
Abstract
Although HIV self-testing (HIVST) has expanded in many regions, a few HIVST services have been tailored for and organized by youth. Innovative HIVST models are needed to differentiate testing services and generate local demand for HIVST among youth. The current pilot study aimed at examining the feasibility and efficacy of crowdsourced youth-led strategies to enhance HIVST as well as sexually transmitted infection (STI) testing. Teams of youth iteratively developed HIVST interventions using crowdsourcing approaches and apprenticeship training. Five interventions were selected and then evaluated among youth (ages 14–24) from September 2019 to March 2020. Given the similar outcomes and approaches, we present cumulative data from the completed interventions. We assessed HIVST uptake (self-report), STI uptake (facility reports for gonorrhea, syphilis, hepatitis B, and chlamydia testing), and quality of youth participation. Mixed-effect logistic regression models estimated intervention effects at baseline and 6 months. Of the 388 youths enrolled, 25.3% were aged 14–19, 58.0% were male, and 54.1% had completed secondary education. We observed a significant increase in HIVST from 3 months compared with 6 months (20% vs. 90%;
Introduction
Youth (aged 14–24) are often excluded from meaningful involvement in developing, implementing, and evaluating research and programs that impact their health and well-being. 1 There remains an urgent need to engage youth across the HIV prevention and treatment continuum, particularly in sub-Saharan Africa (SSA) where there is an increasing youth population and sub-optimal health service utilization. 2 SSA also accounts for 72% of new HIV infections among adolescents and young people, and the death rates attributable to HIV among this age group are on the rise. 3,4
More alarming is the current low rates of HIV diagnosis among youth in this region, as many of the undiagnosed youth do not use essential HIV prevention services, including HIV testing services and other sexually transmitted infection (STI) testing. 5 In Nigeria, for example, youth have low testing uptake such that only 16% of young women and 9% of young men had ever tested for HIV in 2013, with minimal progress in ensuing years. 6 Contributing to the low test uptake is a complex array of individual (fear, and low perceived risk), 7,8 social (insufficient social support), 8 and structural level (poor access to testing) barriers that persist in traditional approaches to HIV testing that often ignore developmental stages and the diverse needs of young people. Eliminating these barriers to promote HIV testing among youth would require novel approaches. Moreover, for such novel approaches to be appealing and sustainable, the designed and implemented interventions should be in partnership with the youth themselves, as this has been found to be effective. 1,9,10
HIV self-testing (HIVST), a process whereby an individual performs their own HIV test and interprets their test result discretely without presenting to a health facility, 11 has shown potential to reach youth who may not otherwise test. 12,13 Due to the large body of evidence that points to its effectiveness and benefits, the World Health Organization (WHO) as well as the Nigerian National HIV and AIDS strategic framework 2019–202114 recommends HIVST as an alternative to traditional HIV testing services as one way to increase uptake of testing in young people. However, despite the release of country-specific guidelines, 14 increased donor investment, and price reductions of HIVST kits in the public sector, 15 significant barriers remain to uptake.
Having youth actively engaged in developing and implementing strategies to promote HIVST is an appealing approach that may enhance uptake. Participatory approaches provide an enabling environment to generate needed innovations that better reflect youth's needs while improving acceptability, effectiveness and sustainability. 16 Although there are increasing efforts to engage youth in improving HIV prevention outcomes, very few studies have actively involved youth in developing and implementing strategies to promote HIV testing. 1
Crowdsourcing, using open contests, is one such participatory approach where a group of individuals attempt to solve a problem and then share their solutions with the public. 17 –19 This approach has been used increasingly in public health 20 and may be useful in engaging youth in the development of HIVST services and could ultimately spur HIV test uptake. 21 Once participants are engaged, an apprenticeship training strategy pairs them with local experts to further build capacity for developing and implementing new youth-friendly HIVST services in real-world settings. Apprenticeship also provides the practical skills, direct mentorship, and supportive environment to increase the likelihood of launching successful HIVST services targeting youth populations. Moreover, delivering such services will involve lay and trained youth-friendly health workers in both facility and community settings. 22 By engaging youth in crowdsourcing activities and apprenticeship training, the interventions developed and implemented for youth by youth may hold key for local ownership and long-term sustainability of services over time.
In the context of HIV testing, crowdsourcing and apprenticeship training may enhance demand, reach, and uptake of HIVST by modifying individual, social, and structural barriers to testing. Thus, this pilot, quasi-experimental study aims at (1) determining the feasibility of enrolling youth, aged 14–24 years into five pilot intervention studies; (2) establishing the feasibility of retaining participants through a 6-month follow-up period; and (3) obtaining a preliminary estimate of efficacy of youth-led strategies, developed through crowdsourcing and apprenticeship training, to enhance the uptake of HIVST among youth in Nigeria.
Methods
Study design
We conducted a pilot, quasi-experimental cohort study from September 2019 to March 2020 to evaluate five different models of service delivery across seven sites as part of the Innovative Tools to Expand Youth-friendly HIV Self-Testing (I-TEST) study, known locally as 4 Youth by Youth (4YBY). We followed the template for Social Innovation in Health Research Checklist
23
to provide a detailed description of the interventions and ultimately replicability (Supplementary Table S1). The trial was registered with
Intervention development procedures
The steps for the intervention development are shown in Fig. 1. Guided by a youth participatory action research (YPAR) framework, 24 three participatory activities were implemented from October 2018 to July 2019 to inform the content and structure of the intervention. First, we conducted a crowdsourcing open call over a 7-week period, where we solicited concepts and strategies to promote HIVST. We used the WHO/TDR practical guide on crowdsourcing to inform the open call. 25

The steps for the 4YBY intervention development process. 4YBY, 4 Youth by Youth.
Next, we conducted a 48-h designathon in which pre-formed teams collaborated to design youth-friendly HIVST service strategies in a sprint-like event. A designathon is a crowdsourced approach in which small groups of people collaborate to solve a problem. 26 Both the crowdsourcing open call and designathon were judged by an expert panel of Nigerian professionals in public health, communications, civil society, and product design based on desirability to young people, feasibility to implement, and potential for impact (described in details elsewhere). 6,27,28
Finally, during our 4-week apprenticeship training (which we called an innovation bootcamp 28 ) aimed at building capacity for research and entrepreneurship, a select group of teams refined and finalized their service strategies for improving HIVST among young Nigerians. The five best-scoring strategies, in collaboration with the Nigerian Institute of Medical Research (NIMR), pilot-tested their HIVST packages across seven local government areas in Nigeria.
Intervention components and implementation
We implemented a quasi-experimental study comparing five different models of service delivery developed and implemented by trained youth research facilitators. Detailed descriptions of all five interventions' components are available in Supplementary Table S1. Common elements across the five interventions included HIVST service packages, as well as STI testing, that were sold for <1500-naira (3 USD) and youth-led organization. Participants were asked to test twice within the 6-month time period (once at 3 months and once at 6 months after baseline).
Intervention 1 (Lagos State): This intervention repackaged the standard HIVST kit to be more appealing to youth and rebranded it as a “SMART Pack.” The pack included oral HIVST kits, educational pamphlets, a referral coupon (for linkage to youth-friendly clinics for STI testing), and a wristband (to normalize HIV testing). The package was promoted at social gatherings and outreach events.
Intervention 2 (Lagos State): This intervention created a self-care box called “LUVBOX” that included HIVST kits, condoms, referral coupons (for linkage to youth-friendly clinics for STI testing), and hygiene products (panty liners for females and beard care kit for males). It was promoted at in-person outreach events in schools and local market squares.
Intervention 3 (Enugu State): HIVST kits were promoted at social community events (soccer games and dance competitions) and on social media platforms. The kits included a USSD (unstructured supplementary service data) code for users to access on their mobile phone a set of step-by-step instructions on how to use the kit in the local language, Igbo. The study team used mobile clinics to provide youth-friendly services, including STI testing.
Intervention 4 (Ondo State): The intervention repackaged the HIVST kit to also include access to local skill acquisition programs while drawing on youth ambassadors to distribute the kits in student communities and via WhatsApp messages. The youth ambassadors included individuals aged 14–24 who were able to commit to the role for the designated time period and are connected to other youths in the communities in varying capacities such as youth leaders or social influencers in public health. These individuals were well positioned to share information with their peers about the HIVST services while building community support to extend the reach and demand for HIVST among youth. They used mobile clinics to provide youth-friendly services, including STI testing.
Intervention 5 (Oyo State): The intervention provided an oral HIVST kit and an access pin code that gave the users access to a program website. This site allowed participants to redeem prizes and an opportunity to speak to a counselor trained on how to conduct the test, understand the result, and support linkage to youth-friendly clinics for STI testing.
Study population and procedures
The interventions were implemented in 4 out of the 36 states in Nigeria, namely, Lagos, Enugu, Ondo, and Oyo states across 7 geographical distinct catchment areas. For each intervention, our goal was to recruit at least 80 participants. Each state had established two youth-friendly health facilities, where participants were referred for follow-up visits that included STI testing and facility-based confirmatory HIV testing. The criteria for selecting the youth-friendly health facilities included the clinic's proximity to the study site location, the number of young clients they serve and whether they offer comprehensive sexual and reproductive health services (including STI testing) to youth.
Study participants eligibility criteria included (1) being 14–24 years old; (2) self-reported HIV negative or unknown HIV status; (3) able to speak and understand English; (4) willing and able to provide informed consent; and (5) have a mobile phone. Recruitment occurred through a combination of community-based events, social media platforms, and peer referral. The studies were organized by groups of 3–5 paid trained youth research facilitators at each site. The trained youth research facilitators were responsible for recruiting study participants, facilitating intervention delivery and data collection.
In addition, each site received supportive supervision and mentorship through a series of participatory learning community (PLC) sessions. Guided by the Institute of Health Breakthrough Series, 29 the PLC was organized around the Plan-Do-Study-Act (PDSA) cycles wherein teams across all the study sites collaborated to identify problems and barriers to implementation, define a strategy that can produce change, test the strategy, and use locally generated data to determine and compare across sites if the change yielded a process improvement. The PLC sessions were also used to enhance ongoing implementation across the study sites and evaluate adherence and fidelity to the study protocol. The PLC sessions were co-organized by NIMR technical staff and youth research facilitators.
Potential participants were approached by a trained youth research facilitator and asked permission to screen them for study eligibility. Interested eligible participants were given an appointment for an intake where they were enrolled and underwent baseline assessment after providing informed consent. On completing the baseline assessment, participants received either one of the five package of services based on the catchment area (Lagos, Oyo, Ondo, or Enugu state) in which the participant reside and the intervention is implemented. All enrolled participants were followed for 6 months.
Retention and follow-up
Participants were contacted via SMS (short message service) text message and phone calls 3 and 6 months after baseline. Participants were also asked to complete a follow-up evaluation that included facility-based STI testing and a survey. Those with a positive HIVST result during the study assessments were encouraged to link to care for confirmatory HIV testing by a study team member.
Outcomes
The primary outcome was uptake of HIVST that was assessed at 3 and 6 months post-intervention based on self-reported data collected through a structured questionnaire. The STI testing uptake, including testing for chlamydia, gonorrhea, syphilis, and hepatitis B, was a secondary outcome. The STI testing uptake was assessed at baseline and 6 months through self-reported data and administrative records at the participating youth-friendly clinics.
Baseline and follow-up assessments also included question about sexual behaviors, including condom use, HIV and STI testing history, and youth participation quality and experience. We used the modified 12-item Tiffany-Eckenrode Program Participation Scale 30 to assess the extent to which youth were substantially engaged and valued. The intervention feasibility is described in a Consolidated Standards of Reporting Trials (CONSORT) diagram, 31 which illustrates results for enrollment and retention. Definitions of primary and secondary outcomes and detailed methods of assessments can be found in Table 1.
Definitions of Primary and Secondary Outcomes
STI, sexually transmitted infection.
Statistical analysis
Given that this pilot data was meant to inform the subsequent randomized controlled trial (RCT), we did not conduct a formal size calculation and the analyses were not designed to have a specified level of statistical power. 32 Descriptive statistics were calculated as frequencies and percentages for categorical variables and means and standard deviations (SDs) for continuous variables. Changes in primary and secondary outcomes between baseline and 6-month follow-up were assessed by using χ 2 tests for categorical variables. Youth participation measures are presented as mean ± SD, with higher mean scores (maximum of 4) indicating more highly engaged program participation.
Mixed-effect logistic regression models (SAS procedure glimmix) with logit as the link function was applied, while controlling for age, gender, education, employment, income, ethnicity and ever had sex. An interaction term between intervention and time was included in the model to compare study outcomes between baseline and follow-up. The generalized linear mixed model uses random effects to account for the correlated repeated measures at the baseline and follow-up.
Ethical consideration
Ethical approvals for the study were granted by the Saint Louis University and the NIMR Institutional Review Boards.
Results
Of the 950 individuals assessed for eligibility, 407 were deemed eligible, of whom 388 were enrolled and completed baseline assessments (Fig. 2). Intervention 5 withdrew from the study at 2 months and did not complete the study. However, the enrolled participants (
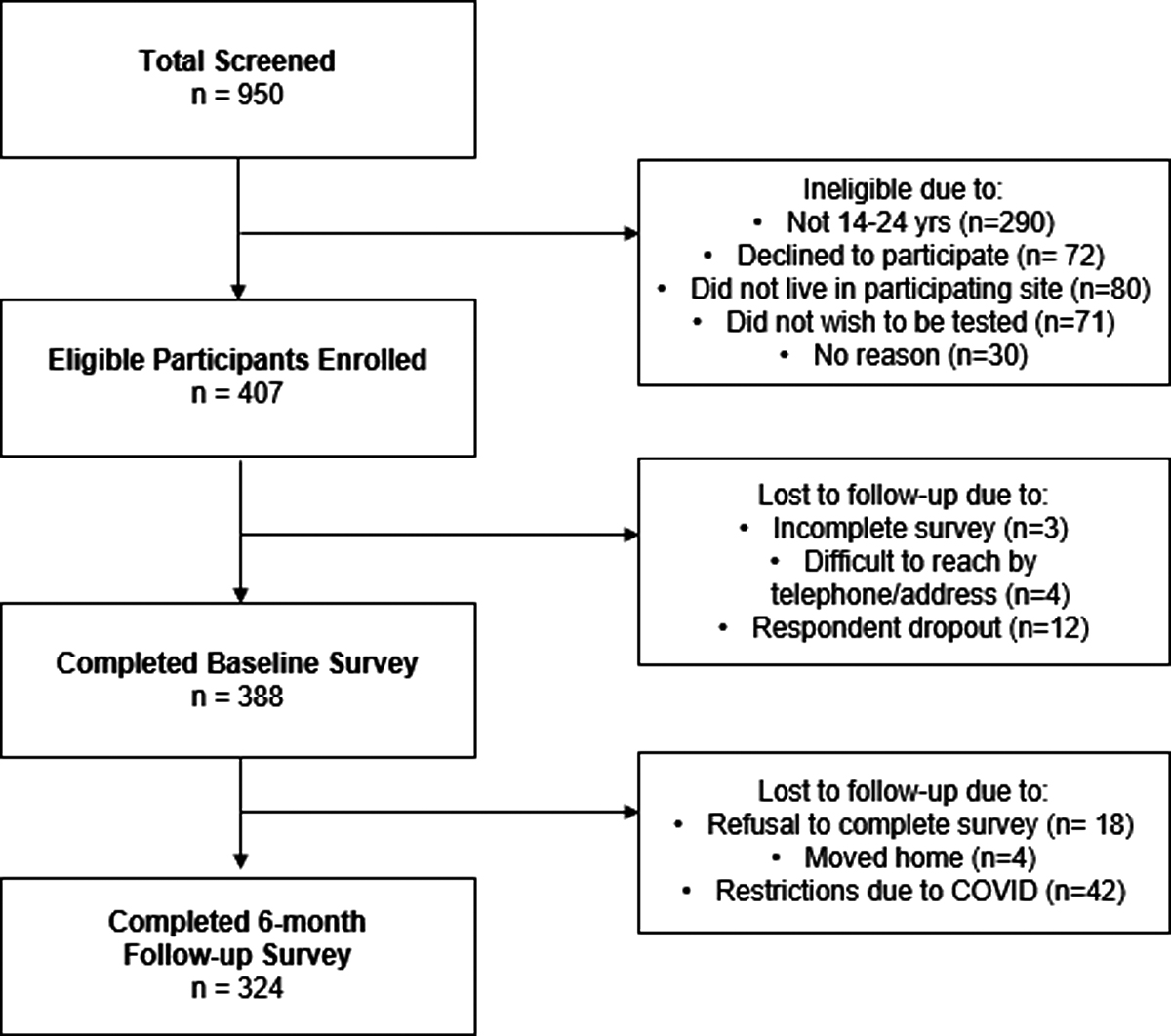
Flow diagram of participant recruitment process and follow-up for the I-TEST/4YBY study. 4YBY, 4 Youth by Youth; I-TEST, Innovative Tools to Expand Youth-friendly HIV Self-Testing.
Baseline Sociodemographic Characteristics, Sexual Behavioral Factors, HIV, and Sexually Transmitted Infection Testing Behaviors Among 388 Youth Enrolled in the Innovative Tools to Expand Youth-Friendly HIV Self-Testing Study, 2019–2020
SD, standard deviation.
About three-quarter (75.0%) earned an average monthly income of less than ₦50,000 as compared with the national average monthly income of ₦43,200 (USD 111) in 2020.
33
At baseline, 168 (43.3%) youth had ever had any form of sexual intercourse (oral, anal, or vaginal), and 59 (15.2%) reported consistent condom use during sexual intercourse in the past 3 months before the study. At baseline, the overall proportion of first-time testers (with no previous testing history) was 84.0% (
Retention was high, with 83.5% (324/388) of enrolled participants completing the final study assessment at 6 months. Primary reasons for non-retention included restrictions due to COVID-19, being non-locatable and relocating as the majority of our study participants were students.
Statistically significant positive increases were observed for HIVST as well as STI testing (Fig. 3). The uptake of HIVST increased from 19.9% (
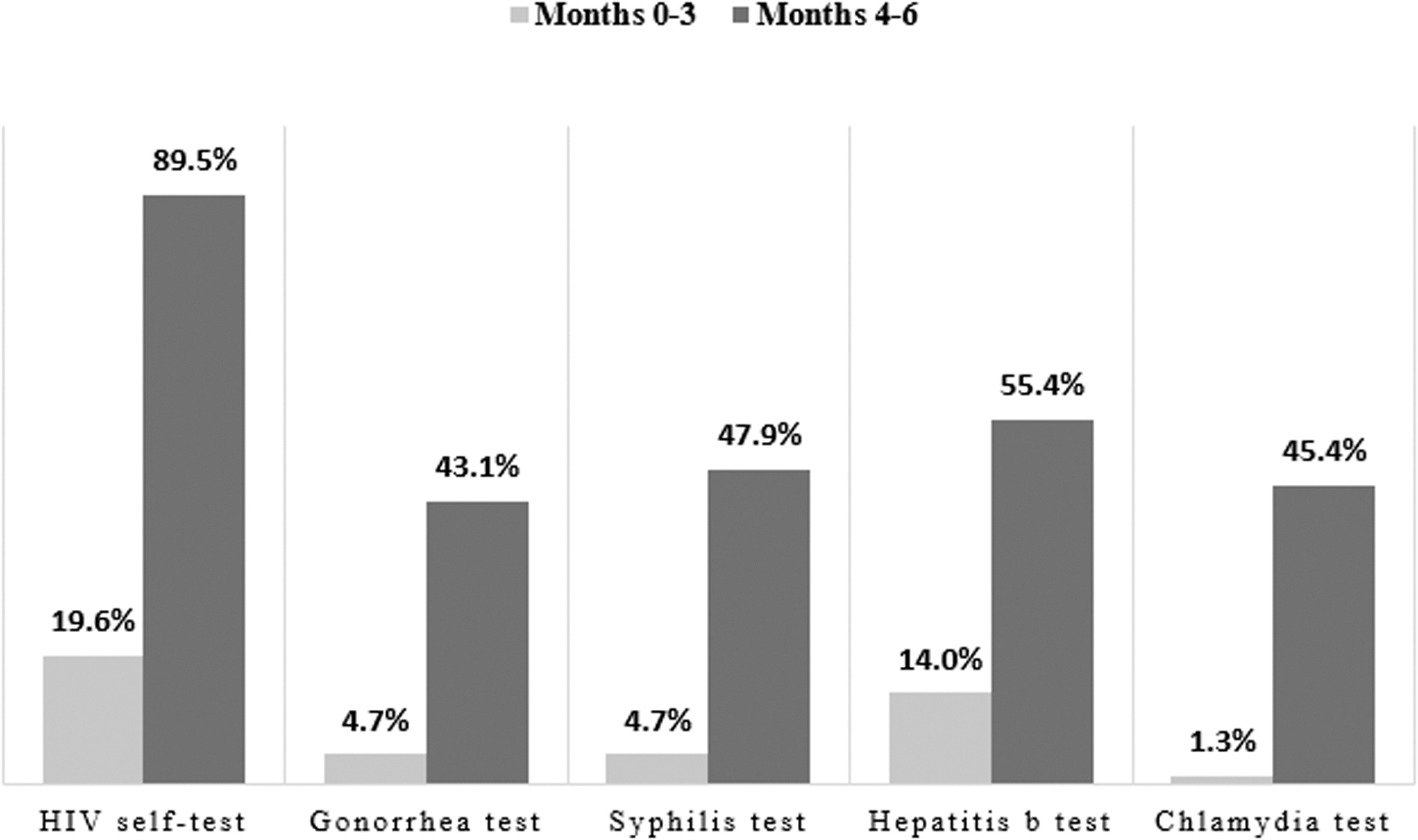
Increase in HIV and STI testing. STI, sexually transmitted infection.
There was no statistically significant difference in the past 3-month self-reported condomless sex between 3- and 6-month follow-up (33.2% vs. 31.2%,
Change in Uptake of HIV and Sexually Transmitted Infection Testing Services Among Participants During 6-Month Follow-Up
There were 311 participants with at least 1 measurement in unadjusted (bivariable) analyses.
Adjusted for age, gender, education, employment, income, ethnicity, and ever had sex.
CI, confidence interval; OR, odds ratio.
Table 4 summarizes the mean ratings for quality of youth participation. The mean participation rating was 3.1 (SD = 0.6), which represented strong agreement that the interventions promoted youth ownership, voice/influence, support, and engagement in HIVST services (see Supplementary Table S3 for full scale ratings).
Ratings for Youth Participation Sub-Scales
All Likert responses ranged from 0 to 4, with higher scores indicating strong agreement (0, Strongly disagree; 1, Disagree; 2, Neither agree nor disagree; 3, Agree; 4; Strongly agree).
SD, standard deviation.
Discussion
Findings from our pilot study provide promising evidence of efficacy that youth-led, crowdsourced strategies led to higher uptake of HIV and STI testing. Our study extends the existing literature by applying crowdsourcing to implement youth-developed strategies to promote HIV/STI test uptake, as well as apprenticeship training to build capacity and provide mentorship necessary to implement and evaluate their strategies among other young people in real-world settings. Most HIV testing programs for youth have been adapted from adult testing assumptions, and many suffer from limited youth engagement. 1
Our pilot trial addresses this important gap by providing much-needed evidence and mechanisms that foster meaningful youth engagement in HIV prevention research among high-risk population in sub-Saharan African settings. Although Nigeria is already close to reaching the 90% target of HIV diagnosis in adults, it is unlikely to achieve the 95% target among youth (10–24 years) by 2030 in the absence of youth-friendly HIV prevention service strategies such as youth-led, community-based HIVST service delivery.
Preliminary efficacy data suggest that the interventions were associated with a substantial increase in HIVST uptake and re-testing at the 6-month follow-up. Specifically, data from the 6-month follow-up visit show high readiness to retest, as well as a reduced number of first-time testers. The proportions of HIVST uptake are also similar to that reported in previous community-based HIVST studies conducted in South African and Malawi, where rates among youth were reported to be 90–100%. 34,35 The retesting rate in the South African study was comparable to our study, with most participants (96%) reporting to have repeated HIVST at 9 months. 35
Our results, together with previous research studies, suggest that youth-led HIVST interventions are feasible and could be an effective strategy to generate demand for HIV testing services among youth population. In addition, the ability of the youth-led HIVST distribution strategy to reach first-time testers or infrequent testers suggests the potential for increasing testing coverage among those that conventional, facility-based testing services do not reach.
Our study findings demonstrate that the youth-led, HIV prevention services significantly increased uptake of STI testing at 6 months. However, previous research reported mixed evidence on improving access to and uptake of STI testing with HIVST, 36 with two studies reporting no effect between intervention and control groups 37,38 and one study reporting significant reductions in STI testing. 39 The increase in uptake of STI testing in our study may be attributable to the availability of information, education, and communication materials for the participants and the relative integration of STI testing as part of the HIVST services.
In low- and middle-income countries (LMICs), utilization of facility-based testing services among youth is suboptimal and youth often face sociocultural and structural barriers to accessing services, including lack of convenience, stigma, cost of services, and poor health literacy. 40 Although young people in this setting are regularly exposed to information on HIV through school curriculum programs or other community outreach events, much less attention has been paid to STIs. Moreover, studies conducted in Nigeria among young people suggest moderate to low levels of knowledge about STI prevention, symptoms, and transmission. 41,42
These findings suggest an opportunity to leverage the wide availability of HIV services by integrating STI preventive services and more generally sexual and reproductive health services designed for youth by youth themselves.
Our results point to the significant potential benefits of youth having substantial decision-making power while engaging them extensively in intervention development, planning, and implementation. The strength of HIVST is heightened by using novel youth participatory approaches whereby the youth themselves developed HIVST interventions through crowdsourcing open calls and were further trained in a 4-week innovation bootcamp to implement and evaluate the intervention in real-world settings. Our approaches demonstrate that by simultaneously engaging youth while addressing their unique care-seeking needs, it is possible to substantially spur uptake of HIV/STI testing, even in a resource-constrained setting.
Combining HIV and STI testing with effective follow-up strategies is important to ensure that individuals remain HIV-uninfected or facilitate linkage to appropriate services following a positive diagnosis. 43,44 Across the intervention groups, individual-level follow-up (i.e., referral coupons) and digital tools (i.e., USSD, WhatsApp, and other social media platforms) were leveraged to collect HIVST usage and provide linkage information to study participants.
These strategies are timely in the light of increased recognition on the importance of developing pragmatic approaches to monitor HIVST usage and linkage as countries consider scale-up and adoption of HIVST policies. 45 In future iterations of the intervention, we plan to utilize mobile applications to confirm test uptake across larger geographical regions, as well as incorporate other mhealth platforms, such as the USSD, for individuals who may have limited access to internet connectivity.
Our study has several limitations. First, the study was designed as a pilot and did not have a control group. This limits the inferences that can be made about the study findings. However, the similarity of the interventions and outcomes allowed us to pool results. Second, the use of self-report measures to assess some outcomes may have introduced recall and social desirability bias. At the same time, our primary outcome was assessed by administrative records. Third, COVID-19 complicated the timing of the 6-month follow-up, making the exact timing of the final follow-up not uniform across all youth. Finally, given that the aim of the pilot study was to provide evidence of preliminary efficacy, the sample size was relatively small, which limits any conclusions being made regarding the generalizability of findings.
Our data have implications for research and programs. In terms of research, this demonstrates that youth-led research pilots are feasible in the Nigerian context. Youth can have a key role in all stages of developing and implementing research studies. In addition, our pilot data suggest that larger trials are warranted to understand how this intervention can be implemented on a larger scale. In terms of programs, our data show how participatory approaches such as crowdsourcing open calls provide a structured mechanism for community engagement.
These activities provided a way to harness youth voices, building local ownership of the project. Nonetheless, participatory-based approaches, which promote shared decision-making between youth and researchers on intervention development and implementation. Findings from our pilot study demonstrated sufficient feasibility and preliminary effectiveness to justify progress to a full-scale implementation trial, with some amendments necessary. The lessons learned from the pilot study provide key insights into working with young people as partners and leaders in HIV prevention research in LMICs.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest. The sponsor played no role in the (1) study design; (2) the collection, analysis, and interpretation of data; (3) the writing of the report; and (4) the decision to submit the article for publication. No authors received payment to produce the article.
Funding Information
The study is funded by Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Grant number: UG3HD096929. The authors are also funded by the National Institute of Mental Health (R00MH104154, R34MH109359, and R34MH119963) and the National Institute of Allergy and Infectious Diseases (P30AI50410 and K24AI143471).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.