
Abstract
Introduction:
Biosafety Level 2 (BSL-2) training programs were benchmarked at institutions of higher learning in the United States by surveying Biosafety Officers (BSOs). The goal of this survey was to not only compare Institutional Biosafety Committee (IBC) requirements for BSL-2 training but also compare delivery format, length of training, inclusion of a hands-on or interactive component, and requirement for refresher training.
Methods:
Survey subjects were drawn from the National Institutes of Health (NIH) registry of BSOs and were limited to BSOs at institutions of higher learning in the United States. Twelve survey questions were developed in this study. The survey was sent to 324 BSOs, of which 108 responded with sufficient data to be included in the analysis.
Results:
The survey found that BSL-2 training is required by the institutional and/or IBC policy at 88% of institutions, is optional at 5.6%, and not offered at 6.5%. More than half of the respondents (60.4%) offered BSL-2 training in an on-demand manner. Some institutions (34.5%) include a component of training that is in person. However, this training does not always include hands-on exercises or interactive activities. The survey indicated that most (96.6%) institutions offered BSL-2 training less than three hours in length, and many (58%) institutions required refresher training.
Conclusions:
Most institutions of higher learning in the United States, which are registered with the NIH, require BSL-2 training for laboratory personnel involved in research and teaching.
Introduction
Laboratory personnel working with biological materials should receive appropriate training to perform their work safely and ensure compliance with biological safety regulations and guidelines. Biosafety Level 2 (BSL-2) training covers the basic principles and practices for working with biohazardous materials, including infectious agents that cause human disease, microbial toxins, and other hazardous biological materials that pose a moderate risk to personnel and the environment, as outlined in the
There is no regulatory requirement for institutions to provide BSL-2 training. 1 This is different from the training requirements for work with other hazards, including work with chemical hazards as mandated by the Hazard Communication Standard, 4 work with materials that may contain microorganisms infectious to humans present in blood as mandated by the Bloodborne Pathogen Standard, 5 and work with biological agents and toxins that pose a severe threat to human, animal, and/or plant health as mandated by the Select Agent and Toxins regulations 6 Although many institutions offer BSL-2 training, the individual principal investigator (PI) who leads the research is responsible for training their personnel and students on how to work safely with biohazardous materials at BSL-2 instead of the institution.
Biosafety training helps ensure that laboratory personnel know how to work safely with biohazardous materials. Higher education institutions may have personnel who lack experience working with the unique hazards found in a biological laboratory. Lack of hazard awareness and inadequate safety knowledge have led to unsafe actions, 7 leading to over 90% of safety incidents in biology laboratories. 8 When hazards are unrecognized or underestimated, risk perception is influenced, which has been shown to impact safety-related decision-making. 9 Familiarity with biosafety training and knowledge of agents studied have correlated with reduced laboratory-acquired infections. 10 BSL-2 training offered at an institutional level promotes a foundation of knowledge of laboratory hazards and safety work practices for working with human pathogens or other biohazardous materials. As an institution, we have completed a high-level risk assessment based on the Institutional Biosafety Committee protocols submitted, the Iowa State University (ISU) policies, and the types of facilities and equipment we have. Based on this risk assessment, we developed a general BSL-2 training that can be used as an introductory overview of what researchers may expect. It is the responsibility of the individual PIs and/or supervisors to provide laboratory-specific training based on the hazards and risks in their respective workspaces. Laboratory-specific training must be provided by competent laboratory staff to ensure proficiency in handling biohazardous materials and safely performing associated procedures.
As outlined in published biosafety guidelines from the Centers for Disease Control and Prevention1,2 and NIH Guidelines,
3
content covered as part of BSL-2 training builds upon the basics of working with noninfectious biohazardous materials. Based on these guidelines, BSL-2 training programs include topics such as identifying potential hazards, hazard control measures, administrative control measures, and emergency preparedness and response. This training should consist of the essential elements of BSL-2 criteria outlined by the
ISU offers BSL-2 training to students, staff, and faculty working with biohazardous materials that require BSL-2. This training is not required by institutional policy or the Institutional Biosafety Committee (IBC). Historically, the training consisted of an in-person classroom presentation covering the principles of biosafety, the procedures and practices necessary to work safely with biohazardous materials, and a hands-on component that included identification of improperly prepared biohazardous waste and utilizing provided resources to determine the proper disinfectant for a given infectious agent. The course was offered several times a year and open to a maximum of 20 participants (i.e., faculty, staff, students, and postdocs).
The authors discussed implementing an online on-demand BSL-2 course, as low enrollment in the in-person course has resulted in numerous cancelations of the offered sessions (i.e., a minimum of six participants are required for training to occur). There is perceived value for in-person BSL-2 training, which may be lost by providing training in an online format. It is presumed that enrollment in the in-person course would be much higher if there were a requirement to take this course at the institutional level or by the IBC. However, a requirement for BSL-2 training may increase enrollment to a level in which additional course sessions would be necessary, requiring extra support by biosafety professionals.
The discussions regarding transitioning from in-person to online training included benchmarking the training format and the requirement for training at other academic institutions. A previous survey of biosafety professionals found that 85% of the institutions required biosafety training at BSL-2. 11 However, this publication did not differentiate this training requirement for academic institutions from other institutions, including private companies, government agencies, and nonprofit organizations. 11 In addition to the delivery format and requirement for BSL-2 training, the length of training, the inclusion of a hands-on component, and available refresher BSL-2 training were crucial areas of focus. A survey was created and distributed to biosafety professionals at other academic institutions of higher education to benchmark other BSL-2 training programs.
Materials and Methods
The cohort for this study was chosen from a list of IBC contacts and Biosafety Officers (BSOs) of record at the NIH. A Freedom of Information Act request was filed with the NIH in October 2022 to list all BSOs and IBC contacts, including email addresses. The original list from the NIH included IBC contacts and BSOs from educational institutions (i.e., emails ending .edu), commercial entity BSOs (e.g., emails ending .com or .org), and international institutions (e.g., email addresses ending .uk, .au, .ca, etc.). The list also included duplicate entries for BSOs whose responsibilities included multiple departments, sections, or institutes within a larger organization and various contacts for a single institution or IBC. Duplicate and multiple contact email addresses (313), such as email addresses ending .com (530), .org (171), .gov (66), .mil (6), .bio (2), .us (2), .inf (1), and international email addresses (81), were excluded from the survey cohort. From an original list of 1519 IBC contacts and BSOs, this resulted in a survey sample size of 324 BSOs and IBC contacts, who were emailed invitations to the survey.
The survey consisted of 10 multiple-choice questions and two free-text entry questions. It was determined through preview testing (unpublished data) that the average length of time it would take a respondent to complete the survey was 10 min. The survey queried training format, length, and frequency of training, but did not delve into the specific knowledge included in the training. In addition, the survey did not include a definition of BSL-2 training because the
The survey and prospective respondents’ information was submitted to the ISU Institutional Review Board (IRB). The IRB determined that approval for this survey was not required because it does not include human subjects (as they are federally defined). The survey was sent to the final list of email addresses using Qualtrics®, and a reminder email was subsequently sent to the BSOs that had not participated initially.
Pearson’s chi-squared test using two degrees of freedom was performed to analyze if there was a correlation between select survey responses using R software (https://www.r-project.org/). A
Results
Survey Response
Of the original 324 NIH-registered BSOs, 111 responded, representing a 34.3% response rate. Since three did not respond to all survey questions (≤2 responses), 108 respondents’ answers were used for the analysis. The geographic distribution of the respondents was limited to the United States of America (USA) and represented all regions of the United States.
Requirement for BSL-2 Training
Respondents indicated that BSL-2 training was required by their institution, 83.3% (
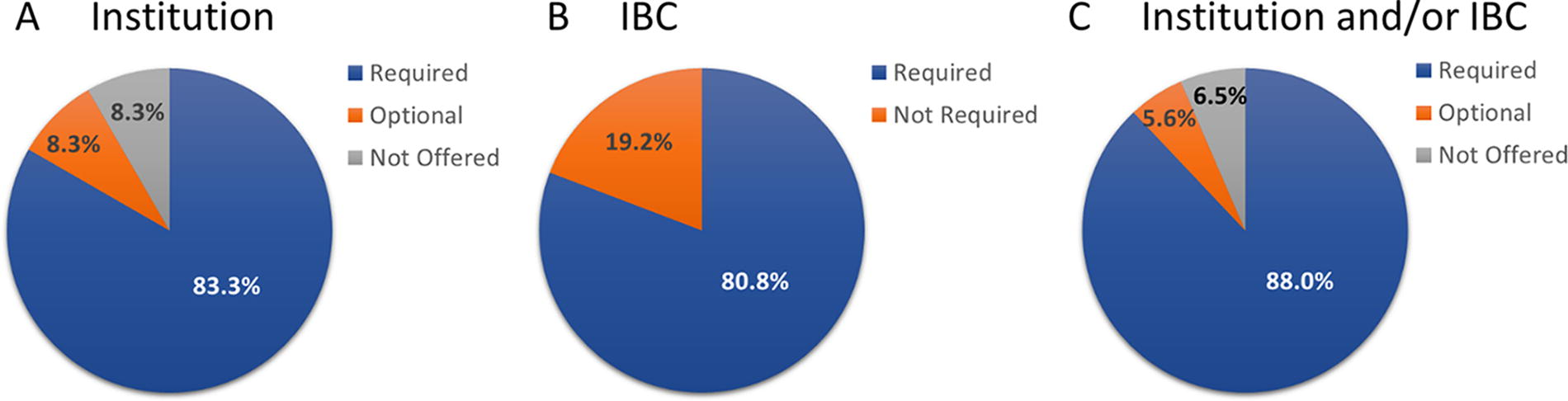
Requirement for BSL-2 training. (A) Requirement for training at the institutional level. (B) Requirement for training by the IBC. (C) Requirement for training by the institution and/or IBC. BSL-2, Biosafety Level 2; IBC, Institutional Biosafety Committee.
Based on Carnegie Classification’s definitions for institution size, 12 respondents to this survey were fairly evenly distributed between small (20%), medium (19%), large (27%), and huge (34%) institutions based on student enrollment.
All respondents from medium institutions (
Format of BSL-2 Training
The next set of survey questions related to the format or delivery method of the training was only offered to respondents who indicated BSL-2 training was provided. The majority of respondents (60.4%,
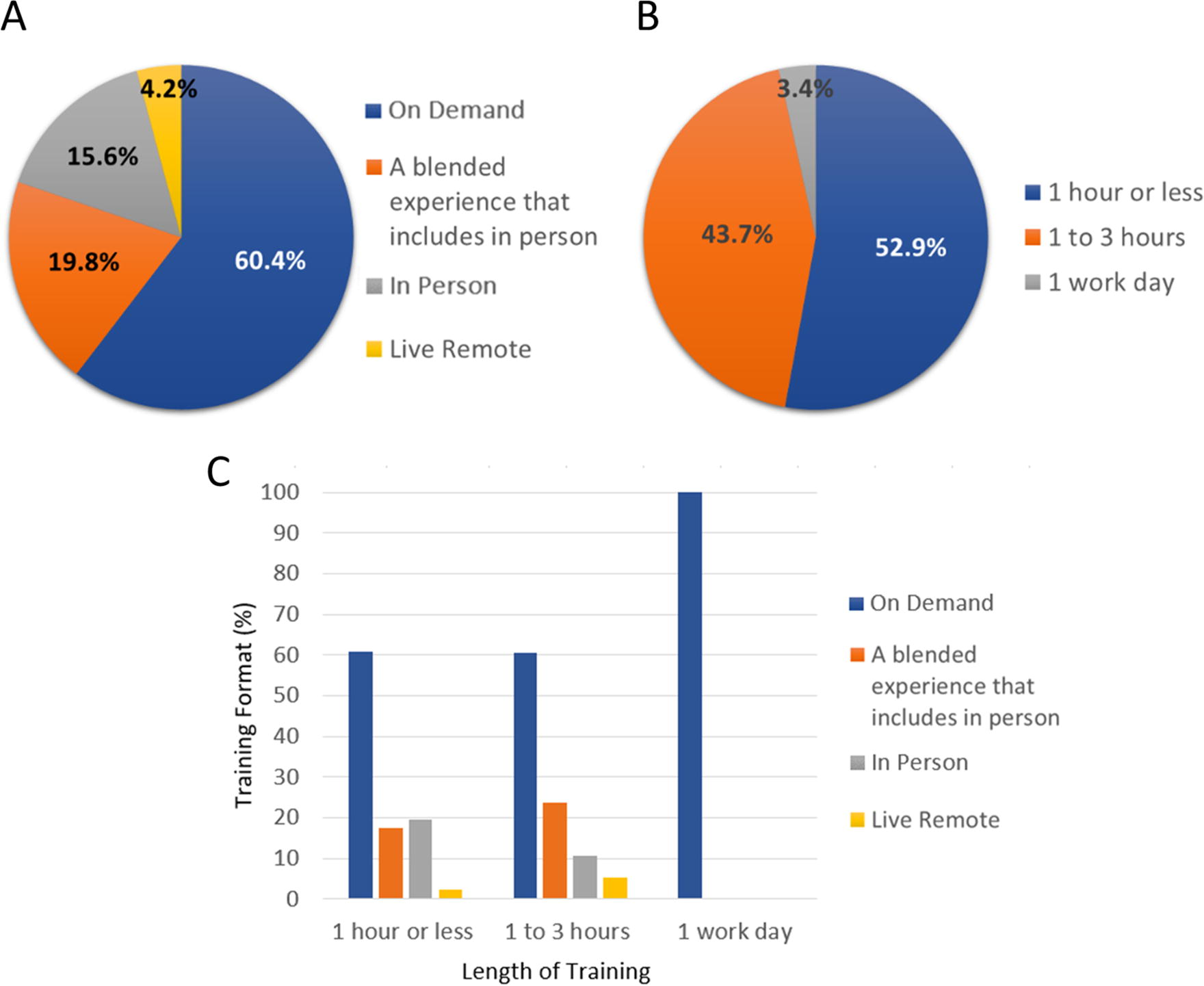
Format and length of BSL-2 training. (A) Delivery format of BSL-2 training. (B) Length of BSL-2 training. (C) Relationship between delivery format and length of training.
For respondents who indicated training was required, the most utilized delivery format was on-demand, 61.5% (
When there was no training requirement, the most utilized delivery format was split between on-demand, 40% (
On-demand training is the most popular training format regardless of institution size based on survey responses provided by 75 respondents, accounting for 50% (
Length of BSL-2 Training and Relationship to Delivery Format
When asked about the length of BSL-2 training offered, more than half of the respondents, 52.9% (
There was no significant difference in BSL-2 training formats when the training was offered for ≤1 h or 1–3 h. Aggregating the format and length of training, respondents stated that on-demand format for 1 hour or less and 1–3 h was the most common combination. On-demand training was offered by 100% (
Hands-on Component Included in BSL-2 Training
BSOs who indicated that the BSL-2 training format was either in-person or a blended experience, including in-person, were asked to categorize the type(s) of hands-on exercises or interactive activities included in the BSL-2 training. A total of 30 respondents answered this question, of which 11 said the training was offered in-person, and 19 said the training was a blended experience, including in-person. Of these, 4 and 8 respondents, respectively, or 40% total (
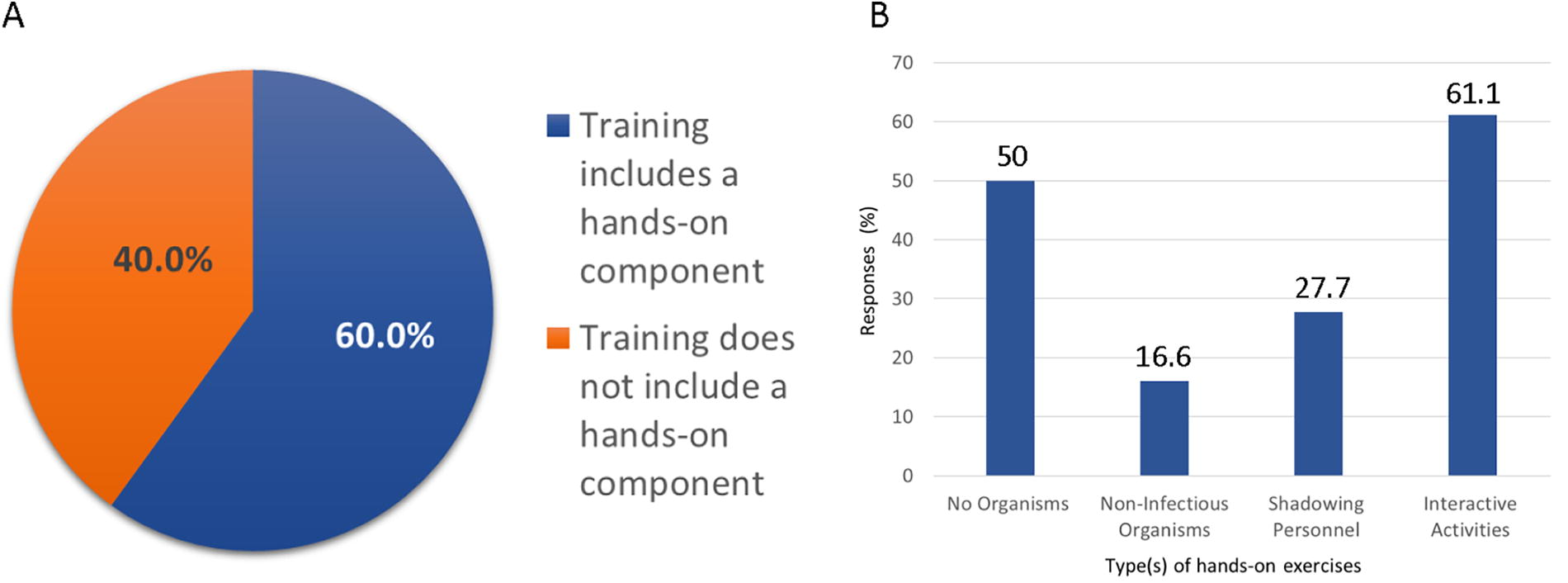
Type(s) of hands-on exercises or interactive activities that were reported by respondents who said that their BSL-2 training format was either in person or a blended experience that includes in-person training. (A) Responses regarding the inclusion of a hands-on component in training. (B) Responses regarding type(s) of hands-on exercises.
Of the 18 respondents who identified that a hands-on component was included as part of the training, 50% (
Respondents who selected at least one type of hands-on exercise or interactive activity were asked to describe the hands-on exercises or interactive activities included in the training. Of applicable respondents, 61% (
Descriptions of hands-on exercises or interactive activities
PI, principal investigator; BSC, biosafety cabinet; PPE, personal protective equipment; BSL, biosafety level.
Refresher BSL-2 Training
Many respondents, 58% (
Format of Refresher BSL-2 Training
The majority of respondents, 78.9% (
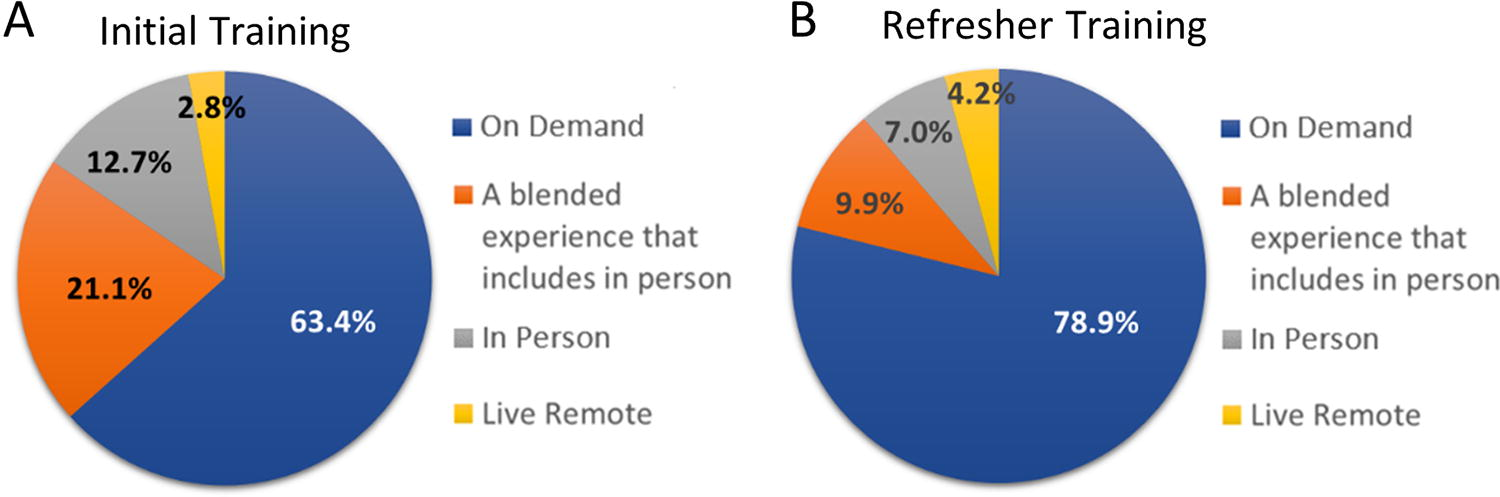
Training format for respondents who said that their institution offers both initial and refresher BSL-2 training. (A) Initial BSL-2 training. (B) Refresher BSL-2 training.
Length of Refresher BSL-2 Training
When asked about the length of refresher BSL-2 training, over half of the respondents, 60.6% (
Respondents who indicated their institutions did not currently offer BSL-2 training were asked whether there was a plan to develop BSL-2 training in the future. About half of the 44.4% (
Discussion
This survey found that most institutions of higher learning in the United States, which are registered with the NIH, require BSL-2 training either as a policy of the Institution and/or IBC, although it is not specifically required by the NIH Guidelines
3
or
The survey found that 61.5% of institutions that require training offer this training on-demand. A portion of the respondents indicated that training is provided through a blended experience that includes in-person (19.7%), which may have an on-demand training component. Therefore, an on-demand format may be offered at up to 81% of institutions requiring BSL-2 training, although this could not be confirmed using the survey data acquired. This result is consistent with the increased prevalence of online training, which has become the fastest-growing market in the education industry, with a 900% growth rate globally since the year 2000. 15 The COVID-19 pandemic further contributed to the utilization of this teaching format as a majority of higher education institutions developed online curriculums to fulfill traditional in-person lectures such as laboratory, field, and studio components. 16 Although several credentialing organizations, such as ABSA International, allowed for an extension of the certification period due to the COVID-19 pandemic, 17 other professions moved their continuing education and refreshers to asynchronous online training.
The survey found that BSL-2 refresher training is required at most institutions, even though this is not a requirement outlined by published biosafety guidelines1–3 or specific occupational safety regulations. 13 Recurrent training aligns with several public health regulations, which require annual refresher training for individuals who work with bloodborne pathogens 5 and select agents and toxins. 6 Many professions require continuous educational training to provide awareness, introduce new techniques, and reinforce skills and knowledge that may have been forgotten.18–20
Only a small contingent of respondents (<10%) indicated that a hands-on training component was included, regardless of delivery format. Online training formats offer a convenient and cost-effective method for training delivery as individuals can take the training on-demand. A study that investigated the use of virtual simulations for laboratory exercises showed that students trained either virtually or through live demonstration tutor showed similar knowledge in the microbiological practice of streaking plates. 21 A study on the effectiveness of online cardiopulmonary resuscitation recertification training versus in-person training found online training was as effective or better than in-person recertification training and produced better learning outcomes when the training has user-controlled interactions and prompts for learner reflection.22,23 It is important to note these studies were on recurrent training and did not study the effectiveness of presenting initial training in an online format.
Online learning offers the ability to incorporate features that appeal to multiple learning styles. For example, some learners prefer reading text to comprehend information, whereas audio learners benefit most from listening to information, and visual learners benefit from images and animations. 24 Online training also offers the opportunity to employ learner engagement strategies, such as games and other interactive features. 25 Training modules can be purposefully abbreviated to reflect the students’ attention span to learn new material while allowing the learner to review the material in the course at any time. 26
Limitations
The survey’s focus was to benchmark the BSL-2 training programs offered by other academic institutions of higher education, which included the requirement for training, delivery method, length of training, and if the training included a hands-on component. There are several areas of focus that this survey did not inquire about. For example, this survey did not evaluate which personnel at the institution the BSL-2 training was provided to (students, faculty, or staff). The survey did not capture the BSL-2 training programs at nonacademic institutions such as private companies, government agencies, or nonprofit organizations. All responses were from individuals at institutions of higher learning listed on the NIH registry of BSOs; however, no additional characteristics, such as job role or specific institution type, were captured as part of the survey, As the content of BSL-2 training is covered in biosafety guidance publications, the content of training offered at academic institutions was not included as part of the survey inquiry. Word selection, the format, or presentation style of the provided training were not included, nor was an evaluation of the delivery method concerning learning engagement and information retention. The survey did not inquire about compliance or effectiveness of institutions’ training programs, which may be impacted by aspects of the training program, such as delivery method. In addition, this survey was not utilized to compare the BSL-2 training programs found in different geographic regions or used by other cultures.
The survey question regarding the types of hands-on exercises or interactive activities included in the training elicited many responses, referencing laboratory-provided training (Table 1). It was determined that this question could have been written more clearly to capture only responses related to hands-on training provided directly by the institution. However, only 18 of 108 respondents indicated that hands-on training was included as part of their BSL-2 training program, so it is indicated that few institutions include hands-on training or interactive activities as part of the offered BSL-2 training. Furthermore, the survey did not include a question regarding hands-on or interactive training for work at ABSL-2.
Conclusions
A survey of BSOs was used to benchmark BSL-2 training programs offered by institutions of higher learning in the United States. Based on survey responses, most institutions that conduct research or teach at BSL-2 require laboratory personnel to complete BSL-2 training. Most respondents also indicated the requirement was the policy of both the IBC and the institution. The format or delivery method used to provide the BSL-2 training was predominantly provided using an on-demand format, with a small contingent of respondents (<10%) indicating a hands-on training component was included, regardless of delivery format. Most institutions offer BSL-2 training that is less than three hours long. Most institutions that indicated they require BSL-2 training for personnel also provide refresher BSL-2 training, with on-demand being the predominant format. The results of this survey can serve as an opportunity for institutions to benchmark their BSL-2 training programs and provides evidence that most institutions have a mandatory BSL-2 training requirement as part of their IBC requirements.
Footnotes
Acknowledgments
The authors would like to thank the Iowa State University Center for Survey Statistics and Methodology (ISU CSSM), which was consulted to help formulate questions. The authors would also like to thank the Iowa State University Statistical Consulting Group, which performed the statistical analyses for this article.
Authors’ Contributions
K.H. and S.Z. contributed to the design and implementation of the research, K.H. contributed to the analysis of results, and all authors contributed to the writing of the article. B.M. conceived the original concept and supervised the project.
Data Access Statement
Research data supporting this publication are available from the corresponding author.
Authors’ Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.