
Abstract
Introduction:
Laboratory technicians are routinely exposed to occupational health hazards that can be a serious threat to their health. To safeguard themselves against laboratory-acquired infections, they must be aware of universal work precautions. A targeted educational intervention to increase awareness about universal precautions was designed to result in behavioral changes in attitudes and practices to help reduce the incidence of laboratory-acquired infections. This study was planned to assess the preexisting levels of knowledge, attitudes, and practices of laboratory technicians regarding universal work precautions at a tertiary care hospital in central India and to evaluate the effectiveness of educational interventions on the same.
Method:
The 40 lab technicians participating in the study were subjected to educational interventions in the form of training on universal precautions. Pretest and posttest evaluations using questionnaires were conducted to evaluate the learning gain. Pretest and posttest responses to each question were compared using the Pearson chi-square test. The subjects' mean pretest and posttest scores were compared using paired t tests, and the significance level was set at .05.
Results:
There was remarkably significant improvement in knowledge, attitudes, and practices of laboratory technicians regarding universal work precautions after the educational intervention/training sessions.
Conclusion:
On the basis of the findings, it was suggested that such training sessions should be conducted regularly for laboratory technicians to help in better retention of knowledge and to instill a positive attitude toward universal precautions.
Introduction
Laboratory technicians are routinely exposed to occupational health hazards that could be a serious threat to their health and lives if proper biosafety precautions are not observed. 1 To safeguard themselves against laboratory-acquired infections, laboratory workers must be aware of universal work precautions.
Laboratory technicians working with large pools of clinical specimens are routinely exposed to a large number of potential pathogens. However, they may not be aware of the impending risks and therefore not sufficiently motivated to follow basic universal work precautions. This may result in dangerous laboratory practices during the collection, transport, storage, processing, and disposal of specimens, rendering laboratory technicians more vulnerable and at risk of contracting infections. 2
As per the guidelines of the Center for Disease Control and Prevention (Atlanta, GA), universal work precautions apply to blood; body fluids containing visible blood, semen, vaginal secretions, and body tissues; and fluids such as cerebrospinal, synovial, pleural, peritoneal, pericardial, and amniotic fluids, but they do not apply to feces, nasal secretions, sputum, saliva, sweat, tears, urine, and vomitus, unless they contain visible blood.2–5
Universal work precautions include the use of personal protective equipment (PPE) such as masks, gloves, gowns, aprons, goggles, or protective eyewear, which can reduce the risk of exposing skin or mucous membranes to potentially infectious materials. Because specifying the types of barriers needed for every possible clinical situation is impractical, some judgment must be exercised. Health care workers should also take all necessary precautions to prevent injuries while using needles, scalpels, and other sharp instruments or devices; when handling sharp instruments after procedures; when cleaning used instruments; and when disposing of used needles.3,4
All clinical samples, such as blood and certain body fluids, should be considered potentially infectious. Every laboratory worker should be aware of the potential hazards in his or her workplace and understand the concept of “biosafety,” which promotes safe laboratory practices and procedures as well as the proper use of containment equipment and disposal facilities by laboratory staff. 3
Because adherence to standard guidelines could be affected by a laboratory worker's level of awareness, threat perceptions, attitude/beliefs/opinions, availability of resources, workload, and work culture, laboratory technicians should be equipped with proper knowledge, attitudes, and skills to enable them to follow safe laboratory practices. This study proposed that a targeted educational intervention would not only impart knowledge, increase awareness, and keep laboratory workers updated about universal precautions but would also translate into behavioral changes in attitudes and practices that would help reduce the risk of laboratory-acquired infections.
In their review of 26 studies involving varied populations of health care workers, Safdar and Abad 6 demonstrated a statistically significant decrease in risk, ranging from 0% to 0.79%, in laboratory-associated infection rates after educational intervention.
The educational process should include assessing the factors affecting compliance with biosafety precautions in laboratory technicians, providing a chance to address any gaps in knowledge and practices, and helping to formulate strategies and necessary interventions for minimizing the risk of laboratory-acquired infections.5,7,8 But before being incorporated into institutional policy, the educational strategies should be evaluated for their effectiveness to achieve the desired outcomes.
In view of the above facts, this questionnaire-based interventional study was planned and undertaken to assess the impact of an educational intervention on the knowledge, attitudes, and practices of laboratory technicians regarding universal work precautions at a tertiary care teaching hospital in Central India.
Materials and Methods5,8–10
This interventional study based on self-administered questionnaires was carried out to assess the knowledge, attitudes/perceptions, and practices of laboratory technicians working in the central clinical laboratory of a tertiary care teaching hospital in Central India and to evaluate the effectiveness of educational interventions in eliminating any existing educational and work practice gaps. The study was undertaken after obtaining clearance from the institutional ethics committee at the hospital.
The content, purpose, scope, and nature of the study were very well explained to the study participants, who were told that participation was voluntary and that their responses would be anonymous. Only those who volunteered to participate were included in the study after obtaining verbal consent. To ensure subjects understood the questions, instructors were available to provide explanations.
All of the study participants completed the pretest questionnaire. They then participated in an educational intervention (an induction training program on universal precautions and laboratory biosafety measures) in the form of 2 interactive lectures of 1.5 hours each in 2 separate sessions conducted by the principal investigator. After completion, study participants were administered a posttest questionnaire that was the same as the pretest questionnaire.
The structured questionnaire was designed on the basis of related and relevant literature based on standard guidelines framed by the World Health Organization's Laboratory Biosafety Manual 8 and the Centers for Disease Control and Prevention's Perspectives in Disease Prevention and Health Promotion Update. 6 Questions were checked for their relevance, clarity, and understandability, and requisite changes were made to make them easily understandable. The entire teaching module and the questionnaire were reviewed by senior subject experts to assess the relevance of their contents and were modified accordingly.
The study was conducted in the hospital's Demonstration Hall, where all of the seats are numbered. The questionnaires for the pretest and posttest had numbers corresponding to the seat numbers. The study participants chose their seats randomly. They were distributed the questionnaires with the code number corresponding to their seat number. The questionnaires were anonymous and linked only to the seat number and not to the person seated there. Due care was taken to maintain confidentiality regarding the identity and personal details of the study participants.
The questionnaire consisted of 60 questions divided into 4 parts:
Demographic information (5 questions) Assessment of knowledge (18 questions) Assessment of attitudes/perceptions (12 questions) Assessment of practices (19 questions)
The 18 questions in the knowledge assessment included multiple-choice questions (objective-type questions having only 1 correct response among 4 options), yes/no type items, and enumerative questions.
For the 12 questions in the attitudes/perceptions assessment, the respondents gave their opinions on a 1- to 5-point Likert scale ranging from strongly agree to strongly disagree.
For the 19 questions in the assessment of practices, the respondents gave their opinion on a 1- to 5-point Likert scale ranging from never to always.
Assessment of the knowledge, attitudes/perceptions, and practices components was done on the basis of a scoring system in which 1 point was given for each correct response to knowledge, positive attitudes/perceptions, and correct practices and 0 was given for incorrect knowledge, negative attitudes/perceptions, and suboptimal/risky practices. A score of 75% or greater was considered good, 50% to 74% as moderate, and less than 50% as poor.
Statistical Analysis
The responses to the questionnaire from the voluntary participants were tabulated, and data were compiled using Microsoft Excel 2010 software. Appropriate statistical tools were used as per requirement. P values for the chi-squared distribution (for various values of χ 2 and degrees of freedom) were calculated for pretest and posttest responses to each question by using the Pearson chi-square test. Subjects' pretest and posttest scores were compared using paired t tests, and the significance level was set to P < .05.
To study the effectiveness of the educational intervention, the authors calculated absolute learning gain and class average normalized gain as follows:
Absolute learning gain: (posttest) – (pretest)
Class average normalized gain (g) was calculated by Hake's criteria:
 where brackets indicate class averages/mean test scores. Class average normalized gain is categorized as follows: 0.1 to 0.29 as low gain, 0.3 to 0.69 as medium gain, and 0.7 to 1.0 as high gain.
where brackets indicate class averages/mean test scores. Class average normalized gain is categorized as follows: 0.1 to 0.29 as low gain, 0.3 to 0.69 as medium gain, and 0.7 to 1.0 as high gain.
Results
Knowledge of Universal Work Precautions
The assessment of knowledge regarding universal work precautions among laboratory technicians through pretest and posttest questionnaires, with the same set of questions administered before and after the educational intervention, clearly reveals a highly significant improvement in knowledge levels after the training session (P < .00001).
Before training, most of the study subjects (60%) showed poor levels of knowledge, 25% exhibited moderate levels, while only 15% were found to have good levels of knowledge (Figure 1). After training, 45% of trainees showed good levels of knowledge, 32.5% exhibited moderate levels, and only 22.5% were left with poor knowledge levels (Figure 1).
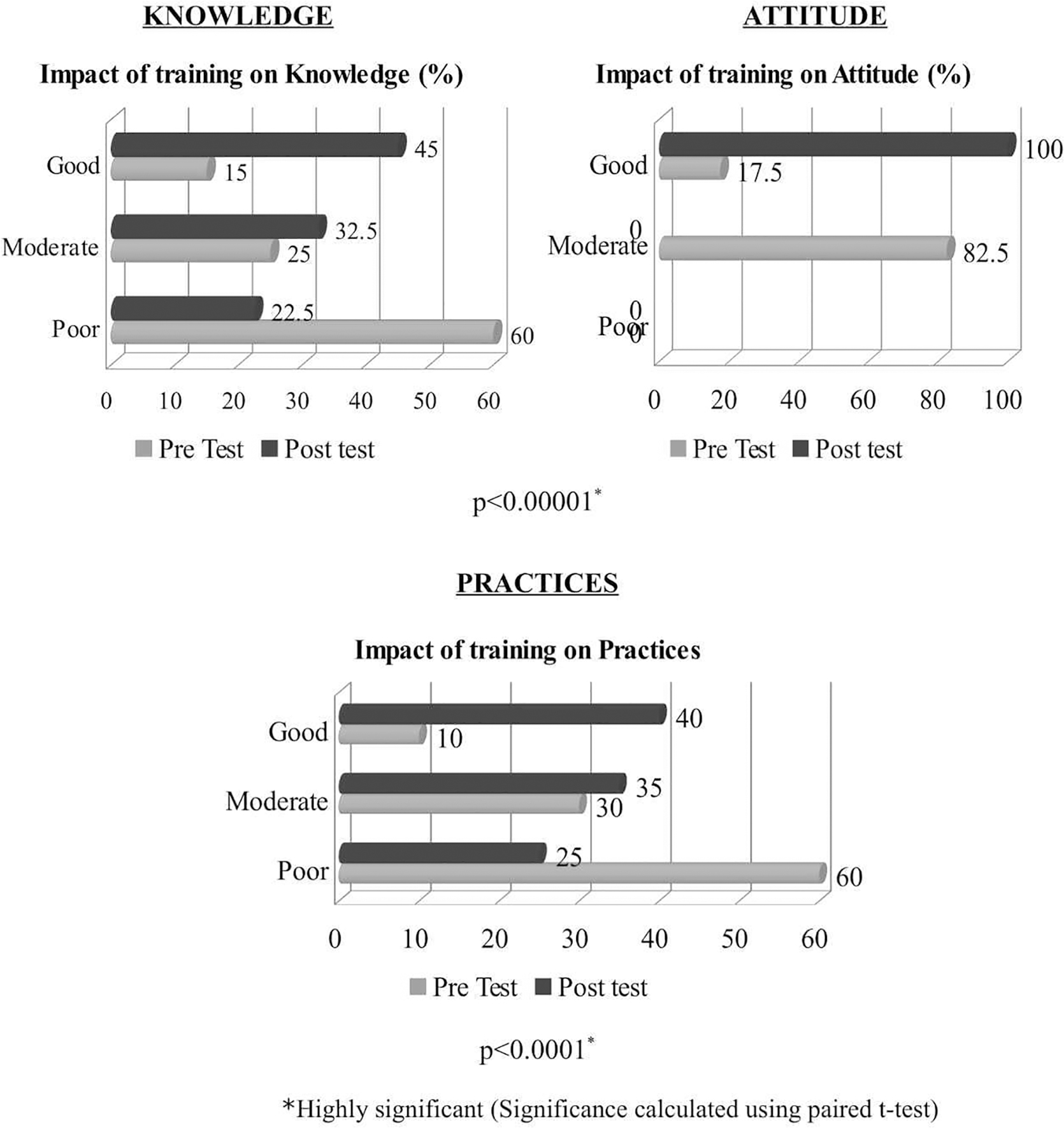
Assessment of impact of training on knowledge, attitudes, and practices regarding universal work precautions among laboratory technicians.
Of 18 questions asked, a significant difference was observed in pretest and posttest responses to 14 questions, indicating a remarkable improvement in the knowledge levels of participants after training (Table 1).
Significance was calculated using Pearson chi-square test. NS indicates P > .05 (not significant).
P < .05 (significant); **P < .001 (highly significant).
Attitudes Regarding Universal Work Precautions
The assessment of attitudes in this study clearly showed the study subjects' improvement in attitude levels after training. This was statistically significant (P < .0001).
Before training, most of the study subjects (82.5%) exhibited moderate levels of attitude, while 17.5% demonstrated good attitude and none showed poor attitude. After training, all trainees (100%) were found to exhibit good attitude levels regarding universal work precautions (Figure 1).
Of the 12 questions that assessed attitude, a significant improvement in attitude levels between pretest and posttest responses was seen in 4 questions (Table 2).
Significance was calculated using Pearson chi-square test. NS indicates P > .05 (not significant).
P < .05 (significant); ** P < .001 (highly significant).
Practices Regarding Universal Work Precautions
The assessment of practices in this study clearly indicates that the study subjects' improvement in practice levels after training was statistically significant (P < .0001).
Before training, most of the study subjects (60%) exhibited poor levels of practice, 30% showed moderate levels, and only 10% showed good levels of practice. After training, 40% of the study subjects were found to exhibit good levels of practice, 35% showed moderate levels, and only 25% showed poor levels of practice (Figure 1).
Of 20 questions assessing practices, a significant difference in practice levels between pretest and posttest responses was seen in 14 questions (Table 3).
Significance was calculated using Pearson chi-square test. NS indicates P > .05 (not significant).
P < .05 (significant).
As depicted in Table 4, significantly high absolute learning gain in all 3 sections occurred. Hake's class average normalized gain metrics clearly indicated a medium learning gain for all sections. However, learning gain for the knowledge and practice sections was similar and comparatively higher than for the attitude section.
Significance was calculated using paired t test.
P < .001 (significant); **P < .0001 (highly significant).
Discussion
In this study, it was observed that more than 70% of study subjects (lab technicians) exhibited poor levels of knowledge prior to the training program. This finding is similar to a number of studies conducted in the past. Zaveri and Karia 2 reported that the level of awareness about universal work precautions was as low as 20.8%, wherein most of the subjects had not even heard the term. Attitude and practice levels were also low, as demonstrated in the studies conducted by Omokhodion, 11 Alam, 12 Odusanya 13 Ejilemele and Ojule, 14 Suchitra et al, 15 and El Gilany et al. 1 These findings are in contrast to the studies conducted by Goswami et al 16 and Gurubacharya et al, 17 who reported good levels of knowledge, attitude, and practice regarding universal work precautions by the paramedical staff.
In our study, of the 18 questions asked to assess the knowledge levels of study subjects, a significant increase in the number of correct responses to 14 questions occurred after the educational intervention. However, there was no significant effect from training on the questions pertaining to barrier precautions, PPE, liquid waste disinfection, and method of discarding blood samples. In these cases, there was no remarkable difference in the number of correct responses to these questions between the pretest and posttest. This lack of statistical improvement was due to an already high level of knowledge in these areas during the pretest; that is, there was less room for improvement, except for PPE, for which the level of awareness remained low even after the intervention.
As evident from the results of this study, there was remarkably significant improvement in the knowledge, attitudes, and practice of laboratory technicians regarding universal work precautions after the educational intervention/training sessions. This finding is in accordance with a number of similar studies conducted previously (Suchitra et al, 15 Goswami et al, 16 Malgaonkar and Kartikeyan, 18 El-Gilany et al, 1 and Gaikwad et al.6,7 The study by El-Gilany et al 1 had stressed the importance of repeated training sessions at regular intervals to reinforce safe laboratory practices.
In our study, 65% of lab technicians reportedly practiced recapping of needles routinely; this is a risky practice, and because of the impending risk of needle-stick injuries, it is not at all recommended according to the standard guidelines in Biosafety in Microbiological and Biological Laboratories. 19 This finding is in accordance with the study conducted by Nasim et al, 20 in which about 50% of lab technicians were reported to use this risky practice. But after the training program, most of the technicians in our laboratory were found to discontinue this practice.
In a study conducted by Kamal and Khan, 21 it was observed that the practice of reusing disposable syringes is as high as 24%, and most of the health care providers were unaware of the health hazards associated with this suboptimal practice. To curb this practice, used syringes must be discarded properly. However, Nasim et al 20 in a similar study showed that 43% of the study subjects from the public sector threw used syringes into the dustbins without using proper disposal methods. In addition, Habibullah and Afsar 22 reported that only 35% of health care facilities cut needles before disposal.
Centrifuge machines are one of the main sources of aerosol dispersal in laboratories. If these aerosols are inhaled, the result could be a laboratory-acquired infection. Therefore, according to the US Department of Health and Human Services, the Centers for Disease Control and Prevention, and the National Institutes of Health, prior to centrifuging, the tubes should be capped and centrifuges should be closed to avoid biohazards due to inhalation. 18
In a study conducted by Nasim et al, 20 34% of lab technicians never or only occasionally closed centrifuge machines during centrifugation, while in another study by Misra et al, 23 this figure was much higher (ie, 63%). In our study, more than 65% of respondents were found to follow the correct practice of closing the centrifuge prior to operation, which was further improved to 87.5% after training.
In a study conducted by Suchitra et al, 15 a significant difference in the preeducation and the first posteducation responses was observed. However, the performance of respondents declined in the second posttest and dropped further in the third posttest. A similar problem with the retention of knowledge with the passage of time was observed in a study by Wagner et al. 24
Therefore, it was suggested that training sessions needed to be conducted at regular intervals for various categories of health care workers to improve retention of knowledge and to instill a positive attitude toward universal work precautions through repetitive reinforcement. This would also translate into behavioral changes in attitudes and practices that would help to reduce the incidence of laboratory- and hospital-acquired infections. In addition, written standard institutional guidelines and well-structured training modules for health care workers including lab technicians should be in place.
While evaluating the effectiveness of educational intervention in this study, we have found a statistically significant absolute learning gain and a medium level of class average normalized learning gain for all 3 aspects: knowledge, attitude, and practices. These findings support the effectiveness of the induction program. However, there is definitely a scope for further improvement in the training program, so as to achieve higher levels of learning gain.
To address the issues of persistently poor levels of knowledge and practice, even after the educational intervention evident from the posttest scores in some of the study participants, the authors will redesign the training modules in consultation with subject experts to achieve a more targeted and personalized approach. Such redesigned interventions for the lab technicians would be conducted at regular intervals, particularly targeting the poor performers.
An important limitation of this study was the use of self-administered questionnaires to assess the levels of practice among the respondents. Although self-reporting may be the simplest, easiest, and least time-consuming method, there is always a risk of bias on the part of the respondents who will tend to report better practices than what they actually do.
Declared practices may or may not reflect actual practices: only direct observation can confirm improvement of actual practices. Therefore, further studies are suggested involving checklist-based onsite assessment through direct observation to analyze the impact of educational interventions on the actual practices of the study subjects.
A targeted educational intervention strategy can be helpful in the long-term reduction of laboratory-acquired infections. Safdar and Abad 6 reviewed 26 studies involving varied study populations of health care workers using a number of different educational programs and demonstrated a statistically significant decrease in infection rates after intervention in 21 studies.
But such positive outcomes in laboratory practice may not be solely attributable to knowledge gain from a 1-day educational intervention. Multiple factors determine compliance with universal work precautions/safe laboratory practices. These may include lack of knowledge, experience, and skills; lack of proper training; lack of institutional guidelines; high work load; understaffing; lack of motivation/encouragement; lack of role models; lack of resources; lack of administrative support; poor work culture; lack of incentives; staff risk perceptions; time pressures; and facilities available for staff to use. Hence, it is recommended that further studies be planned to include these factors to assess sustained improvement in adherence to safe laboratory practices by laboratory workers.
Footnotes
Ethical Approval Statement
This study was conducted with prior approval from the Institutional Ethics Committee, Govt. Medical College, Datia. The work presented here is original and has not been submitted or published elsewhere.
Statement of Human and Animal Rights
Not applicable to this study.
Statement of Informed Consent
Informed consent has been taken from all participants.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.