
Abstract
A recent series of widespread infectious disease outbreaks has highlighted commonalities and differences between three key professions that operate on the front lines of response in support of research and/or direct healthcare providers: biosafety, infection prevention, and public health. This assessment, which builds upon previous study by the authors, examines the stated professional competency categories for these three areas, highlighting similarities and differences. This assessment is important as these professions are being drawn together in an operational environment driven by the current pandemic and inevitably future disease outbreaks. Cross-training opportunities for the various professions are proposed.
Introduction
After Ebola virus disease (EVD) was detected in the United States in 2014, we performed a comparison of the similarities and differences of the stated competency categories for the biosafety and infection prevention professions. 1 The intent of the exercise was to identify possible training needs that could be facilitated by these two key professional organizations, ABSA International (ABSA) and the Association for Professionals in Infection Control and Epidemiology (APIC), to bridge the gap between protecting laboratorians (the primary focus of biosafety professionals) and protecting patients and healthcare workers (the primary focus of infection prevention professionals), respectively.
Fortunately, the EVD spread within the United States was aggressively contained and relatively brief. This outcome, however, is in stark contrast to the current coronavirus disease 2019 (COVID-19) pandemic where biosafety and infection prevention professionals are routinely interacting among each other as well as with public health professionals, whose primary focus is the health of the general public. To this end, in this article we update our original 2016 publication by performing an assessment of the stated competencies for public health professionals, as described by the National Board of Public Health Examiners for the Certificate in Public Health (CPH) credential, and compare them with the competencies of the biosafety and infection prevention professions.
The primary credential for infection preventionists is the Certification in Infection Prevention and Control (CIC). Credentials for biosafety professionals include the Certified Biological Safety Professional (CBSP) or the Registered Biosafety Professional (RBP). The purpose of this update is to identify commonalties and differences among these professions and, more importantly, to promote understanding, cross-training, and collaboration among all three of these groups. We feel this is crucial, not only to address the current pandemic, but for the successful management and mitigation of future outbreaks.
Methods
A thoughtful collection of dedicated professionals from the biosafety, infection prevention, and public health professions convened over time to elucidate the basic competencies that a practicing professional, in one of these areas, should possess. To be recognized as a professional in their realm, competency acquisition is proven through documented academic and professional knowledge, professional experience, an examination, and subsequent continuing education. Each professional organization (ABSA, APIC, and APHA) has established requirements for qualification, certification, and maintenance of their respective professional credentials. Competency requirements for each of these three areas were reviewed and compared by the authors during this analysis.2–5
Table 1 summarizes the sources from where we obtained the stated competencies. Since the previous assessment, the competences for the CIC were updated in 2021 and these updates have been incorporated into the current assessment.
Summary of biosafety, infection prevention, and public health professional organizations and associated certifications from which competencies are drawn
Competencies are drawn from published certification requirements.
The previous assessment included a detailed list of the stated competences for the biosafety and infection prevention realms. 1 An important lesson learned from this previous assessment was that the stated competences for the biosafety and infection prevention professions varied by degree of granularity, leading to the need for the authors to apply professional judgment to consolidate the competency statements into topical and manageable areas.
For example, subtle differences were noted in the processes and objectives for elements such as disinfection and decontamination, use of protective equipment, and waste management. Those wishing to obtain more detailed information on the specific stated competencies for each profession are encouraged to access the respective websites listed in the references section of this article.
Results
Within the stated competencies, all three professions require a basic understanding of human disease history, transmission, and preventive measures. This knowledge is used to protect the health of their respective target populations—laboratory workers, patients and healthcare workers, and the general population—as well as educate and train these populations regarding safe and healthy practices. All three professions require the development, management, and implementation of programs that must align with applicable regulations, guidelines, and accepted standards of practice. Communication is a common competency as each profession is required to effectively train and convey their program goals to have a substantial impact on their populations' perceptions and behaviors, which ultimately impacts outcomes.
Public Health and Infection Prevention commonly collect and evaluate data on disease surveillance and use epidemiological statistical methods to study disease correlation and prevention initiatives.
Although not explicitly stated in the listed professional competencies, biosafety commonly intersects with public health. For example, within human research/clinical studies (e.g. biosafety participation and input within the Institutional Review Board), leadership and management (e.g. biosafety serving as representatives within the Institutional Biosafety Committee, Institutional Review Board, and/or Institutional Animal Care and Use Committee), and within protocol development, guidance or training for public health (e.g. training for clinicians during Ebola virus outbreak including patient transport issues, COVID-19 related protocol development for diagnostic testing, vaccination sites, employee and student training, personal protective equipment selection and training, etc.).
Figure 1 graphically displays an annotated summary of the stated competencies categories for biosafety, infection prevention, and public health professionals as stated by ABSA, APIC, and APHA, with overlapping competencies as identified by the authors in the center and competency categories primarily applicable to each profession around the perimeter.
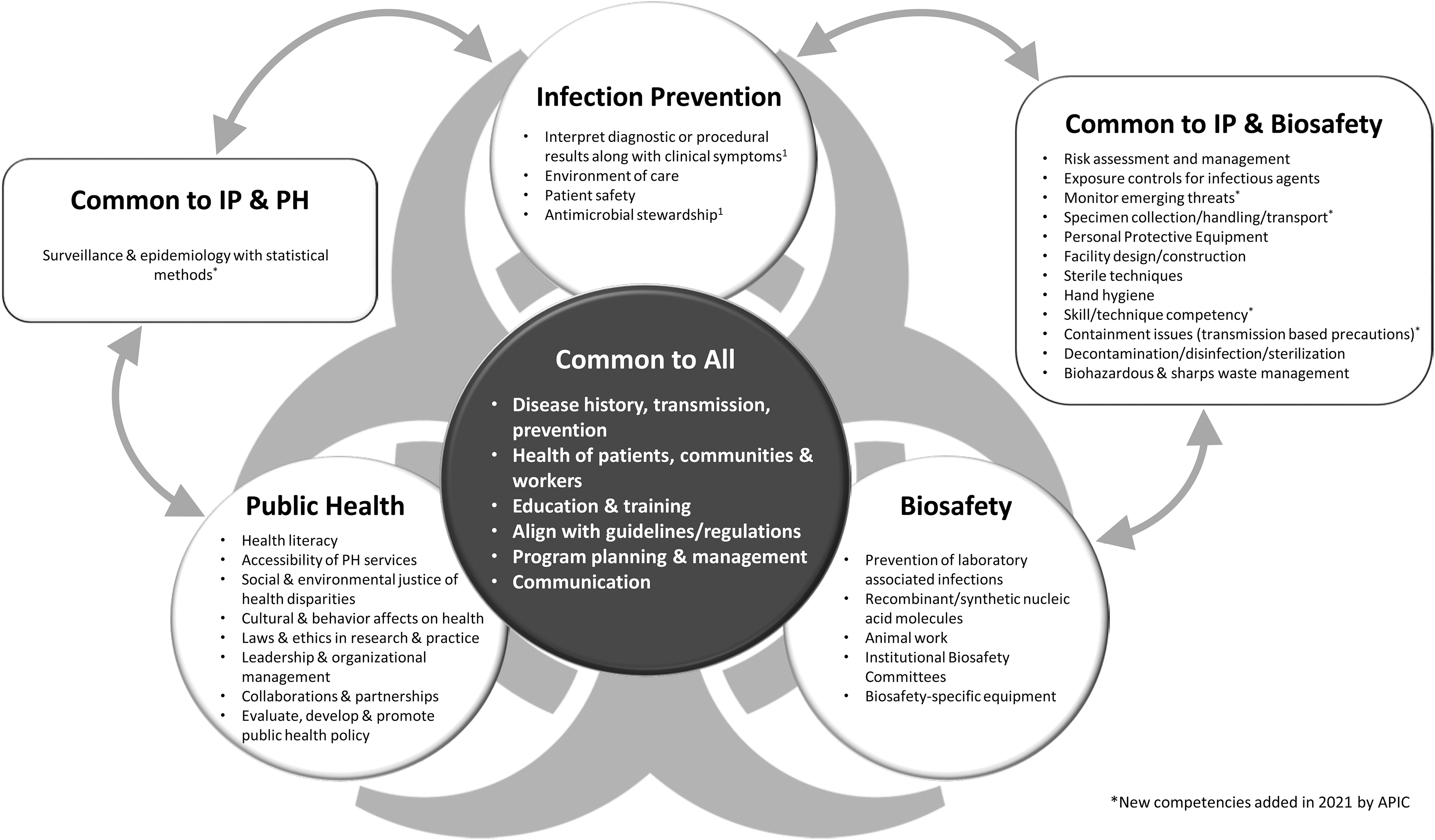
An annotated list of stated professional competencies for the biosafety, infection prevention, and public health professions, as stated by ABSA-I, APIC, and APHA, respectively, are listed in the circles within this figure. In the center, overlapping competency categories applicable to all three professions are highlighted.
Note that although there are some overlapping areas between biosafety and public health as stated above, this figure does not display this overlap since the competencies are not explicitly listed at current.
Discussion
A general theme that emerged from the assessment conducted and summarized in this study, beyond the common core of knowledge items identified, is that the variation in the competencies is seemingly driven by (1) the primary target population the profession intends to protect and (2) the setting where these professionals typically work. For example, biosafety professionals typically implement controls, such as engineering and administrative controls, which are identified and implemented based on the knowledge and understanding of the specific pathogenic organism(s) that are known to be or expected to be present within the controlled environment of the laboratory setting.
Some exceptions can exist such as if unknown organisms or novel organisms, which we have limited knowledge or understanding of may are present, in which case we may need to rely on interim biosafety guidelines that are issued and frequently updated as more is learned about the unknown or novel pathogen. A recent example is the Center for Disease Control and Prevention's Interim Laboratory Biosafety Guidelines for Handling and Processing Specimens Associated with Coronavirus Disease 2019 (COVID-19). 6
Conversely, infection prevention professionals and public health professionals may or may not have knowledge of the diseases or the causative pathogenic organisms they are encountering, until, for example, confirmatory testing is conducted to provide definitive information. Consider the early stages of an outbreak situation involving an unknown or a novel pathogen—specific controls or precautions may not be straight forward or fully understood—and vulnerabilities exist to workers and the general public, such as disease transmission. This suggests that some focused cross-training and awareness among these three professions may be beneficial. This is especially true when collective resources become constrained during pandemic situations.
Public Health Resources and Actions
This necessary cooperation and coordination among biosafety, infection prevention, and public health professions can best be illustrated by reviewing the five infectious disease issues facing our planet as described within the Global Health Security Agenda.
7
These include the following:
The emergence and spread of new microbes The globalization of travel and food supply The rise of drug-resistant pathogens The acceleration of biological science capabilities and the risk that these capabilities may cause the inadvertent or intentional release of pathogens Continued concerns about the acquisition, development, and use of biological agents by state or non-state actors.
Addressing these five issues requires close cooperation and collaboration between the three professions we describe in this assessment, along with others.
Efforts to enhance this close cooperation and collaboration are currently underway. For example, the State of Texas is preparing for the inevitable next public health threat by forming a new state agency, the Texas Epidemic Public Health Institute (TEPHI). 8 In 2021, the Texas Legislature, with approval of Governor Greg Abbott, created and funded TEPHI and housed it within The University of Texas Health Science Center at Houston (UTHealth) to create linkages among local and statewide agencies, businesses, and community leaders, and combine existing resources and expertise to form a robust public health reserve, strengthen the resiliency of the state's workforce and infrastructure, and develop an integrated research program.
To promote access to public health training, TEPHI has developed a certificate program in pandemic preparedness and response. The certificate, available in spring 2022, is designed for public health personnel who have not received formal training in public health and for people interested in public health. All activities are online and it includes four asynchronous online courses and a capstone exercise:
Epidemiology 101—this course is an overview of the causes of health outcomes and diseases in populations, and it includes disease distribution, determinants, control, and prevention.
Surveillance of Infectious Diseases—this course provides learners with an introduction to the characteristics of surveillance systems and how data from these systems are used to detect infectious disease outbreaks and other threats to public health.
Foundations of Infectious Diseases—this course covers the biology and epidemiology of infectious diseases, including emerging and re-emerging diseases. It also covers the use of epidemiological methods to investigate outbreaks.
Public Health Emergency Preparedness and Response—this course introduces learners to the key concepts of emergency preparedness and response, and includes the National Incident Management System (NIMS) training.
Capstone tabletop exercise—in this exercise, learners will combine their new knowledge and skills to detect and respond to a public health emergency.
Possible Next Steps for Consideration
To address the challenges ahead, ABSA, APIC, and APHA can enhance their respective response readiness to infectious disease outbreaks by considering the following options and opportunities:
At the grassroots level, local affiliate chapters of these professional organizations may consider extending invitations to speakers (to their respective meetings) to describe the competencies that reside outside of the sphere of commonalities. For example, members of the Southern Biosafety Association (SBA), a recognized ABSA affiliate, delivered a presentation to the local Houston area APIC chapter during a convened meeting on the basics of biosafety in May 2016. The interaction was warmly received and established a connection between biosafety and infection prevention based on the improved understanding of the respective professions. These interactions and enhanced relationships have proven fruitful during subsequent disease outbreak situations such as Zika and COVID-19 where local communication and collaboration was anecdotally observed to be enhanced between the groups.
ABSA might consider a dedicated focus on requests submitted for professional development courses on topics that do not reside within the sphere of commonalities during its annual biosafety conference. Such presentations might be provided by ABSA members as well as members of these parallel organizations.
From a strategic standpoint, in this new environment amid the ongoing COVID-19 pandemic, a reassessment of the stated CBSP competencies might produce an additional set of competencies that include some of these non-commonality topics. Training in these non-biosafety-related areas could be beneficial given the anecdotal feedback obtained from biosafety professionals who participated (in various capacities) in serving their organizations and the general public during the pandemic. This training could be incentivized through the issuance of additional credentialing maintenance points for the CBSP credential or RBP designation.
Consider a periodic “mega meeting” to be held every 3–5 years perhaps. Ideally, all three organizations will collaborate to produce a single meeting that includes plenary and profession-specific tracks. A suggested format for such a meeting could include sessions that include all participants to discuss issues inherent to the identified commonalities, and then additional sessions could consist of breakout sessions focused on issues inherent to the various specialty professions.
Summary
The five issues described in the Global Health Security Agenda suggest that there is an increasing need for all professions involved in the response to infectious disease outbreaks to optimize services by closely collaborating, communicating, and coordinating activities. The biosafety, infection prevention, and public health components of these responses are critical and cross-training opportunities exist to ensure the best possible outcomes, especially amid the current ongoing COVID-19 pandemic and surely for future outbreaks as well.
Footnotes
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Authors' Disclosure Statement
No competing financial interests exist.
Funding Information
The P2R Consortium is supported, in part, by the National Institute of Environmental Health Sciences of the National Institutes of Health under Award No. U45ES019360.