.2% (n = 2) implemented 8 indicators. The indicators with the lowest implementation rates included: (1) having LGBTQ+ individuals on a community advisory board (3/9 clinics were unable to implement this), (2) community-based LGBTQ+ organization flyers or information available in the clinic (2/9 clinics did not have this), (3) a transgender flag in the clinic, and (4) an LGBTQ+ rainbow flag in the clinic (2/9 clinics were unable to implement as a result of organizational policy).
All nine clinics were able to implement the following five indicators: (1) gender neutral patient bathrooms, (2) visible gender and sexual minority inclusive waiting room materials, (3) history taking includes assigned sex at birth and current gender identity inclusive of nonbinary identities, (4) all staff training on gender identity diversity and sexual orientation, and (5) a gender identity, gender expression, and sexual orientation non-discrimination policy clearly displayed.
Having noticed and liked specific LGBTQ+ WCSIs was found to be associated to both sexual identity and age (Table 6). Identifying as a sexual minority participant (gay, lesbian, same-gender loving, bisexual, pansexual) was significantly (p < 0.001) associated with noticing and liking 7/12 WCSIs, and 9/12 WCSIs were significantly associated (p < 0.05) with being noticed and liked by participants younger than 50 years. The other three WCSIs (all staff training, community advisory board LGBTQ+ members, and inclusion of sexual and gender identities on sexual history) were not directly measured on the Patient Satisfaction Survey.
LGBTQ+ Welcoming Clinical Space Indicators by Sexual Identity and Age
p Values ≤ 0.05, in bold, are statistically significant.
“Other” includes something else, choose not to disclose, and multiple sexual identities over time.
Because the sample size of transgender individuals was small, we analyzed this based only on sexual identity (LGB).
LGB, lesbian, gay, bisexual/pensexual identity.
For gender minority identifying participants who completed the Patient Satisfaction Survey at least once (n = 24), 79.2% reported noticing and liking at least one of the three gender minority specific indicators. Regarding the noticing a question at intake or registration of selected patient name and pronoun, 75.0% (18/24) noticed and liked; regarding gender-neutral bathroom access, 50% reported noticing and liking; and, for the presence of a transgender flag in the clinic, 33.33% reported noticing and liking. Only 29.2% reported noticing and liking all three of the gender minority-specific indicators. For the satisfaction question, “The clinic staff and providers treated me with respect,” 23/24 (95.8%) gender minority participants responded noticing and liking of gender minority.
Costs
Nurses reported the most time spent on direct-patient STI-related care and on nondirect patient care at 0–1 month and 4–6 months after the start date of intervention implementation. The time spent by each clinic was totaled and averaged for direct patient care and for nondirect patient STI-related work (Figs. 3 and 4). Using the Mann–Whitney U testing, the direct patient care time spend was significantly (p = 0.0003) greater at 4–6 months after implementing the interventions compared with 0–1 month of implementation. The time efforts on nondirect patient care STI-related activities were not significantly (p = 0.583) different at 0–1 month and 4–6 months after the initiation date of the intervention implementations.
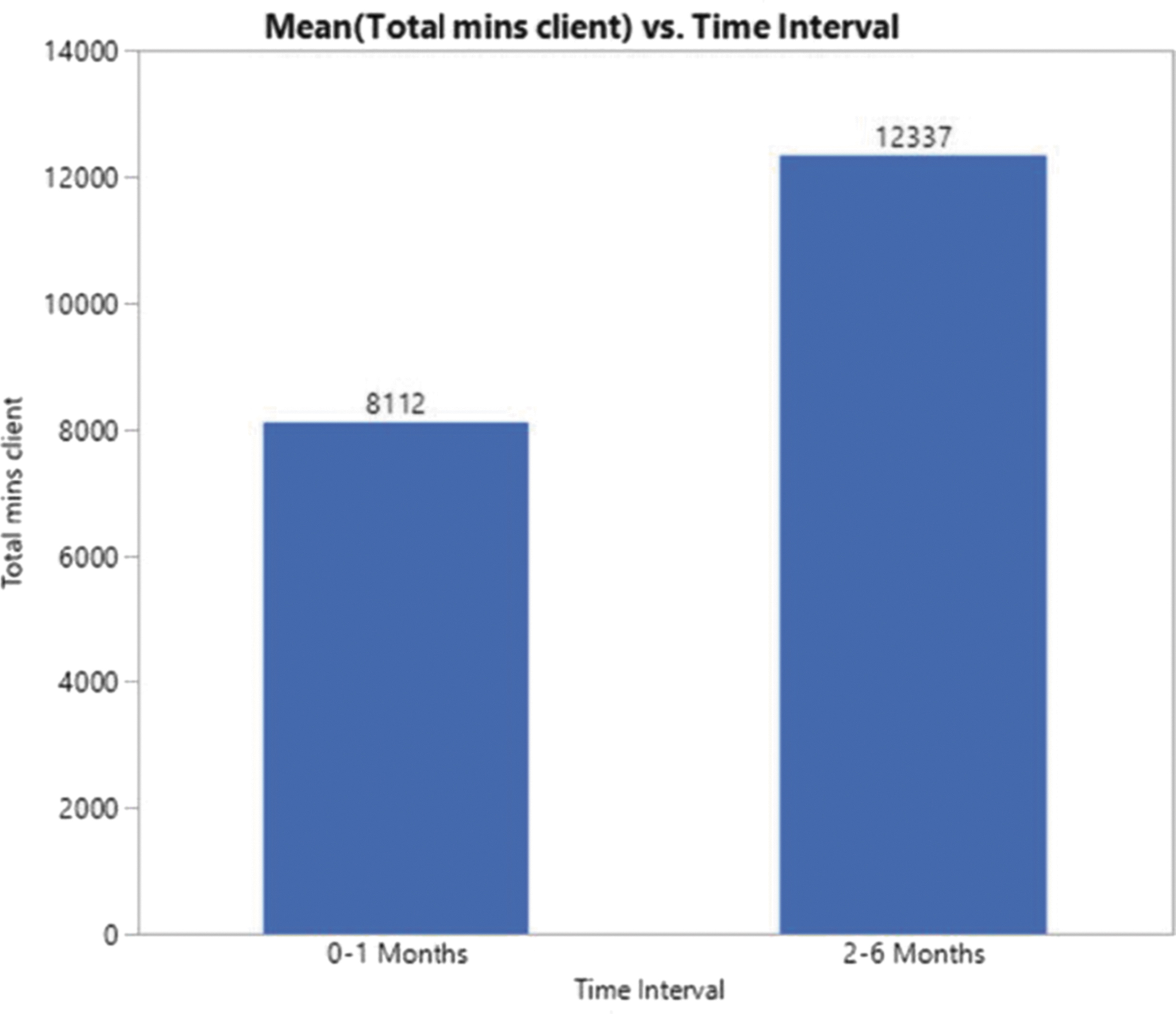
Average total direct patient contact STI-related time efforts. STI, sexually transmitted infection.
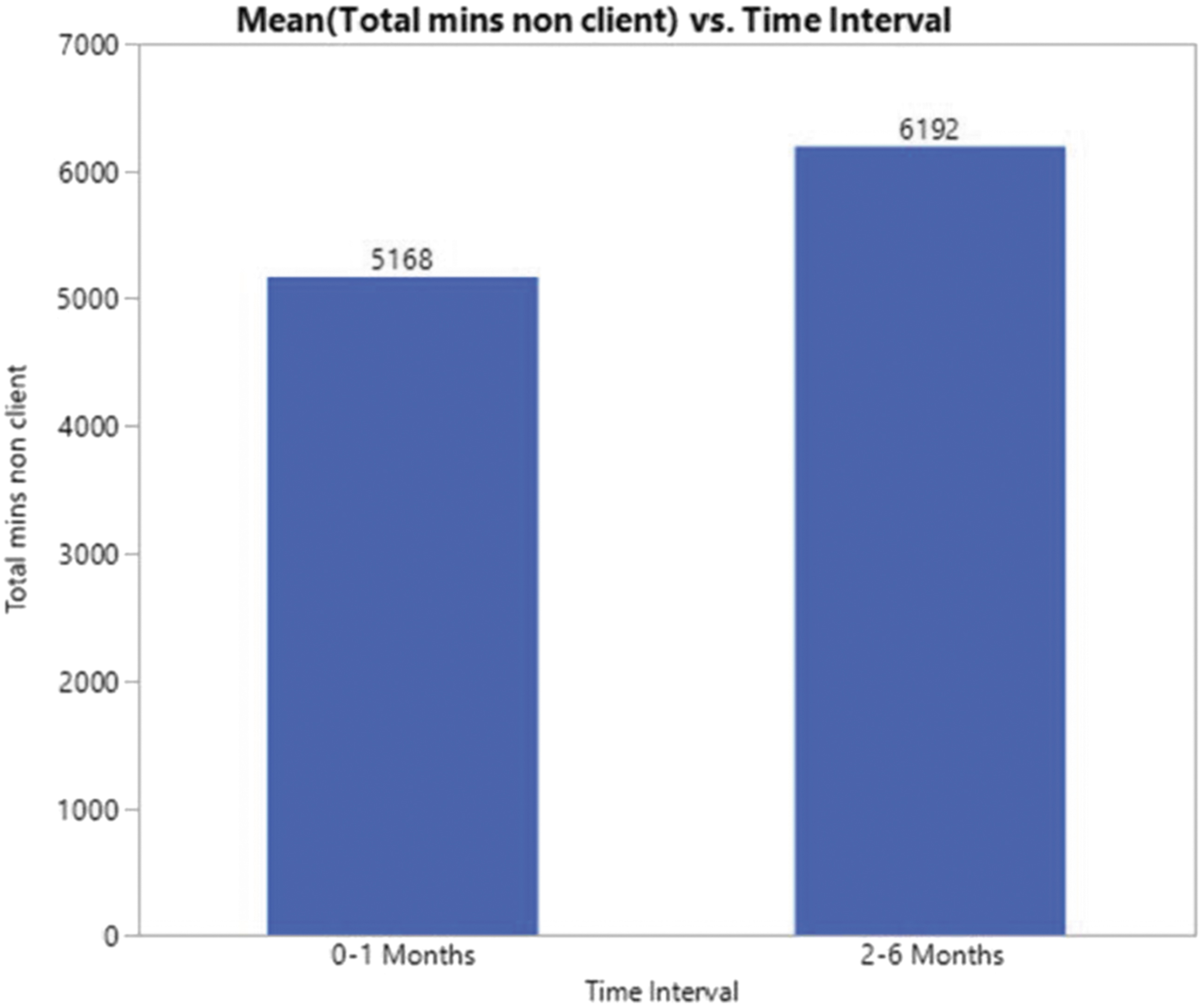
Average total nondirect patient contact STI-related time efforts. STI, sexually transmitted infection.
Discussion
In this multi-site, multi-intervention study, urogenital and extragenital site testing was carried out based on self-reported risks on an ACASI-based sexual history by STI-asymptomatic patients. The bundled interventions were acceptable and successful in the routine screening and testing of CT, GC, and syphilis among PWH in RWHAP and BPHC-funded clinics. Implementation of the interventions standardized the routinization of STI screening, testing, and treatment in each of the nine clinics in this study.
RWHAP providers at the clinics in this study reported primarily doing an annual CT/GC urine test and a syphilis test and only doing additional testing, including extragenital site testing, when the patient reported STI-related symptoms. Utilization of the self-administered electronic sexual history was reported as “easy” or “very easy” by most participants, and providers also found the ACASI-based sexual history to be an acceptable component of routine primary care. Patients reported privacy and invasiveness as reasons they preferred to self-collect rectal swabs. For pharyngeal specimen collection, most preferred to self-collect after being instructed on how to collect the specimen, yet more preferred to have a clinical team member collect the pharyngeal specimen compared with the rectal specimen.
However, of those that needed extragenital site CT/GC NAATs, self-collection over provider-collected specimens were preferred in this and other studies. 22,23 The LGBTQ+ WCSIs were significantly more likely to be noticed and liked by sexual and gender minority participants and by participants younger than 50 years. This is important since adolescents, young adults, transgender women, and sexual minority men have higher than average incidence rates of bacterial STIs. Noticing and liking the LGBTQ+ welcoming indicators served as an acknowledgment of sexual and gender minority patients and aligns with recommendations based on qualitative studies. 24 –26 Normalizing these patient-centered interventions allowed for sustainable routine screening and testing of bacterial STIs at each clinic visit.
Identification of STI predictive factors for more targeted routine STI testing has been evolving. In this study, participants reporting two or more sexual partners, alcohol or drug use before sex, and having a sexual partner who has other current sexual partners were all significantly associated with having a positive CT, GC, or syphilis test result. Being younger than 50 years was significantly associated with being diagnosed with syphilis (p < 0.001), urogenital GC (p = 0.017), and/or rectal GC (p = 0.009). In a study of bacterial STI among women with HIV in Alabama, having a positive CT, GC, or trichomoniasis test result was significantly associated with reported alcohol or drug use before sex (p = 0.025), having public health care coverage (p = 0.048), being younger than 50 years (p = 0.040), and having had a prior recent CT or GC infection (p = 0.047). 27 Other studies have similarly shown that “chemsex” (use of alcohol or illicit drugs before sex) is associated with condomless sex. 4,28
Use of LGBTQ+ WCSIs was found to be noticed and liked significantly more often by the targeted audience (LGBTQ+ participants) as well as by those younger than 50 years. For barriers and success in implementation of the LGBTQ+ WCSIs, see Impact of Implementation Welcoming Clinic Space Indicators on Sexual and Gender Minority Population. 29 Whether or not the LGBTQ+ WCSIs directly impacted the disclosure of sexual behavior information on the self-administered sexual history was not evaluated in this study but would be an important follow-up study. Risk behaviors were identified in gender and sexual minority as well as by male participants who reported having sex with men but did not identify as sexual or gender minority individuals.
Since there were no data to compare to responses to the same sexual history questions before the bundled interventions being implemented, it is unknown whether the ACASI-based sexual history or the LGBTQ+ WCSIs significantly increased the likelihood of MSM behavior disclosure, sexual minority identity disclosure, or gender identity disclosure. However, gender and sexual minority identifying persons and other non-gay, bisexual, or pansexual identifying MSM were identified as participants in this study.
An attempt was made to keep the one-time costs of the four bundled interventions to a minimum but was influenced by the size of the clinic (e.g., the number of tablets needed to provide the ACASI-based sexual history to all patients seen each day). However, the amount of clinical team member time efforts significantly increased from the initial intervention implementation period of 0–1 month to 4–6 months after initiating intervention implementation. This is most likely because of increased time spent providing the ACASI-based sexual history to each patient, education provided on urogenital and extragenital specimen self-collection, processing (collection in some cases) of STI test specimens, reviewing laboratory results, treating positive STIs, STI harm reduction education, and follow-up efforts at 2 weeks (for positive pharyngeal GC) or 3–6 months after STI risk was identified or a positive STI treatment (outside of pharyngeal GC).
Limitations
Before implementation of the interventions in each clinic, difficulties existed in identifying the numbers of patients who had been tested for each of the bacterial STI tests used as outcome measures for this project (i.e., the number of tests ordered and completed for rectal, urine, vaginal, cervical, pharyngeal CT/GC NAATs, and syphilis serologies). Among the nine clinics, there were five different EHR systems that varied even among with the same system. Therefore, baseline numbers and results of tests performed in the year preceding the implementation of the interventions were not accomplished. Additionally, pulling result reports from each of the EHRs was difficult and required the consultation with experts from each EHR in most cases. Data in several instances had to be collected manually from the EMRs of consenting participants. With manual extrapolation of data, the risk of error increases.
In March 2020, a national emergency was declared in the US, and a national “shut down” was put into place. Because of exposure to and illness from SARS-CoV-2, clinics needed to be closed for up to 2 weeks at a time. At the department of health clinics and health centers, staff were reassigned to provide patient triage of all patients coming into the clinic, and to assist with SARS-CoV-2 testing and vaccination. The intent was to have all nine clinics implement the interventions simultaneously, and begin enrolling participants on the same day, and continue collecting data for 12 months. However, because of COVID-19, some patients were fearful of coming to clinic, and infectious disease physicians involved with medical center clinics were being pulled for inpatient care and consultations related to SARS-CoV-2.
The clinics and health centers were utilizing telehealth to provide primary care services, and patients were seen in-person primarily for laboratory visits if the clinic had a laboratory in the clinic (8/9). It was at these laboratory visits patients were asked to complete the ACASI-based sexual history, and if STI testing was indicated, a standing order was used to order tests not already ordered by the provider. In addition to the COVID-19 pandemic limitations to patient volume in the clinics, natural disasters (i.e., hurricanes, floods, ice storms) occurred in the summer, fall, and winter of 2020–2021, which further affected the clinic operations in LA and DC. As a result, follow-up patient care was disrupted during the data collection period possibly resulting in fewer screening and testing visits.
For patients who could not make it in-person to the clinic for specimen collection or the on-site clinic laboratory was not available (i.e., closed because clinic was closed or laboratory personnel were being quarantined for exposure to or were ill from SARS-CoV-2), they were sent to commercial community-based laboratory collection sites. At these commercial laboratory sites (in all three jurisdictions), extragenital site CT/GC NAAT specimen collection was not allowed. Patient self-collection of CT/GC NAAT has not been approved by the FDA for extragenital site specimens, and therefore, only laboratories that have conducted a validation study of patient- versus provider-collected extragenital site specimens to verify non-inferiority of patient-collected specimens are able to test patient-collected specimens.
This was identified as a large barrier to normalizing routine screening and testing during the COVID-19 pandemic since much of primary care was performed utilizing telehealth technologies. If a patient was not able to come to the clinic for completion of the ACASI-based sexual history (it could not be performed electronically outside of the clinic) and/or had specimens collected at a commercial community-based laboratory, extragenital site NAAT specimens were not able to be done. Another barrier was limited availability of CT/GC NAAT testing kits at each clinic since the same reagents and swabs are used for SARS-CoV-2 testing, resulting in a diminished supply of CT/GC NAAT kits nationally.
In conclusion, the interventions effectively routinized STI screening questions asked of each patient, which resulted in increased testing of bacterial STIs based on reported behavioral risk. The patient-centered approach to self-completion of the sexual history along with encouragement and instruction to self-collect CT/GC NAAT specimens at urogenital and extragenital sites was satisfactory to the participants and acceptable to the clinical teams. The LGBTQ+ WCSIs and the provider trainings enhanced the ACASI-based sexual history and NAAT specimen(s) self-collection interventions to provide emotionally safer, judgment-free clinics for those at risk of STIs to get the care needed.
Ethical Approval
The study protocol was approved by the institutional review boards of Rutgers University, the Florida State Department of Health, the University of Florida, Louisiana State University, and Howard University.
Consent
Informed consent was obtained from all participants.
Footnotes
Acknowledgments
We thank the Rutgers University School of Nursing team members involved with this study in collaboration with the authors: Kathleen Cullinen, PhD, RD; Macsu Hill, PhD, MPH; Taylor Anderson, MS; Andrea Norberg, DNP, RN; Mary Jo Hoyt, MSN; Peter Oates, MSN, APRN. We also thank the clinical team members and administrators at the nine clinical demonstration sites, the three convener site teams, our training partners at the National Network of STD Clinical Prevention Training Centers, and our colleagues from the HRSA HIV/AIDS Bureau Division of Policy and Data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the US Department of Health and Human Services (HHS) Health Resources and Services Administration's (HRSA) HIV/AIDS Bureau (HAB) and Bureau of Primary Health Care (BPHC) under grant number U90HA32147. The contents are those of the author(s) and do not necessarily represent the official views of, or an endorsement, by HHS, HRSA, HAB, BPHC, or the US Government.