
Abstract
This study examined the relationships between perceived public stigma, experienced stigma, and quality of life in people living with HIV (PLHIV), and whether self-stigma mediates these relationships. Cross-sectional data were analyzed from 1704 PLHIV in care at OLVG hospital in the Netherlands. We measured different types of stigma (perceived public stigma, experienced stigma, and self-stigma), and various quality-of-life outcomes (disclosure concerns, depression, anxiety, sexual problems, sleeping difficulties, self-esteem, general health, and social support). Structural equation modeling was used to test the paths from different types of stigma to quality-of-life outcomes. All direct effects of self-stigma on quality-of-life outcomes were significant. The final mediation model showed that the effects of both perceived public and experienced stigma on quality-of-life outcomes were mediated by self-stigma. These findings highlight the importance of addressing self-stigma in PLHIV, and call for (psychosocial) interventions that reduce the harmful effects of HIV-related stigma.
Introduction
HIV has gradually transitioned into a chronic rather than life-threatening condition as a result of major advances in treatment development and access to antiretroviral therapy. 1,2 However, despite significant improvements in efforts to end the epidemic, critical issues for people living with HIV (PLHIV) remain. Globally, HIV-related stigma continues to be an important barrier to both effective HIV treatment and prevention initiatives. 3,4 Research further suggests that stigma compromises the quality of life of PLHIV. 5 –10 Quality of life is a multi-dimensional construct that encompasses physical, psychological, and social dimensions of life. 11
Literature on HIV-related stigma finds its roots in the early work of Erving Goffman (1963), 12 who defined stigma as “the discrediting of individuals based on an undesirable attribute.”(p3) Today, HIV-related stigma is characterized by various forms of stigma that can be encountered by PLHIV, including public stigma and self-stigma (also referred to as internalized stigma). 13,14 Public stigma entails the negative beliefs held in society about HIV, negative emotional reactions such as anger or disgust, and negative behaviors such as avoidance or abuse toward PLHIV. 15,16 Public stigma can be perceived as well as experienced (i.e., discrimination or enacted stigma). Self-stigma occurs when a person with a stigmatized condition is aware of public stigma, and internalizes the negative beliefs in society and accepts their validity. 17 –19 In this sense, self-stigma is the product of public stigma. Previous studies have found that self-stigma manifests in multiple ways including feelings of shame or feeling dirty, as well as guilt and fear. 20,21
Stigma, both public and self-stigma, is highly detrimental. Stigma is linked to negative psychological, social, and physical health outcomes (e.g., depression, anxiety, lower self-esteem, disclosure concerns, reduced social support, sexual problems, sleeping difficulties, and poorer general health) across different countries and key populations including individuals with a migration background, men who have sex with men (MSM), women, and people with substance use dependence. 8,13,14,19,22 –30
Over the years, there has been substantial research on how the psychological, social, and health aspects of quality of life are impacted by public stigma or by self-stigma, but there is little research that has investigated whether quality-of-life outcomes are impacted by public stigma through self-stigma. Conceptual models of stigma put forth by Pryor and Reeder 15,16 and Berger et al. 17 posit that PLHIV who perceive or experience HIV-related stigma are more likely to internalize stigma, and this consequently leads to poorer quality of life across psychological (depression, anxiety, and self-esteem), social (disclosure concerns, social support), and health (general health, sexual problems, and sleeping difficulties) dimensions. As a result, in this study with large sample of PLHIV in the Netherlands, we hypothesized that self-stigma mediates the pathways from both perceived public stigma and experienced stigma to quality-of-life outcomes.
Further, with the knowledge that social support can buffer against stigma and its impacts, 30 –34 we further hypothesized that the pathways from both perceived public stigma and experienced stigma to self-stigma are moderated by social support. This is new. Research on the role of social support for PLHIV has focused predominantly on the relationship between social support and stigma 30,32 or on relationships between social support and quality-of-life outcomes. 33 One study, by Brener and colleagues, 34 investigated social support as a moderator in the relationship between HIV-related stigma and health outcomes but, to our knowledge, no previous study has explored the possible buffering effect of social support in the relationship between public stigma and self-stigma. Theoretically, it makes sense that social support can protect PLHIV from the internalization of negative beliefs about HIV and PLHIV, as public stigma is at the core of all other forms of stigma, including self-stigma. 35 Hence, our hypothesis.
Disentangling how various forms of stigma work to impact quality-of-life outcomes across psychological, social, and health dimensions, and whether social support can buffer against the internalization of public stigma is not only theoretically important, it is important for the design of effective interventions that reduce stigma and improve quality of life in PLHIV. 5,36
Methods
Participants and procedures
Data for this study were drawn from a cross-sectional survey of 1704 PLHIV recruited from the Department of Internal Medicine of OLVG Hospital in Amsterdam in the context of a holistic HIV care trajectory. 37 Participants were eligible for the study if they were at least 18 years of age, and if they were able to complete the survey in Dutch or English. Of the ∼3000 patients invited to participate, 1704 completed the survey (57%). Informed consent was obtained. Demographic characteristics (gender, age, region of origin, HIV transmission route, and time since diagnosis) were retrieved from medical records. Data collection took place between 2016 and 2018. Surveys were completed online or offline during hospital visits. Ethical approval for this study was granted by the ethical review board of OLVG Hospital in the Netherlands.
Measures
HIV-related stigma
HIV-related stigma was measured using an adapted version of the 40-item HIV stigma scale developed by Berger et al., 17 namely the short 10-item HIV stigma scale. 38 The 10-item scale measures public attitudes, personalized stigma, negative self-image, and disclosure concerns. Answers were provided on a 4-point scale ranging from 1 to 4, with higher scores indicating greater stigma. This scale is a frequently used measure of HIV-related stigma and is considered both valid and reliable. 38,39 For this study, we utilized each subscale individually because they represent different forms of stigma. We drew items from the short HIV stigma scale that reflect the concepts of perceived public stigma, experienced stigma, and self-stigma.
Perceived public stigma was measured using the two-item subscale “public attitudes.” An example item is “Most people with HIV are rejected when others find out.” Cronbach's alpha was 0.84. Experienced stigma was assessed using the three-item subscale “personalized stigma.” An example item is “I have lost friends by telling them I have HIV.” Cronbach's alpha was 0.84. Self-stigma was measured using the three-item subscale “negative self-image.” An example item is “Having HIV makes me feel that I'm a bad person,” Cronbach’ alpha was 0.89.
Quality-of-life outcomes
Staff at OLVG Hospital specialized in HIV care, together with PLHIV and experts in psychosocial and health aspects of living with HIV, identified eight crucial aspects of quality of life for PLHIV. These aspects were also considered to be clinically relevant to the provision of patient-centered health care. The eight aspects represent psychological, social, and health dimensions of quality of life. 37
Disclosure concerns were assessed using the two-item subscale “disclosure concerns” of the HIV stigma scale. 38 In the analysis, we treated disclosure concerns as a quality-of-life outcome instead of a type of stigma because previous studies have found internalized stigma in PLHIV to be a significant predictor of disclosure concerns. 25,39,40 An example item is “I am very careful who I tell that I have HIV.” Cronbach's alpha was 0.66.
Depression and anxiety were measured using the 14-item Hospital Anxiety and Depression Scale (HADS), 41 comprising 7 items for depression and 7 items for anxiety. An example item for depression is “I still enjoy the things I used to enjoy.” An example item for anxiety is “I get sudden feelings of panic.” Answers were provided on a 4-point scale ranging from 0 to 3, with higher scores indicating higher levels of depression and anxiety. The HADS is a frequently used measure of depression and anxiety. Cronbach's alpha for both depression and anxiety was 0.83.
Sexual problems were measured with a nine-item scale developed based on the model of incentive motivation 42 and the Natsal-SF. 43 The scale measures sexual functioning and experience, sexual feelings, and sexual satisfaction. Answers were provided on a 5-point scale ranging from 1 to 5, with higher scores indicating greater sexual problems. An example item is “Do you feel anxious about having sex because you are afraid of passing HIV to others?” Cronbach's alpha was 0.81.
Sleeping difficulties were measured using the three-item Symptom Checklist 90 Revised. 44,45 Answers were provided on a 5-point scale ranging from 1 to 5, with higher scores indicating more sleep difficulties. Items included questions related to trouble falling asleep or disturbed sleep. Cronbach's alpha was 0.80.
Self-esteem was measured using the Single-Item Self-Esteem Scale (SISE), 46 namely “I have high self-esteem” with scores ranging from 1 to 7. A higher score indicates more self-esteem. The scale demonstrated high construct validity. 46
General health was assessed using the 12-item Short Form Health Survey. 47 The scale measured physical and mental health domains. Scores range from 0 to 100, reflecting worst to best health. An example item is “Have you been able to concentrate on what you are doing?” This scale has been used extensively and is considered both valid and reliable. 47 Cronbach's alpha was 0.90.
Social support was assessed using the 12-item short version of the Social Support List-Interaction 48 that measures everyday support, support in problem situations, and esteem support. The scores range from 12 to 48, with higher scores indicating more social support. An example item is “Does it ever happen to you that people show they are fond of you?” This scale is a frequently used measure of social support. Cronbach's alpha was 0.92.
Data analysis
We first conducted a missing data analysis using the expectation maximization likelihood approach because 3.87% of the data were missing due to nonresponse. Descriptive analyses were then conducted for all variables in our sample. A regression analysis was used to test whether moderation of social support in the interaction between perceived public stigma, experienced stigma, and self-stigma was present.
Structural equation modeling (SEM) was used to test paths from different types of stigma (independent variables) to quality-of-life outcomes (dependent variables). We examined (1) direct effects of perceived public, experienced stigma, and self-stigma on quality-of-life outcomes, and (2) indirect effects of perceived public and experienced stigma on quality-of-life outcomes through self-stigma. The Lavaan package 49,50 was used to test how well the stigma mediation model fitted the data and whether there were any relevant indirect effects present. Model fit was determined using the Tucker Lewis Index (TLI), the standardized root mean square residual (SRMR), and the root-mean-square error of approximation (RMSEA). Cutoff values of 0.95 for the TLI 51,52 and 0.06 for the RMSEA and the SRMR 53 indicate a good fit, and an adequate fit is indicated when TLI exceeds 0.90, and when RMSEA and SRMR are <0.08. 51,53 For this study, statistical significance of the (indirect) effects was obtained by computing the 95% confidence intervals around the parameter estimates. The adjusted (bias-corrected) bootstrap percentile (bca) method was used to obtain the confidence intervals. In our analyses, we controlled for gender, age, region of origin, HIV transmission route, and time since diagnosis.
Results
Most of the 1704 participants included in the sample were male (94%). Age ranged from 21 to 84, with a mean age of 50.7 years [standard deviation (SD) = 10.9]. The sample was culturally diverse; more than half of the participants were born in the Netherlands (62%), 22% had a non-Western migration background, 15% had a Western migration background, and 1% was unknown. The majority of the participants had acquired HIV through same sex intercourse (MSM; 87%). The mean time since diagnosis was 11.8 years (SD = 7.9).
Table 1 gives correlations, means, and SDs for all stigma and quality-of-life variables. Pearson correlation analyses indicated that self-stigma was significantly and positively related to other types of stigma (perceived public stigma r(1702) = 0.55, p < 0.01, experienced stigma r(1702) = 0.47, p < 0.01). Self-stigma was also significantly related to all domains of quality-of-life outcomes, and showed a positive association with disclosure concerns, depression, anxiety, sexual problems, and sleeping difficulties [rs(1702) ranging from 0.31 to 0.48, p < 0.01]. Finally, self-stigma was negatively associated with self-esteem, general health, and social support [r(1702) = −0.29, −0.40, −0.29, p < 0.01]. Similarly, perceived public stigma and experienced stigma were positively associated with disclosure concerns, depression, anxiety, sexual problems, and sleeping difficulties [rs(1702) ranging from 0.21 to 0.51, p < 0.01], and negatively related to self-esteem, general health, and social support [rs(1702) ranging from −0.19 to −0.34, p < 0.01].
Correlations, Mean Scores, and Standard Deviations of All Stigma and Quality-of-Life Variables in People Living with HIV Sample (N = 1704)
All correlations are significant with p < 0.01.
α, Cronbach's alpha; M, mean; SD, standard deviation.
SEM results
Regression analysis was conducted to examine the moderating effect of social support in the pathways from perceived public stigma and experienced stigma to self-stigma. The analysis indicated that the interaction terms were very small for both experienced stigma [b = −0.009; standard error (SE) = 0.003] and for perceived public stigma (b = −0.005; SE = 0.003). Therefore, moderating effects were ignored in subsequent analyses. However, social support was added as a covariate in the model because it had an effect on the quality-of-life outcomes.
The final structural model (without interactions) fitted the data well: (χ 2 (12) = 57.9, TLI = 0.970, SRMR = 0.024, RMSEA = 0.047). SEM results are presented in Fig. 1 and Table 2. Figure 1 shows the significant standardized direct effects, with smaller effects (<0.20) omitted. The 12 indirect effects in this model (1 for each combination of independent and dependent variable) are displayed in Table 2. Two direct effects were added to this model (perceived public stigma to disclosure concerns and experienced stigma to disclosure concerns) to obtain a good fit. This was necessary because a model with only indirect effects could not fully explain the correlation between experienced and perceived public stigma, on one hand, and disclosure concerns, on the other.
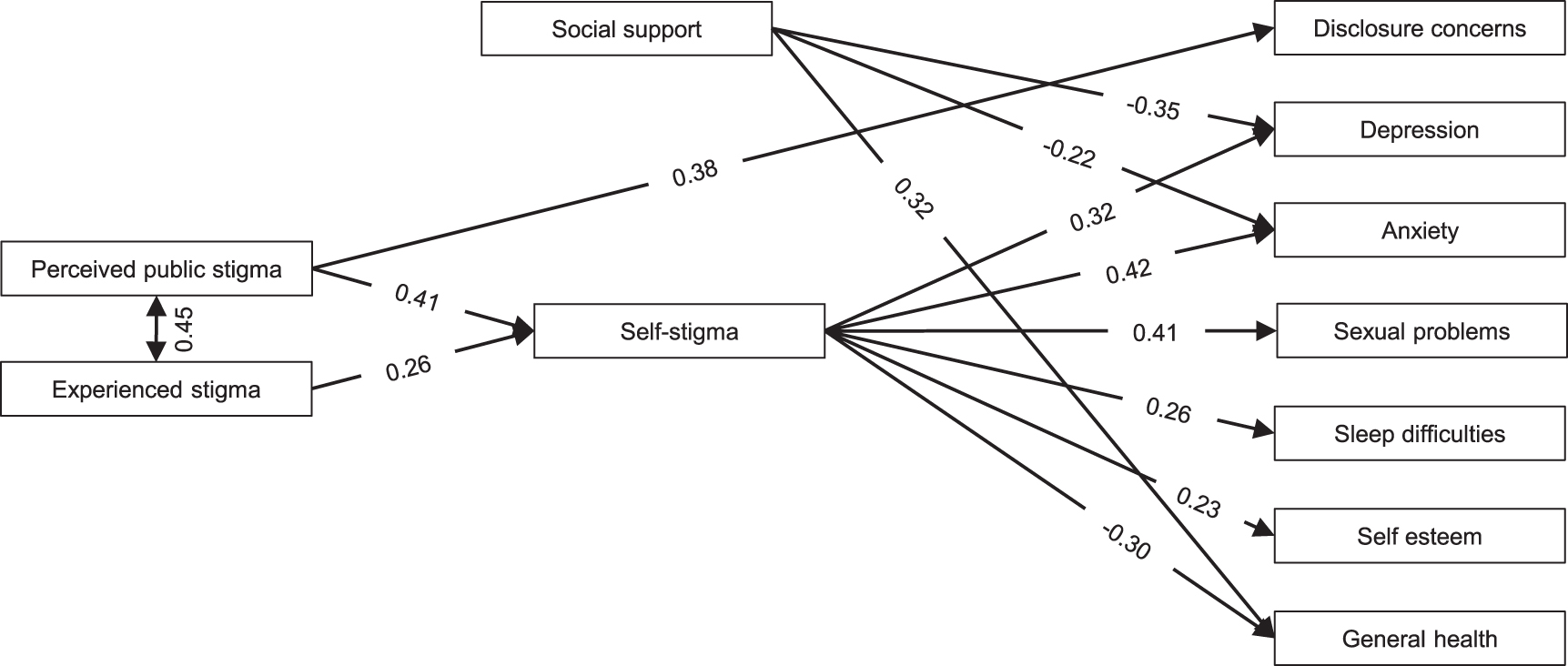
Self-stigma mediation model with standardized parameters showing direct effects. The lines with arrows show all direct effects in the mediation model. Only effects of 0.20 or higher are shown in the figure.
Estimates of Standardized Indirect Effects Through Self-Stigma in Mediation Model (Structural Equation Modeling)
These are direct effects and were added because they were necessary to obtain a good fit.
CI, confidence interval.
Results displayed in Fig. 1 and Table 2 illustrate the size of the indirect effects through self-stigma of both perceived public stigma and experienced stigma on quality-of-life outcomes, indicating a mediating effect of self-stigma in the relationship between, on one hand, perceived public stigma and experienced stigma and, on the other, quality of life. The indirect effects of perceived public stigma were larger than those of experienced stigma. Tables showing all direct pathways from self-stigma and social support to quality-of-life outcomes as well as explained variance of the model for all dependent variables are presented in the supplementary material.
Discussion
This study set out to explore a comprehensive model of HIV-related stigma and its impact on quality of life in PLHIV. We found that self-stigma mediates the relationships between perceived public stigma and experienced stigma, on one hand, and quality-of-life outcomes, namely disclosure concerns, depression, anxiety, sexual problems, sleeping difficulties, self-esteem, and general health, on the other hand. To date, there are a limited number of studies investigating how stigma types influence each other and the lives of PLHIV. 21 Prior research does indicate that HIV-related stigma directly affects the quality of life of PLHIV negatively. 14,19,21,24,54,55 Corroborating this, we found that both public stigma and self-stigma had direct effects on all quality-of-life outcomes. Our results extend previous work on HIV-related stigma and quality of life by highlighting that perceived public and experienced stigma negatively affect quality of life through its impact on self-stigma.
In our study, perceived public stigma and experienced stigma predicted higher self-stigma, which is in line with prior research in which perceived community stigma was found to predict self-stigma in women living with HIV in a health care setting. 56 Supporting these findings, experienced stigma has also been found to be associated with self-stigma in PLHIV. 57,58 In our study, perceived public stigma was found to be a stronger driver of self-stigma than experienced stigma. This may be due to the way in which self-stigma is generally understood, namely as the internalization of stigmatizing beliefs in society. 16,26,59 It is possible that perceived negative beliefs more directly affect the self because perceived beliefs are potentially more likely than actual experiences of stigma to generate feelings of fear or anticipation of being stigmatized.
Our findings further show that social support was strongly related to some of the quality-of-life outcomes, namely depression, anxiety, and general health. This partly aligns with recent research that highlights social support as a protective factor against stigma and negative (mental) health outcomes. 30,33,37,60 However, social support did not act as a moderator in our model, as we hypothesized, and the role of social support in the relationship between stigma types could not be explained. Previous research with PLHIV has identified a buffering effect of social support on perceived stigma, 32,61 and the same effect of social support on self-stigma, 30 but the role of social support within relationship dynamics of different stigma types requires further study. Specifically, we recommend that future research further investigates the role that social support and other potential buffers (e.g., empowerment and resilience strategies) can play in reducing different types of stigma in PLHIV to clarify its potential for ameliorating the negative effects of different types of stigma. We further recommend exploring the possible moderating effects of different facets of social support (such as everyday support or support in problem situations) on different types of stigma.
Our study is unique in that it focused on pathways from HIV-related stigma to quality-of-life outcomes, and the role of self-stigma within this process. To our knowledge, the only comparable research was conducted by Turan et al. 19 That study examined the mediating role of self-stigma in the relationship between HIV-related public stigma and affective, cognitive, and mental health (with significant indirect effects found) and treatment adherence (with no significant indirect effect found). Our study builds on this and further conceptualizes the relationships between perceived public stigma, experienced stigma, self-stigma, and the quality of life of PLHIV in mental, social, and health domains.
Our findings clearly suggest that efforts to reduce HIV-related stigma and improve the quality of life of PLHIV should include strategies specifically addressing self-stigma. Strategies to reduce self-stigma include cognitive behavioral therapy, psychoeducation, enhancing social and peer support, and other empowerment techniques. 26,62 –65 However, prior research reveals a shortage of high-quality interventions targeting HIV-related self-stigma. 26,62,66,67 A recent systematic review by Pantelic et al. 26 indicated that multi-leveled interventions are likely to be more effective in reducing self-stigma among key populations living with HIV. We recognize that drivers of self-stigma may vary across cultures and contexts. Therefore, we recommend that future studies on HIV-related self-stigma focus on examining other potential (sociocultural) drivers of self-stigma for different PLHIV to better inform interventions. This is important because self-stigma in PLHIV is also influenced by broader structural and social inequalities. 68,69 It may also be important to address the relationship between HIV-related stigma and substance use. Recent studies have drawn attention to high rates of substance use and related (mental) health problems in PLHIV, especially among MSM. 70,71
The findings of this study should be interpreted in light of some limitations. First, the data in our study were derived from an urban region in the Netherlands and consisted of predominantly MSM, therefore, limiting the generalizability of our findings to other key populations living with HIV. However, the demographic composition of our sample is typical for the Dutch PLHIV population, of which the majority are MSM. Second, bias toward nonresponse should be noted with regard to both missing data in our sample and those who refused to participate. Nonresponse may be due to language or cultural barriers as the HIV patient population at OLVG hospital is also highly culturally diverse. Future studies should focus on finding ways to include harder-to-reach populations. Third, our data were cross-sectional, limiting possibilities for causal inference. We recommend longitudinal studies that could further explore pathways of HIV-related stigma, sociodemographic indicators, and associated health outcomes over time.
This study showed that perceived public stigma and experienced stigma contribute to self-stigma in PLHIV, which, in turn, leads to reduced quality of life. The findings thus demonstrate the importance of addressing self-stigma in PLHIV. Future interventions that aim to reduce HIV-related stigma and improve quality of life for PLHIV should, therefore, incorporate theory- and evidence-based strategies to reduce self-stigma.
Compliance with Ethical Standards
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of OLVG Hospital in the Netherlands. Informed consent was obtained from all individual participants included in this study.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Alzbeta Kupkova, Chantal den Daas, Marie Jose Kleene, Kees Brinkman, and Guido van den Berk. Data analysis was performed by Peter Verboon and all authors contributed to the interpretation of data. The first draft of the article was written by Yvonne van der Kooij and Alzbeta Kupkova and all authors commented on previous versions of the article. All authors read and approved the final article.
Acknowledgments
We extend our gratitude to all PLHIV who completed the survey. We further thank the HIV specialist nurses and doctors at OLVG hospital for their effort in recruiting patients to complete the surveys.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by Viiv Healthcare, Gilead, and Aidsfonds (research Grant Number AF-P.42601). The funders had no role in decisions regarding the study design, data analysis, or publication.