
Abstract
Incidental findings are common and commonly missed. The end result is late diagnosis of cancer and a missed opportunity for cure. This problem is pervasive, and is due to systemic and systematic issues with data volume, data fidelity, workflow, oversight, accountability, care handoffs, tracking, and system complexity. There are at least 15 human steps that must happen flawlessly for a patient with an incidental finding to complete the most appropriate follow-up evaluation. Artificial intelligence solutions can improve some of these steps, but there are currently limitations that preclude efficiently and effectively expanding across data sets and across incidental types. A more comprehensive solution is needed that addresses all the care failure steps. Examples of partial, more comprehensive, and complete solutions are described.
No provider gets up each morning and says “today, I plan on missing cancer.” Yet it happens daily, it has happened on your watch, and it may have happened within your family. The good news is this is a fixable problem. But like all problems, there is a method to creating a solution that is effective, efficient, scalable, and sustainable.
The primary focus of this commentary will be on incidental findings, which are common and commonly missed. As an example, over a third of chest computed tomography (CT) scans will have an incidental pulmonary nodule (IPN), the rate of malignancy for IPNs overall is ∼5%, and follow-up IPN care fails in ∼50% of cases (range 30–70%).1–3 This means that for every 120 chest CT scans you read or order, 1 lung cancer will be missed. And this is just one imaging modality, and one type of incidental finding, for a systemic and systematic problem.
Why Does This Problem Exist?
These are among the most critical elements driving the failure to reliably follow-up on incidental findings:
High data volume—health care systems rely on thousands of individual providers to process critical tasks and details at a time when they are already overwhelmed by information. Low data fidelity—there is no process to assure that the information being created is accurate, complete, consistent, and timely. Lack of workflow standardization—there is no workflow standard to assure that care is reliable, timely, patient centered, and of high quality. No process oversight—there is no defined ownership and accountability of the care process overall, or its individual parts. No defined accountability—by definition, an incidental finding is something discovered that was unanticipated. As such it may be viewed as “someone else's responsibility,” leading to confusion as to who is accountable for pursuing the workup. Care handoff failures—the transfer of care and the critical information needed are fraught with failure. Unreconciled events—there is no reliable reconciliation (tracking) process if a needed event or task fails to occur. Multiple steps/system complexity—the system is highly complex, with multiple failure points.
This final driver of care failure bears further exploration. Take, for example, an incidental finding seen on CT scan where the correct care plan is a follow-up CT. Sounds simple—test resulted … new test done. However, there are at least 15 critical human steps that must happen flawlessly for the correct care plan to be executed (Fig. 1). And as previously cited, this happens ∼50% of the time. That is akin to the pilot announcing, “There are fifteen steps we must do before takeoff, but don't worry, we usually complete about eight correctly.” You and I would exit the plane. But in health care, our patients do not have that option. They are at our mercy, and they need to have faith that we will get it right. And we do—50% of the time.
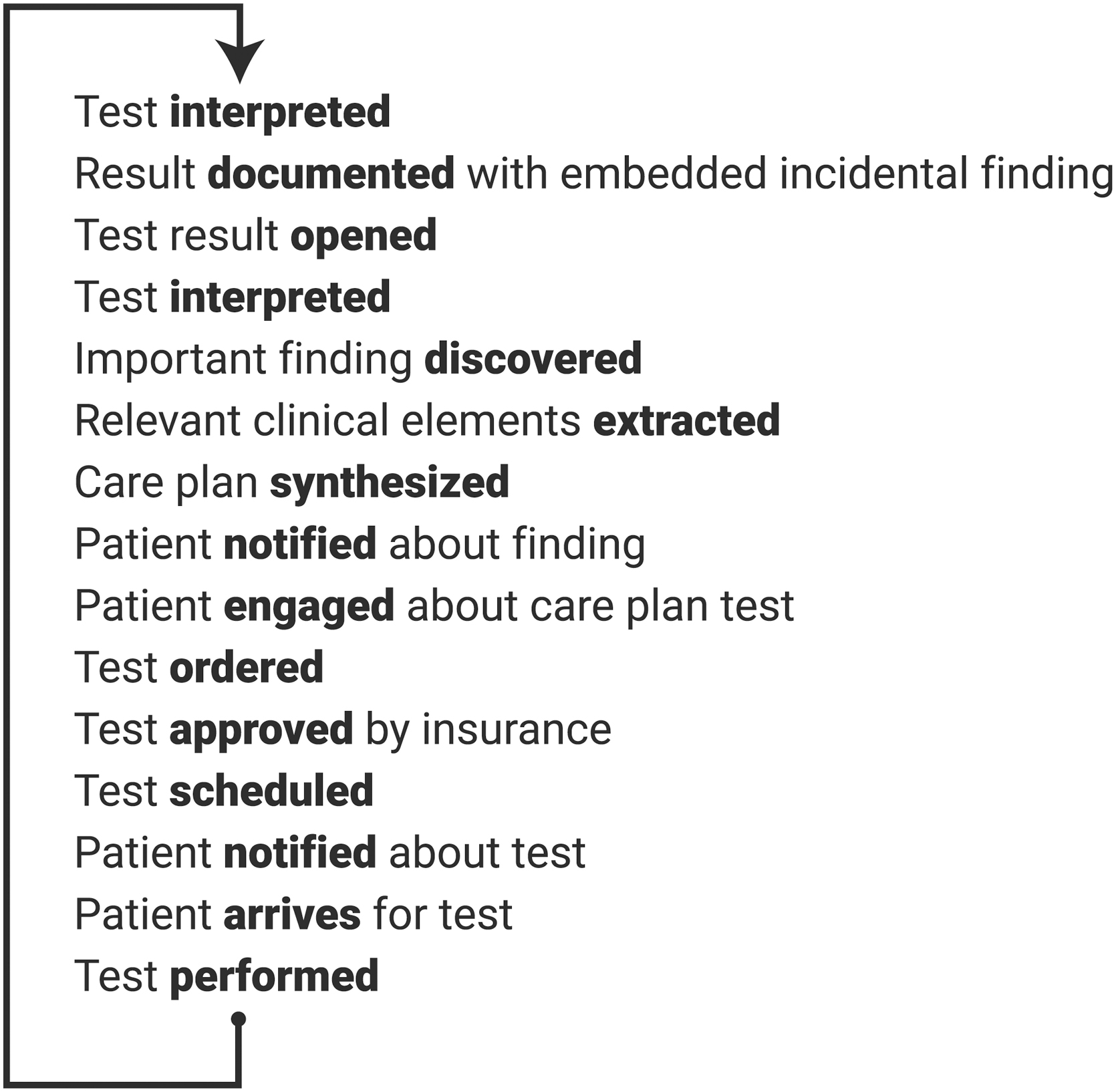
Fifteen human steps are required to assure reliable incidental finding follow-up. Bold text emphasizes the action required for each of the steps.
Partial Solutions
We can simplify the system for managing incidental findings into seven critical steps that we want to happen flawlessly:
Abnormality identified
Care plan created
Patient/provider notified
Test scheduled
Care plan tracked
Next test resulted
Process measured
Although it is tempting to focus on trying to fix just one step—a partial solution—you cannot change one part of a system without risking significant unanticipated (and in health care, often unmeasured) side effects. Fix one thing in a broken system, and something else pops up—upstream or downstream. Or maybe you improve one piece, but the ultimate outcome does not change. Either way, you did not solve the problem.
Let us examine such a partial solution using artificial intelligence (AI). AI is used most commonly in step 1—the identification of an abnormal incidental finding. Researchers at Northwestern Medicine designed an AI natural language processing (NLP) system to flag radiology reports with findings that needed follow-up. 4 Their clinical validation showed a sensitivity of ∼70%, suggesting that the system missed 30% of findings. In addition, their system then signaled the physician using best practice alerts (BPAs), which are ignored or overridden in some studies 50–95% of the time. 5 In addition, BPAs are a source of increased work for already overburdened providers—potentially increasing the likelihood of other mistakes being made.
Another partial use of AI is identification of an abnormality from the image itself. The potential for AI-based image analysis to improve detection has led to an explosion of AI software programs and companies. As of October 2023, the Food and Drug Administration has approved 863 different AI systems, 80+% of which are in the radiology space. 6 Although there is great promise for improving nodule identification and characterization using AI, there are limitations and concerns for utilizing this technology alone to help us stop missing cancer. First, every company has their own proprietary algorithms, and every abnormality will require its own algorithms, so expanding beyond pulmonary nodules to other organs/cancer risks is both limited and potentially very expensive (cannot “go wide”).
Second, most solutions are trained on a small subset of patients, and the results may not apply to other patient groups for the same abnormality (cannot “go deep”). Finally, although AI algorithms may make it more efficient for the radiologist, this may translate into the radiologist being asked to read more studies (potentially increasing human error).
Even if there were a robust set of algorithms that identified and characterized many types of abnormalities, this solution only helps with the first of the seven steps above. Importantly, if AI improved Step 1 alone, the increase in throughput volume could overwhelm the downstream steps, resulting in a potentially catastrophic failure of the rest of the process.
More Comprehensive Solutions
To solve the problem of missing cancer, we need to focus on solutions that address all seven steps. To that end, health care groups have developed successful incidental lung nodule programs. 7 –10 These programs commonly include three critical components:
People (lung navigators and subject matter experts)
Process (specific clinical pathways designed to mimic guidelines)
Information technology (using spreadsheets, electronic health record functions, proprietary software, or commercially available software)
But not every program effectively addresses each of the seven steps. As an example, the Finding Incidental Disease program employed tracking software to follow-up on radiology reports flagged as having an important incidental finding and nurse navigators to remind the ordering physician to follow-up on the abnormality. 8 Follow-up imaging completion increased from 30.8% to 50.7%—statistically significant but clinically inadequate. Dyer et al. also studied the effect of a follow-up imaging tracking and reminder program and found similarly inadequate levels of improvement—46% follow-up prestudy versus 55% with the new system. 9
This illustrates the importance of not only addressing all the process steps, but also the criticality that every step be reliably completed. In addition, it shows that measurement of the process is a fundamental tenet. Without measurement, a program can be instituted (in good faith) but not improve care (and not know that it has failed).
Replacing the Existing System with a Comprehensive End-to-End Solution
An efficient, effective, sustainable, and scalable solution cannot be created by fixing one piece of a dysfunctional system, nor by introducing untested and repurposed functionality that was not designed for that system. What is needed is a new system of care that has extremely high efficiency, effectiveness, reliability, and patient centeredness.
The ideal end-to-end solution
Identifies documented incidental findings across a broad array of target organs/systems (breast, lung, thyroid, pancreas, liver, kidney, and vascular). An advanced AI-driven functionality such as computational linguistics (CL) will assure identification with extremely high recall and precision that is critical to reliable and efficient care delivery. Unlike NLP, which looks for specific content, CL is a semantics model—it understands both content and intent. That is, not just what was said but what was meant. The result is a model that understands medical jargon, does not require any alteration in radiologist dictation, and is scalable across different organ systems.
Creates a care plan that is guideline driven and adjustable by the specialist.
Tracks that care plan until it is completed early by a similar qualifying study, it is completed on time, or alerts providers if it is overdue.
Communicates proactively with providers and with patients.
Sets a final outcome such as the abnormality needs no further follow-up or cancer has been diagnosed.
Reports on program findings including demographics, efficiency, and effectiveness.
Ultimately, the ideal end-to-end solution, one that incorporates the six features described above, becomes a very effective tool that can be integrated into and used to manage both tumor boards and incidental findings clinics. With the confidence that patients with incidental findings are identified for tracking with high recall and precision, the system would allow real-time creation or modification of the care plan that can then be effectively communicated to both patients and providers who may or may not be part of the tumor board or incidental findings clinic discussion. Lastly, being able to track the effectiveness of interventions provides the ability for complex analytics and reporting to be generated as part of the tumor board.
Conclusion
The current health care system for diagnosing cancer commonly fails, not because of bad people, but because of bad process. Addressing only part of the process (e.g., AI for identification) does not solve the problem. The best system solution uses AI to address all the failure points, integrates with existing processes and tools, and reduces work and worry, so we do not miss cancer.
Footnotes
Authors' Contributions
S.S. contributed to data analysis and interpretation (equal); conception or design of the study (equal); data collection, analysis, and interpretation (equal); drafting the article (supporting); critical revision of the article (equal); and final approval of the version to be published (lead). E.N. carried out data analysis and interpretation (equal); conception or design of the study (equal); data collection, analysis, and interpretation (equal); drafting the article (lead); critical revision of the article (equal); and final approval of the version to be published (supporting).
Author Disclosure Statement
S.S. works as chief medical officer for Eon. E.N. has done consulting work for Eon.
Funding Information
There was no funding for this study.