
Abstract
Little evidence is available for the incidence of chronic kidney disease (CKD) and rate of estimated glomerular filtration rate (eGFR) decrement among Asians with low body weight who are susceptible to tenofovir disoproxil fumarate (TDF) nephrotoxicity. In this 12-year observational cohort in Tokyo, we examined 1383 treatment-naïve HIV-1-infected Asians [720 started TDF-containing (TDF group) and 663 started non-TDF-containing (control) combination antiretroviral therapy (cART)]. The CKD incidence was calculated, and the effect of TDF use on CKD development was estimated using logistic regression. The eGFR slopes, before and after cART initiation, were estimated using mixed-effects linear spline models. Most patients were males (median weight, 62.6 kg; 83% started ritonavir-boosted protease inhibitors; median observation duration, 5.08 years). CKD developed in 150 patients (10.8%), with an incidence of 20.6 per 1000 person-years [confidence interval (95% CI), 17.6–24.2]. None developed end-stage renal disease. TDF use was associated with CKD [odds ratio (OR), 1.8; 95% CI, 1.00–3.13; p = 0.052]. The cumulative mean loss in the TDF group, relative to the control, increased over time after 1, 4, and 8 years of TDF exposure (−3.8, −5.5, and −9.0 mL/min/1.73 m2, respectively; p < 0.0001). The eGFR rapidly declined during the first 3 months of cART, particularly in the TDF group (−26.4 vs. −7.4 mL/min/1.73 m2/year in the control). In the TDF group, cART introduction was significantly associated with a faster rate of eGFR decline (from −0.44 to −2.11 mL/min/1.73 m2/year; p = 0.010), whereas in the control, the difference was not significant. For HIV-1-infected Asian patients with low body weight, TDF-containing cART is associated with CKD and faster eGFR declines.
Introduction
T
Although studies have assessed the incidence and associated factors of CKD and ESRD in patients with HIV-1 infection, 7,8 such evidence is scarce for Asians with HIV-1 infection. As TDF nephrotoxicity develops in a dose-dependent manner 9,10 and low body weight is accordingly a risk factor for such toxicity, 11,12 Asians are considered to be susceptible to tenofovir nephrotoxicity due to their small body stature in general, as confirmed by studies in India, Japan, Thailand, and Vietnam. 13 –16 In fact, we have conducted a series of studies, which have shown that low body weight is a risk factor for TDF nephrotoxicity. 12,16,17 Hence, it is important to determine renal function sequelae in Asian patients exposed to long-term cART that can serve as hard end-points, such as CKD and ESRD.
Thus, in the present study, we aimed to assess the incidence and associated factors of CKD and ESRD, while particularly focusing on TDF nephrotoxicity, among treatment-naïve HIV-1-infected Asian patients, using 12-year data from an observational cohort. Moreover, we determined the rate of change in the estimated glomerular filtration rate (eGFR) after cART introduction, by using mixed-effects linear spline models, to estimate the long-term renal prognosis.
Methods
Study design and patients
We performed a single-center cohort study of HIV-1-infected Asian patients using medical records from the AIDS Clinical Center, National Center for Global Health and Medicine (NCGM), Tokyo. The inclusion criteria were (1) treatment-naivety; (2) Asian; (3) age >19 years; (4) initiation of cART at our clinic between January 1, 2004, and December 31, 2013; and (5) treatment with the recommended 300 mg/day dose of TDF in those receiving TDF-containing cART. Moreover, the exclusion criteria were as follows: (1) initiation of cART at another facility; (2) baseline eGFR <60 mL/min/1.73 m2; and (3) discontinuation of TDF or ritonavir-boosted protease inhibitor (PI/r) within 90 days of cART initiation.
Of the 1884 patients who started cART during the study period, 1383 fulfilled these criteria and were enrolled; these included 792 patients who were analyzed in our previous study. 16 The study patients were classified as those receiving TDF-containing cART (TDF group) and those receiving non-TDF-containing cART (control) and were followed up until September 30, 2015. Censoring was performed for cases with discontinuation of ART for >1 month, those referred to other hospitals, those who were lost to follow-up or those who died, or were at the end of the observation period. The selection of the cART regimen at baseline was left to the discretion of the attending physician.
The study was approved by the Human Research Ethics Committee of NCGM. Informed consent was waived because this study only used data gained from clinical practice. The study was conducted according to the principles expressed in the Declaration of Helsinki.
Measurements
eGFR was calculated using the following Japanese equation based on standardized serum creatinine, sex, and age, developed by the Japanese Society of Nephrology: eGFR =194 × [serum creatinine]−1.094 × [age]−0.287 × [0.739 if female]. 18 This equation performs better than the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation 19 in patients with small body stature. 16,20,21 The baseline eGFR was estimated for each patient from age, sex, and serum creatinine levels recorded closest to and preceding the initiation of cART, within 90 days. Patients visited our clinic at least every 3 months for monitoring of CD4 cell count, HIV-1 viral load, and eGFR since the prescription period under the Japanese healthcare system is limited to 3 months. Thus, we collected serum creatinine values measured closest to every 90 days within a range of 45 days between the first visit to our clinic and the end of follow-up for the calculation of the eGFR value. 16 The time-varying CD4 cell count and viral load were collected with the same time interval.
The potential risk factors for renal dysfunction at the initiation of cART (baseline) were recorded along with basic demographic data from the medical records. 11,22 –24 These included age, sex, height, body weight, body–mass index [BMI; body weight (kg)/height (m2)], history of AIDS (defined as history of or concurrent 23 AIDS-defining diseases, including opportunistic infections and malignancies set by the Japanese Ministry of Health, Labour and Welfare), 25 HIV-1 transmission route, baseline laboratory data (CD4 cell count, HIV viral load, and serum creatinine level), and the presence or absence of other medical conditions [concurrent use of (PIs/r); concurrent nephrotoxic drugs such as ganciclovir and sulfamethoxazole/trimethoprim, ganciclovir, foscarnet, and NSAIDs; diabetes mellitus defined as the use of antidiabetic agents; hypertension defined as current treatment with antihypertensive agents; dyslipidemia defined as current treatment with lipid-lowering agents; hepatitis B infection defined as positive hepatitis B surface antigen; hepatitis C infection defined as positive HCV antibody; and smoking]. At our clinic, body weight was measured at every visit, whereas other variables were measured at the first visit and at least once annually. We used the baseline data recorded at or closest to and preceding the start of cART, within 180 days.
Statistical analyses
The following three main analyses were performed:
(1) The incidences of CKD stage 3 (eGFR <60 mL/min/1.73 m2), eGFR <45 mL/min/1.73 m2, and CKD stage 4 (eGFR <30 mL/min/1.73 m2) were calculated by dividing the number of cases who reached the renal end-point by the total observation period. Two consecutive measurements at least 3 months apart, which fulfilled the criteria, were required for each end-point. The changes in eGFR were plotted from the baseline measurement until the occurrence of each of the three renal end-points.
A logistic regression model was used to estimate the effect of TDF use and other variables over control on the occurrence of these renal end-points. The model was adjusted for age, sex, PI/r use, baseline eGFR, baseline body weight, nephrotoxic drug use, CD4 count, and hypertension, which are established risk factors for TDF nephrotoxicity and CKD. 11,17,22,23 The model was also adjusted for the duration of cART. Diabetes mellitus and dyslipidemia were not included due to the low incidence of these conditions in the study population. This analysis was not conducted for eGFR <45 mL/min/1.73 m2 and eGFR <30 mL/min/1.73 m2 due to the small number of patients who reached these end-points.
(2) We estimated the decrement in eGFR in the TDF group relative to the control group by calculating the difference in eGFR loss between the TDF and control groups from baseline to 8 years after cART initiation, with 90-day intervals, using linear mixed models for repeated measures. 16 We constructed the model with a random effect for patients. This model also included fixed effects for the assigned treatment as well as other variables included in the logistic model described above, except for cART duration. Interaction terms for time by treatment were included.
(3) To estimate the eGFR slopes before and after cART initiation, we constructed mixed-effects linear spline models that included all eGFR values at 90-day intervals during the observation period.
7
To construct the model, we first plotted the least-square means of eGFR estimated with the linear mixed model during the study period and observed that the decrease in eGFR was substantial between baseline and 90 days after cART initiation (see Supplementary Fig. S1; Supplementary Data are available online at
Statistical significance was defined with two-sided p-values of <0.05. We used odds ratios (ORs) with 95% confidence intervals (95% CIs). All statistical analyses were performed with SAS software, version 9.4 (SAS Institute, Cary, NC).
Results
Among the 1383 study patients, 1379 received standard cART, which comprised one PI, non-nucleoside reverse transcriptase inhibitor (NNRTI), or integrase strand transfer inhibitor (INSTI) and two nucleoside reverse transcriptase inhibitors (NRTIs). Moreover, 720 started TDF-containing cART (TDF group) and 663 started non-TDF-containing cART (control group). Most of the study patients were males, with a median age of 37 years and median body weight of 62.6 kg [interquartile range (IQR), 56.4–70 kg] (Table 1).
One thousand three hundred seventy-nine patients started standard cART comprising one NNRTI, PI, or INSTI and two NRTIs. Among the other four patients, one received raltegravir plus ritonavir-boosted darunavir, one received lopinavir/ritonavir plus nevirapine, one received raltegravir plus maraviroc plus lopinavir/ritonavir, and one received fosamprenavir plus raltegravir plus abacavir/lamivudine.
BMI is missing for six patients.
Median (interquartile range).
BMI, body–mass index; cART, combination antiretroviral therapy; eGFR, estimated glomerular filtration rate; INSTI, integrase strand transfer inhibitor; IQR, interquartile range; MSM, men who have sex with men; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitor; PI/r, ritonavir-boosted protease inhibitor; TDF, tenofovir disoproxil fumarate.
There was no difference in the baseline eGFR between the two groups (p = 0.16). Further, 83.2% of the patients in the TDF group and 82.8% of those in the control used PI/r. Patients in the TDF group had higher CD4 counts (p < 0.001), were less likely to have hypertension (p < 0.001) or diabetes mellitus (p = 0.023), on concurrent nephrotoxic drugs (p < 0.001), or have a history of AIDS (p = 0.001) compared with the control group. The overall median observation period was 5.08 years, and this value was greater in the control group (median, 7.21 years; IQR, 3.62–9.22 years) than in the TDF group (median, 4.02 years; IQR, 2.53–5.95 years; p < 0.001). The median duration of TDF exposure in patients in the TDF group was 3.07 years (IQR, 1.74–4.83 years). Moreover, the overall total observation period was 7462 patient-years (3095 patient-years in the TDF group and 4367 patient-years in the control group).
During the observation period, an eGFR <60 mL/min/1.73 m2, which persisted for >3 months, occurred in 150 patients (10.8%), with an incidence of 20.6 per 1000 person-years (95% CI, 17.6–24.2) (Table 2). Seventy-one patients (incidence 23.7 per 1000 person-years) in the TDF group and 79 patients (18.5 per 1000 person-years) in the control group developed an eGFR of <60 mL/min/1.73 m2. Moreover, an eGFR <45 mL/min/1.73 m2 occurred in 11 patients (1 in the TDF group and 10 in the control group), with an incidence of 1.49 per 1000 person-years, whereas an eGFR <30 mL/min/1.73 m2 occurred in one patient in the control group, with an incidence of 0.14 per 1000 person-years. Although 48 (3.5%) patients died during the observation period, none developed ESRD that required chronic hemodialysis or renal transplantation.
eGFR, estimated glomerular filtration rate; PY, patient-years; TDF, tenofovir disoproxil fumarate.
Multi-variate logistic regression analysis indicated that TDF use was associated with eGFR <60 mL/min/1.73 m2 (OR, 1.8; 95% CI, 1.00–3.13; p = 0.052) (Table 3). Moreover, greater age, hypertension, and longer cART duration were significantly associated with eGFR <60 mL/min/1.73 m2, whereas higher baseline CD4 count, higher eGFR, and nephrotoxic drug use were inversely associated with eGFR <60 mL/min/1.73 m2.
cART, combination antiretroviral therapy; CI, confidence interval; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; OR, odds ratio; TDF, tenofovir disoproxil fumarate.
Figure 1 shows the results of the linear mixed models for repeated measures up to 8 years. The adjusted cumulative mean loss increased continuously over time in the TDF and control groups; in the TDF group, from −13.3 mL/min/1.73 m2 at 1 year to −19.6 mL/min/1.73 m2 at 4 years and to −28.6 mL/min/1.73 m2 at 8 years of TDF exposure, whereas in the control, from −9.5 mL/min/1.73 m2 at 1 year to −14.0 mL/min/1.73 m2 at 4 years and to −19.6 mL/min/1.73 m2 at 8 years of cART exposure. The adjusted cumulative mean loss in the TDF group relative to the control continuously increased over time; at 1 year of exposure −3.8 mL/min/1.73 m2, at 4 years −5.5 mL/min/1.73 m2, and at 8 years −9.0 mL/min/1.73 m2 (see Supplementary Table S1). There was a significant interaction between time and TDF use (p < 0.0001).
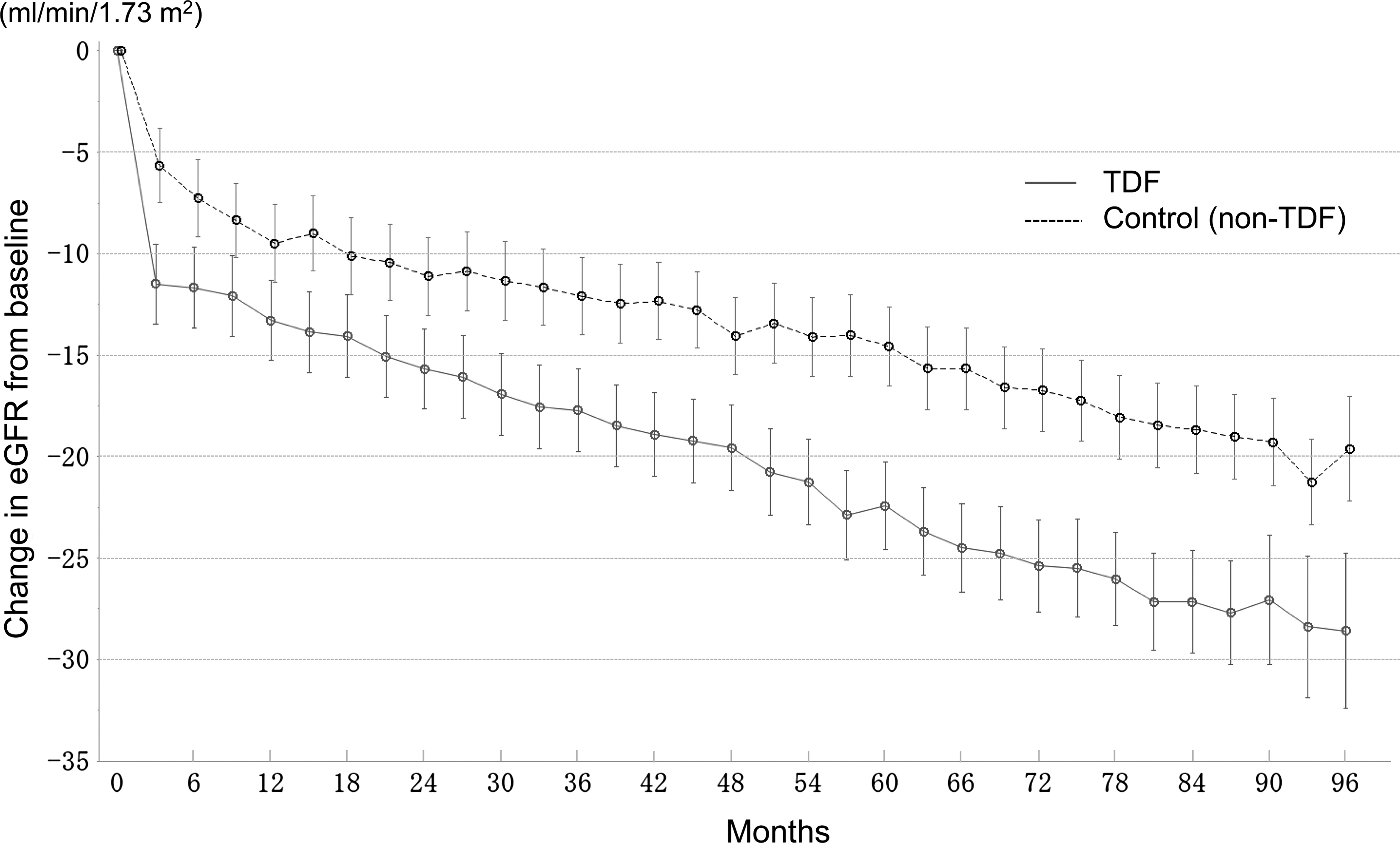
Adjusted mean change in eGFR from baseline to 8 years among treatment-naïve Asian patients after cART introduction. The black line represents the eGFR of patients treated with TDF-containing cART, whereas the dashed line represents that of controls (non-TDF-containing cART). The least-square means and their 95% confidence intervals were estimated using the linear mixed model. The x-axis is labeled with months to make the figure visually understandable; 30 days are used to represent 1 month. Thus, 3 months equal 90 days. cART, combination antiretroviral therapy; eGFR, estimated glomerular filtration rate; tenofovir disoproxil fumarate.
The analysis of eGFR slopes showed that the eGFR rapidly declined during the first 3 months after cART initiation, particularly in the TDF group (−26.4 mL/min/1.73 m2/year in the TDF group and −7.4 mL/min/1.73 m2/year in the control group); thereafter, the eGFR declined with a slope of −2.11 mL/min/1.73 m2/year in the TDF group and −1.24 mL/min/1.73 m2/year in the control group (Table 4). In all the patients, eGFR decline after the first 3 months of cART was faster than that before cART initiation, although the difference was not significant [after the first 3 months of cART: −1.88 (95% CI, −2.02 to −1.74); before cART: −1.52 (95% CI, −2.14 to −0.89); p = 0.27]. However, in the TDF group, eGFR decline after the first 3 months of cART was significantly faster than that before cART initiation [after the first 3 months of cART: −2.11 (95% CI, −2.36 to −1.86); before cART: −0.44 (95% CI, −1.66 to 0.77); p = 0.010].
cART, combination antiretroviral therapy; CI, confidence interval; eGFR, estimated glomerular filtration rate; TDF, tenofovir disoproxil fumarate.
Additional analyses of eGFR, calculated with the CKD-EPI equation, showed similar results (see Supplementary Table S2). The eGFR showed a rapid decline during the first 3 months of cART (−14.4 mL/min/1.73 m2/year in the TDF group; −5.15 mL/min/1.73 m2/year in the control group); thereafter, a decrease in the eGFR of −1.27 mL/min/1.73 m2/year and −0.57 mL/min/1.73 m2/year was observed in the TDF and control groups, respectively. In all the patients, eGFR decline after the first 3 months of cART was faster than that before cART initiation [after the first 3 months of cART: −1.16 (95% CI, −1.28 to −1.05); before cART: −0.36 (95% CI −0.63 to −0.10); p < 0.0001]. In the TDF group, eGFR decline after the first 3 months of cART was significantly faster than that before cART initiation [after the first 3 months of cART: −1.27 (95% CI, −1.47 to −1.06); before cART: 0.14 (95% CI, −0.37 to 0.65); p < 0.0001], whereas in the control group, the difference was not significant [after the first 3 months of cART: −0.57 (95% CI, −0.75 to −0.39); before cART: −0.30 (95% CI, −0.89 to 0.30); p = 0.37].
Discussion
Incidence and associated factors for CKD and ESRD were delineated in this 12-year observational cohort of treatment-naïve Asian patients. Although no patient developed ESRD, the impact of TDF use on the development of CKD and rate of eGFR decrement was evident; TDF use was associated with the development of CKD (OR, 1.8; 95% CI, 1.00–3.13; p = 0.052), and the adjusted mean loss of eGFR among patients who started TDF-containing cART relative to those who started non-TDF-containing cART continuously increased during the 8-year observation period (from −3.8 mL/min/1.73 m2 at 1 year to −5.5 mL/min/1.73 m2 at 4 years and to −9.0 mL/min/1.73 m2 at 8 years of TDF exposure). Further, after a substantial decline during the first 3 months following ART introduction (−26.4 mL/min/1.73 m2/year in the TDF group and −7.4 mL/min/1.73 m2/year in the control group), the eGFR in the TDF group continued to decline with a slope of −2.11 mL/min/1.73 m2/year, whereas that in the control group, it was −1.24 mL/min/1.73 m2/year. As the aging-related decline in renal function in healthy individuals was reported to be only 0.4 mL/min/year, this decrease in the eGFR among patients who received TDF-containing ART cannot be understated. 27
The present study has three main strengths. First, to our knowledge, this is the first study to elucidate the incidence of CKD and ESRD in HIV-1-infected Asian individuals. We found that 10.8% of the overall patients developed CKD, with an incidence of 20.6 per 1000 person-years (95% CI, 17.6–24.2). Long median follow-up period of 5.33 years is a second strength of this study; this could help determine the findings in a real-world setting as HIV-1-infected patients require lifelong cART. This incidence of CKD was approximately twofold higher than that (10.5 per 1000 person-years) reported from the D:A:D cohort of United States, Europe, and Australia (3.3% of the patients developed CKD), with a median follow-up duration of 3.7 years, 28 or that (9.6 per 1000 person-years) reported from the French cohort (3.4% of the patients developed CKD), with a median follow-up duration of 3.1 years. 29 Given that the baseline eGFR was similar among the three cohorts [the present study: median eGFR, 95.7 mL/min/1.73 m2 (IQR, 84.3–109.4); D:A:D cohort: 96 mL/min/1.73 m2 (IQR 82–111); French cohort: 101 mL/min/1.73 m2 (IQR 86–118)], further studies need to elucidate whether the susceptibility to TDF nephrotoxicity in this cohort due to low body weight (median, 62.6 kg), 16 high usage of PI/r, genetic background, or long observation period contributed to this high incidence. Although none of the patients developed ESRD during the study period, the high incidence of CKD and fast rate of eGFR decline after cART introduction (−1.88 mL/min/1.73 m2/year for the overall cohort and −2.11 for the TDF group) in this cohort warrant the careful monitoring of renal function in HIV-1-infected Asians with low body weight.
Third, this study estimated the rate of long-term declines in eGFR before and after cART introduction using a mixed-effects linear spline model. Although many studies have elucidated the prevalence or incidence of CKD in HIV-infected patients, 15,28 –30 only little evidence is available on the rate of eGFR decline based on the longitudinal eGFR data. 7 To our knowledge, only one previous study by Kalayjian et al. 7 has investigated this issue. Our results show that eGFR declines after cART introduction were faster than those before cART introduction, particularly in cases where the cART includes TDF, in contrast with the findings of Kalayjian et al., who showed that cART was associated with a significantly slower rate of eGFR decline (from −2.18 to −1.37 mL/min/1.73 m2/year; p = 0.02). However, the present study is considered to have a methodological advantage over that of Kalayjian et al. as we obtained eGFR data at 90-day intervals and could construct a graph of the least-square means of eGFR (see Supplementary Fig. S1) to understand the shape of the eGFR slope. Accordingly, a rapid decline in eGFR was observed during the first 3 months after cART introduction and the slope became approximately linear thereafter; this is consistent with the findings of several previous studies, which reported that TDF nephrotoxicity typically occurs within the first few months of exposure. 5,13,31 Therefore, we placed two knots at baseline and at 3 months after cART initiation to better estimate the slopes, whereas Kalayjian et al. used only one knot. However, due to scarcity of data, further studies are needed to confirm these findings and understand the extent to which susceptibility to TDF nephrotoxicity in this population affects the results.
In addition to the single-center nature of this study, it has some other limitations. Although this study investigated the incidence of CKD, the data on urinalysis were not available. Because persistent proteinuria is one of the diagnostic criteria for CKD and proteinuria can present in patients with normal eGFR value, 32 our findings of CKD incidence (20.6 per 1000 person-years) might be underestimated. Second, although we focused on the investigation of Asian patients, most study subjects were Japanese men, and only a small number of females were included. Third, because the data were derived from an observational cohort, there is a possibility of channeling bias due to TDF use. In fact, although baseline eGFR was not significantly different between the TDF group and the control group, patients in the control group had a greater number of risk factors for renal dysfunction compared with patients receiving TDF-containing ART. It is also noteworthy that this study excluded patients who discontinued TDF or PI/r within 90 days of cART initiation. Hence, the effects of TDF nephrotoxicity might have been underestimated in the present study. Fourth, there was high prevalence of PI/r use in our cohort, which is an established risk factor for TDF-related nephrotoxicity. 33 –35 Although it is difficult to completely exclude the impact of concurrent PI/r in this study, it should also be noted that the use of PI/r did not associate with the development of CKD in this cohort.
In conclusion, in this 12-year observational cohort of treatment-naïve Asian patients with low body weight, the incidence of CKD was high and TDF use was significantly associated with the development of CKD. The rate of eGFR decline after cART introduction was fast, particularly in cases where TDF was included in the cART. These findings warrant regular and long-term monitoring of renal function in HIV-1-infected Asian patients after cART initiation. Further large-scale studies are needed to confirm the long-term renal prognosis of Asian patients with HIV-1 infection.
Footnotes
Acknowledgments
The authors thank Masaaki DOI, Chuo University. The authors also thank Akiko Nakano (study coordinator) and all the other clinical staff at the AIDS Clinical Center for their help in completing the study.
Source of Funding
This work was supported by a grant from the National Center for Global Health and Medicine (25-106 and 27-6001) and a grant-in-aid from the Imai Memorial Trust for AIDS Research.
Author Disclosure Statement
T.N. has received honoraria from MSD K.K., Janssen Pharmaceutical K.K., Torii Pharmaceutical, Co., and ViiV Healthcare, Co. H.G. has received honoraria from MSD K.K., Janssen Pharmaceutical K.K., Torii Pharmaceutical, Co., and ViiV Healthcare, Co. S.O. has received honoraria and research grants from MSD K.K. and has received honoraria from Torii Pharmaceutical, Co., Abbie GK, ViiV Healthcare, Janssen Pharmaceutical, and Japan Tobacco INC.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.