
Abstract
Antiretroviral therapies (ARTs) benefit millions with human immunodeficiency virus. However, concerns about subsequent weight gain and related metabolic complications have emerged. Early ARTs are associated with adipose tissue changes. While newer ARTs may have fewer adipose alterations, it is unclear whether they lead to increased weight gain. A systematic literature review was performed to describe current published literature describing the use of newer ARTs, weight gain, and related comorbidities. Titles and abstracts were screened, focusing on studies that examined ART initiation and subsequent weight gain; publications were then ranked based on publication type, methodology, and comorbidities, emphasizing US studies with large patient cohorts. This yielded a comprehensive review of the 50 publications on weight gain and a range of related comorbidities, including diabetes and hypertension. Most of the studies describing weight gain found the most significant gains during the first year after initiating ART. Overall, patients gained ∼5 kg 18–96 months after initiating ART. Many of the studies reported altered weight-related comorbidities, including increased risk of diabetes and hypertension. Despite an expectation that newer ARTs may be safer, a review of the literature suggests that contemporary ART use is associated with pronounced weight gain and related comorbidities. Future studies should define and quantify the direct role of newer ARTs in weight gain and related comorbidities, as well as clarify the role of specific drug classes in metabolic disturbance, to improve intervention strategies.
Introduction
Newer antiretroviral therapies (ARTs), herein defined as those developed since 2000, have helped improve the prognosis for people living with human immunodeficiency virus (HIV; PLWH) by providing better control of viral suppression and earlier protection of the immune system with a postdiagnosis initiation of ART sooner than in the past. Over the past 20 years, ARTs have advanced, leading to a decrease in pill burden, improved efficacy and safety, and an increase in the number of ARTs available. As a result, PLWH are living longer lives, and an HIV infection diagnosis has largely evolved from a death sentence to a chronic condition.
Despite the successes of early ARTs in reducing viral load and preventing the onset of acquired immunodeficiency syndrome (AIDS), noticeable metabolic complications have been reported over time in patients taking ART, in particular: an increase in lipodystrophy, including lipoatrophy, lipohypertrophy, hyperlipidemia, and insulin resistance as well as diabetes. 1,2 Specifically, use of older nucleoside reverse transcriptase inhibitors (NRTIs) and older generations of protease inhibitors (PIs), but not non-nucleoside reverse transcriptase inhibitors (NNRTIs), was associated with increased lipodystrophy and has resulted in long-term consequences of altered fat accumulation and metabolism and may lead to increased mortality. 3,4
Concerns remain as PLWH continue to age. 5 Metabolic complications are a growing concern in an aging population coupled with increasing prevalence of PLWH who are overweight or obese, but concerns on weight gain associated with newer ARTs are also arising in treatment-naive and virologically suppressed patients. 6 Newer ARTs, such as integrase inhibitors (INSTIs), succeeding first-generation ARTs beginning in 2005, were thought to reduce metabolic comorbidities. While recent studies have demonstrated less fat redistribution and related metabolic complications, such as lipid abnormalities and hyperglycemia, among new ARTs, it is unclear whether all metabolic comorbidities are completely or clearly abrogated with newer ARTs. 7
We performed a systematic review to identify literature to better understand the clinical and economic burden of weight gain in PLWH who take newer ARTs and the associated short- and long-term weight gain–related comorbidities. Following the systematic review, more recent studies were reviewed to account for newly emerging evidence, including abstracts from relevant conferences, to determine the most current information about newer ARTs.
Methods
Research questions
Research for this review focused on two main questions: What is the clinical burden of weight gain and weight-associated comorbidities in PLWH on newer ARTs? What is the economic burden of weight gain and weight-associated comorbidities in HIV patients on newer ARTs?
Systematic identification and screening strategy
Identification
Using the guidelines of the “Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols” statement (Fig. 1), 8 a comprehensive search strategy was devised to identify studies and review articles by (1) directly querying electronic databases, and (2) screening lists of results from the direct query in (1). For all searches, filters were applied using terms directed to (1) HIV, (2) AIDS, and (3) ART (or combined ART). For systematized searches, filters were applied using terms directed to (1) weight, (2) consequences, (3) sleep apnea, (4) renal disease, (5) diabetes, (6) hypertension, (7) nonalcoholic steatohepatitis, (8) quality measures, and (9) economic burden. Only human studies were considered, including those that were conducted in or contemplated humans. A date limit of articles published in 2010 and later was applied to focus on outcomes associated with newer ART. Articles selected were published in English. Records were identified through database searches of PubMed, Medline, Embase, and Google Scholar on August 21, 2019.
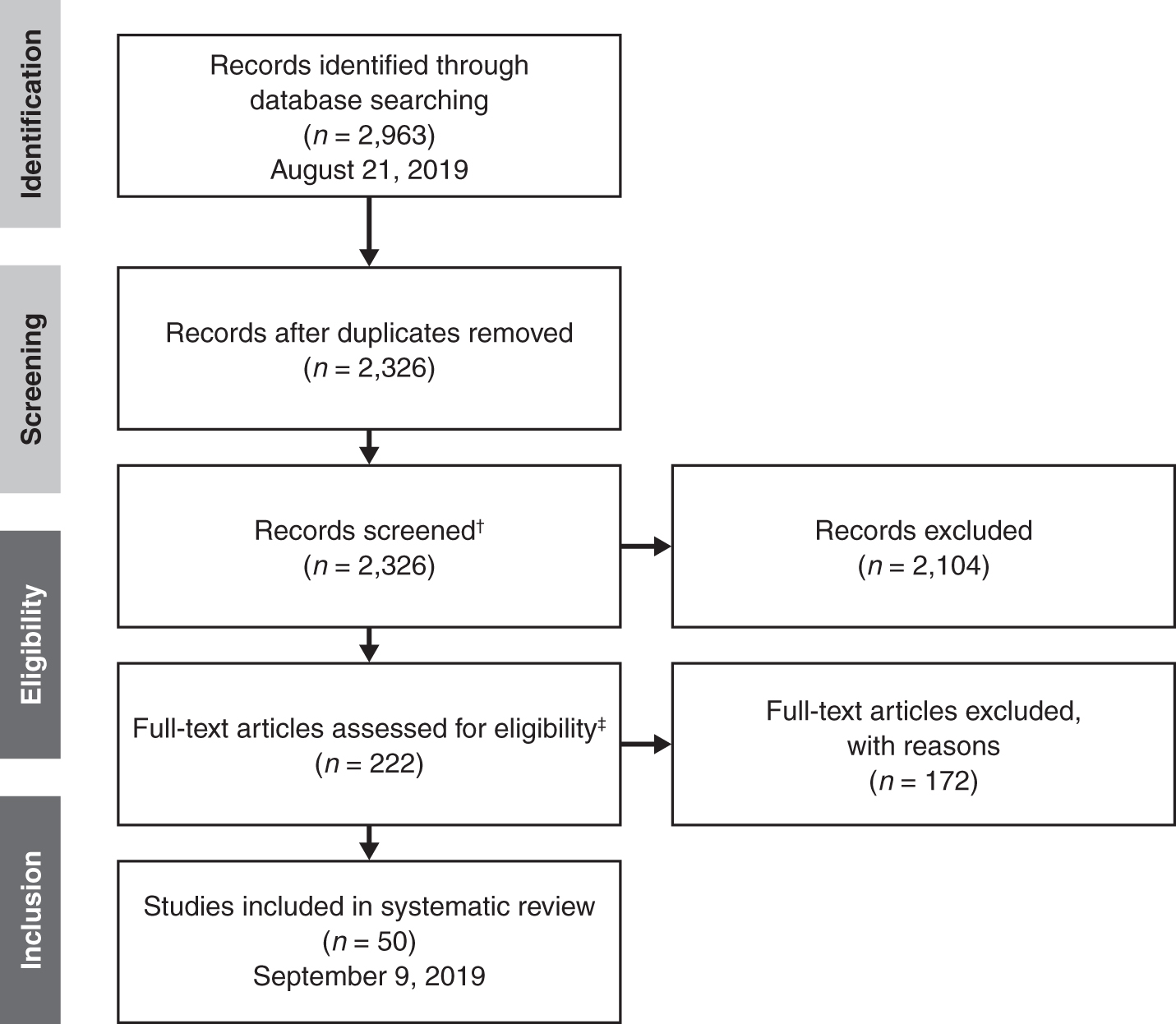
The systematic literature review was completed using the PRISMA approach.* *A systematic approach was used to identify and screen records. Records were then assessed for eligibility and inclusion in the targeted literature summary. †Records were screened by title and abstract using the following criteria: publication type, methodology, comorbidities discussed, country of origin, population examined, and nonclinical outcomes, including economic impacts. ‡Full-text articles were ranked for inclusion based on: publication type, primary literature study type, topic/comorbidities, country of origin, and patient cohort size. The 50 highest ranking records were retained. ARTs, antiretroviral therapies; HIV, human imunodeficiency virus; PRISMA, preferred reporting items for systematic review and meta-analysis; PLWH, people living with HIV.
Screening
One author (H.S.) conducted the initial literature search (n = 2,963 records identified) and removed duplicate articles. Four authors (M.A., H.S., A.V., and Z.Z.) screened the remaining 2,326 publications by title and abstract based on the following criteria:
Publication type (primary literature > review literature)
Methodology in primary resources [(randomized control trial > real-world evidence); (observational studies > prospective studies or retrospective studies)]
Comorbidities discussed (including cardiometabolic, hepatic, and renal)
Country of origin (US > ex-US)
Generalizability of population examined
Nonclinical outcomes, including economic impacts
This resulted in 222 records being retained for assessment for eligibility for the targeted full-text literature review.
Eligibility and inclusion criteria for targeted full-text review
Eligibility
Our targeted full-text review contained the 50 articles that represented recent evidence across a breadth of relevant topics. Eligible articles were chiefly primary literature, although review articles were included and journal impact factor was considered. The central focus was on HIV comorbidities related to weight gain, including diabetes and hypertension, and an attempt was made to encompass an even distribution of comorbidities and to include economic impacts of comorbidities in PLWH on ART. Renal, hepatic, and other cardiac comorbidities were also considered. For the primary literature, randomized control trials were preferred over observational studies or meta-analyses. Studies conducted in the United States were the focus, but other industrialized countries' populations were included. Large patient cohorts were prioritized: n > 100 for prospective studies and randomized controlled trials and n > 1,000 for retrospective studies.
Selections were compared among four authors (M.A., H.S., A.V., and Z.Z.), and the publications of highest ranking were selected for review. Alignment with the search criteria for full-text review was assessed by each author, in consultation with three other authors (W.C., J.L., and H.H.). This resulted in 50 highest ranking records retained, of the 222 screened.
Data extraction and synthesis
Four authors (M.A., H.S., A.V., and Z.Z.) extracted essential data from the selected publications to inform the review, including (1) publication characteristics (authors, date of publication, and journal), (2) population cohort characteristics (country of origin, number of patients, and identity, including age and sex), (3) dates of analysis, including length of study, (4) comorbidities or economic burden discussed in the publication, and (5) significant findings, data, and results relating to (6). Two authors (M.A. and A.V.) conducted a second review of selected publications to summarize results for the Results and Conclusions section, and then one author (H.S.) compiled results into this publication.
Conference abstracts
After reviewing the literature, it became evident that some of the newest studies covering the last 10 years may be absent from the peer-reviewed literature search that was completed. In addition, there was a lack of clarity about the role of specific classes of newer ARTs on weight gain. As such, the authors conducted an additional review of weight gain data presented from recent poster and oral conference presentations related to HIV and AIDS.
Specifically, the authors searched poster abstracts from the 2019 IDWeek, the 2019 Conference on Retroviruses and Opportunistic Infections (CROI), and the 2019 European AIDS Clinical Society (EACS) Conference using the terms “weight,” “co-morbidities” (“comorbidities”), “integrase inhibitors,” “antiretrovirals,” and “metabolism” (“metabolic”) to find abstracts focused on the role of specific ARTs on weight gain. All abstracts were compiled and evaluated before incorporation into the review.
All authors reviewed the publication before submission. As a systematic literature review, Internal Review Board approval was not applicable for this study.
Results
For the systematic literature review, 2,326 articles remained after duplicates were removed from 2,963 articles identified initially. Screening by title and abstract according to eligibility criteria resulted in 222 publications, which were ranked based on publication type (primary literature over review), methodology/study design, comorbidities, country of origin, population examined, and other analyses, including economic impacts. Selections were compared and the 50 highest ranking publications were included for review. The conference abstract review yielded 45 additional studies; of these, the abstracts most relevant (n = 27) to the 50 publications selected for the full-text review were included.
Weight gain
Overall, most of the 30 peer-reviewed articles describing weight gain found the most significant gains during the first year of ART initiation. Of these, 19 were studies or reviews completed in the United States. For some PLWH, this was consistent with “returning to health.” 9,10 However, while PLWH are historically thought of as being underweight, progress in the management and treatment of HIV, including starting treatment earlier, have contributed to making HIV more of a chronic condition, and trends in increased body weight subsequent to ART initiation have been described. 11,12 This may explain why in some cases, the number of PLWH who are considered overweight/obese [body mass index (BMI) ≥25 kg/m2] increased within the first year. 13
Data by duration of ART use and ART class
Increases in weight among users of ART after 1 year were found to be modest but significant. In a post hoc exploratory analysis of the AIDS Clinical Trials Group A5202 study, weight increased from baseline when ART-naive persons initiated ART [tenofovir disoproxil fumarate-emtricitabine (TDF/FTC) or abacavir-lamivudine, with efavirenz (EFV) or atazanavir-ritonavir at standard doses] by a mean weight of 4.8 kg and mean BMI by 1.5 kg/m2 after 96 weeks. 14
Studies also demonstrated increases in overweight and obese populations after 2 years on ART [≥2 NRTIs (stavudine, lamivudine, FTC, zidovudine, TDF, or abacavir) with ≥1 PI (lopinavir/ritonavir) or 1 NNRTI (nevirapine or EFV)]; in a study by Gomes et al., which focused on PLWH in the Dominican Republic starting ART within 90 days of enrollment, 13% became obese (18% were obese at baseline) while an additional 19% became overweight (27% were overweight at baseline). 15 In a prospective study by Tate et al., 44% of the population of treatment-naive PLWH in Birmingham, Alabama, was obese (BMI ≥30 kg/m2) or overweight (BMI 25–29.9 kg/m2) before initiating ART (an NNRTI, an NRTI, a PI, or a ritonavir-boosted PI), which increased to 56% after 2 years. 16
In a retrospective study in Rio de Janeiro, Brazil by Bakal et al., individuals who were overweight when they initiated ART (≥2 NRTIs and a PI, an NNRTI, or a PI and an NNRTI) had a higher risk of becoming obese and those who were underweight at baseline had the greatest annual change in BMI, with an increase in median BMI from 17.1 to 20.3 kg/m2 after 2 years. 17
Data by patient demographic characteristics
Interestingly, our review indicated birth sex differences in weight gain wherein female PLWH gain more weight than males. 11,18 In addition, one study by Taylor et al. focused on disparities in weight gain among minorities and uninsured populations by separating PLWH on ART (dolutegravir, raltegravir, elvitegravir, darunavir, and rilpivirine) into groups based upon race/ethnicity and health insurance status. Uninsured minorities gained weight more rapidly than insured white PLWH. 12
More recent data on INSTI class
When looking through newer research presented at conferences in 2019, most of the 45 discovered abstracts focused on or included an analysis of the role of taking INSTIs on weight gain. Of the 27 studies that focused on INSTIs, 82% (22/27) demonstrated a weight increase following INSTI treatment either when switching to an INSTI from another treatment regimen or when initiating an INSTI in ART-naive individuals. A study by Saber et al. reported a greater weight increase in PLWH who switched to an INSTI compared with those who did not switch. 19 In a retrospective analysis of 14,000 ART-naive PLWH by Koethe, there was a higher incidence of severe weight gain (>10% increase) in PLWH using the INSTI raltegravir containing regimens compared with those using the PI darunavir or atazanavir. 20
In some studies, PLWH who gained weight were more likely to be on an INSTI than an NNRTI or PI, 21 while others show that INSTI and PI use led to similar weight increases. 22 The remaining studies, 18% (5/27), showed no weight increase with taking an INSTI. Specifically, one study by Verboeket et al. presented at EACS 2019 matched 1:2:2 with (1) PLWH switching to INSTI to (2) nonswitchers to (3) HIV-negative participants and found no above average weight change across the three groups. 23
Diabetes
In the general population, the risk of developing type 2 diabetes mellitus (diabetes) is associated with being overweight or obese. 24 An increased risk of developing diabetes in PLWH treated with ART could be associated with increased weight gain with ART use as described in the previous section, or could be caused by HIV. 25 A study by Achhra et al. analyzed data from the Data Collection on Adverse Events of Anti-HIV Drugs (D:A:D) Study group, an observational study of >49,000 PLWH from 11 cohorts in the United States, Europe, and Australia, and described an increase in diabetes risk as BMI increased in PLWH treated with ART. 26
A separate risk analysis of diabetes onset in PLWH completed, in part, by the D:A:D Study Group incorporated factors, including age and HIV immunosuppression, but did not consider use of ART because of conflicting studies whether ART use increases or decreases risk of developing diabetes. The authors pointed to other studies that demonstrated contradicting results of increased or decreased risk of developing diabetes while taking PIs as a reason for not incorporating a direct relationship between ART use and diabetes into modeling, but reported a positive association between diabetes risk and BMI associated with ART use. 27
However, a meta-analysis of 41 observational studies evaluating PLWH who were either ART-naive or taking ART when tested showed increased fasting blood glucose levels and an increased risk for developing diabetes in those treated with ART. 28 A separate meta-analysis across 44 studies also demonstrated increased risk of diabetes development in some studies, but that ART was not a risk factor in all studies. 29 In an additional study by Lin et al. comparing Taiwanese PLWH on ART (most commonly ≥2 NRTIs with NNRTIs or boosted or unboosted PIs; INSTIs not clinically available during the study) with those not on ART, the risk of developing diabetes was associated with ART use (7.16% in ART-treated group vs. 2.24% in untreated group). 30
Hypertension and other cardiovascular complications
Increased risk of cardiovascular disease (CVD) has been described in PLWH regardless of ART use; however, the risk of CVD is lower in those receiving ART than those not receiving ART. 31,32 While some classes of ART are implicated in an increased risk of CVD, 33 this review focused on risk of hypertension, changes in blood pressure, and hyperlipidemia associated with ART to avoid the well-described confounding influence of HIV on CVD risk overall. Most studies demonstrated an increased risk of hypertension with ART use. 34 –38
However, some studies demonstrated a low association between nevirapine and hypertension, 34 while others demonstrated no link between use of ≥2 NRTIs with either an NNRTI, a boosted PI, or an INSTI and hypertension. 39 Higher blood pressure and high triglyceride levels were also reported in PLWH using ART. 39,40 A meta-analysis of 39 studies revealed higher levels of hypertension in those who used ART compared with those who were treatment naive. 41 A review article by Auerback and Abouliafia focused on thromboembolic complications associated with ART use and reported an increase in noncirrhotic portal hypertension in ART users. 42 Periaortic and epicardial fat is correlated with increased hypertension in PLWH on ART. 43
Overall, these results demonstrate increased hypertension, changes in blood pressure, and high cholesterol associated with ART use in PLWH.
Other weight related comorbidities
Our search revealed additional weight-related comorbidities. For example, metabolic syndrome (MetS) is defined as central obesity and metabolic abnormalities that ultimately increase the risk of developing weight-related comorbidities. Previous studies demonstrated that among PLWH, the incidence of MetS increased and the prevalence remained high after initiating ART (3 NRTIs, ≥2 NRTIs with an NNRTI or a boosted PI, or an NNRTI with a boosted PI). 40,44
PLWH also have higher rates of chronic kidney disease (CKD) and some evidence demonstrated an increased risk with ART use. 45 –47 Specifically, compared with PLWH with normal renal function, PLWH with mildly reduced glomerular filtration rates were older, more likely to be female, have higher BMI, and use the NRTI TDF or the PI ritonavir. 45 Other studies showed an increased risk in developing CKD with a ritonavir-boosted PI combined with TDF compared to PLWH treated with a NNRTI combined with TDF, but noted that the risks were small. 48,49 Another study demonstrated no link between specific ART agents and CKD; however, there was a significant association between duration of ART and renal impairment. 50
Generally, PLWH have higher rates of liver MetS. 1 PLWH have higher risk of liver disease due, in part, to HIV itself and certain ART agents, compared to patients who do not. 42,51 A study by Mohr et al. indicated that HIV viral load is associated with higher rates of liver fibrosis and suggested that use of ART may decrease liver fibrosis by decreasing viral load. 52
Economic burden
One additional consideration of our review was economic consequences and health care resource utilization arising from comorbidities associated with HIV and ART. As the population of PLWH who use ART ages, the burden of comorbidities has increased. 32 There is a direct cost impact from diabetes and lipid disorders in PLWH on ART; PLWH with diabetes incurred on average $5,361 higher medical costs annually compared to PLWH without diabetes in a study completed by Dekoven et al. that analyzed medical claims during September 2006 to June 2012. 53
A study by Gallant et al. examined increased all-cause health care utilization and costs in PLWH associated with CVD or CKD and reported an increased cost per patient per month (PPPM) that ranged from $1,400 to $5,000. 54 A study by Johnston et al. compared health care costs between two PIs, atazanavir and darunavir, and found an increased cost PPPM in all-cause health care costs in darunavir-treated PLWH but reported no difference in health costs for specific adverse effects (gastrointestinal, lipid abnormalities, diabetes/hyperglycemia, rash, and jaundice). 55
Discussion
This review demonstrated that newer ART regimens are likely associated with increased weight and weight-related comorbidities, specifically diabetes and hypertension, but some data suggest a lower association with newer ARTs and metabolic effects compared to agents approved before 2000. 56 However, even in the time span reviewed, the components/boosters in ART regimens or combinations have changed, which may also confound the association.
The review focused on how any ART influences weight gain and related comorbidities, but the search revealed that specific classes of ART may influence weight gain differently. In an Italian cohort of treatment-naive PLWH comparing the INSTIs dolutegravir, raltegravir, and elvitegravir, the PI darunavir, and the NNRTI rilpivirine, Taramasso et al. reported that all PLWH had significant increases in BMI after 1 year, but showed no differences between product classes. 57 However, in the Brazilian cohort of Bakal et al.'s study in Brazil (n = 1,794), those using an INSTI (n = 14) had greater annual BMI change compared to those whose core drug was an NNRTI (n = 1,038) or PI (n = 515). 17 In another direct comparison of treatment-naive PLWH starting ART, Bourgi et al. reported PLWH on the INSTI dolutegravir gained more weight (6.0 kg) after 18 months compared with those on an NNRTI (2.6 kg) or the INSTI elvitegravir (0.5 kg). 58 A pooled analysis of eight clinical trials reported that INSTIs were associated with more weight gain than PIs or NNRTIs. 59
The results from the review of conference abstracts also supports INSTIs increasing weight over other ARTs. A recent review by Hill et al. suggests that a growing body of evidence is accumulating on the use of INSTIs and their potential association with significant increases in body weight and even clinical obesity, although it is unclear whether these changes are clinically significant. 6 The authors point to the fact that the effects of an INSTI on body weight need to be analyzed particularly for women and by race, because current evidence suggests different effects. Another recent publication points in the same direction; a recent pooled analysis of eight clinical trials reported that INSTIs were associated with more weight gain than PIs or NNRTIs. 59 Future studies should incorporate prospective study designs and consider comparing various ART regimens to determine the role of each class in weight gain. In addition, weight gain may differ between treatment-naive and -experienced or virologically suppressed switcher patients.
Similarly, direct links between ART classes and comorbidities related to weight gain are not clear. A study by Johnston et al. compared the two PIs darunavir and atazanavir and showed that there was no significant difference despite a numerically lower risk of diabetes and hyperglycemic adverse events in those treated with darunavir ≥6 months after starting ART. 55 Another study by Capeau et al. showed that diabetes development after 10 years is associated with older age and being overweight but was also common in PLWH who used the PI indinavir or the NRTIs stavudine or didanosine. 60 Comorbidities associated with HIV may be exacerbated by ARTs, HIV infection, or weight gain, 61 and future prospective analyses may further elucidate ART-associated risks.
It is difficult to define whether the observed increases in weight are solely a direct result of taking ART or are due to other environmental or population factors that influence weight gain, including social determinants of health. Supporting the latter, some research suggests that developing weight-related comorbidities is preventable. In a study performed by Manne-Goehler et al. in rural South Africa, PLWH treated with ART had greater access to diabetes and hypertension diagnosis and prevention counseling than the general population, which ultimately reduced overall disease burden in this population. 62 Practices like this may be worth replicating in other populations in other countries to attempt to reduce the risk of developing comorbidities following ART initiation and to manage the chronic nature of HIV.
Comparisons in weight gain between uninfected populations and PLWH treated with ART make it hard to distinguish whether ARTs or HIV infection are the direct cause for increased weight gain. 63 In addition, whether weight gain is caused by ARTs or is a consequence of improved overall health from the beneficial effects of ARTs in tandem with living a western lifestyle is not abundantly clear, but consistent and statistically significant correlations were found among the literature for the former. 61 BMI before initiating ART is not always reported, 12 which makes it challenging in some cases to determine whether changes in weight were directly associated with ART use.
This review encompassed a few limitations. Study designs make it difficult to draw direct comparisons of the total amount of weight that is gained, as some studies report changes in BMI 17,26 or kilograms, 14,58 while others place PLWH into BMI-based categories and report whether they became overweight or obese during the time period described. 11,15 Future study designs should consider reporting all three variables to provide more robust conclusions. As well, this review did not distinguish between PLWH who were ART-naive from those switching to new therapies; such differences may influence weight gain and related comorbidities. Another limitation is that many PLWH were treated with multiple ARTs at once, so it is possible that the combination confounds the impact of ART on weight gain and related comorbidities as well. Furthermore, the retrospective or observational nature of the studies may prevent causal relationships from being established. In addition, the criteria used to select studies for this systematic review did not preclude overlap between review articles and primary literature. Finally, this study did not investigate publication bias, which refers to an increased likelihood that studies with significant results will be published over those with null findings. This may lead to an overrepresentation of “positive” studies and undermine the validity of systematic reviews.
An understanding that ARTs increase weight and related comorbidities can lead to best practices implemented by providers that could ultimately identify at-risk populations to reduce disease burden. Of note, December 2019 Department of Health and Human Services Guidelines for ART Use has been updated to reflect recent evidence on the association of INSTI with greater weight gain than NNRTI or boosted-PI regimens. 64 Future studies that clarify the direct impact of newer ARTs, particularly INSTI, on weight gain and related comorbidities could support more effective management and early intervention of HIV-infected patients receiving ART regimens and correspondingly decrease economic burden. HIV infection has become a chronic condition, and with an aging population, weight gain and its potential implications should be top-of-mind when selecting ARTs.
Footnotes
Authors' Contributions
H.S., Z.Z., and M.A. participated in the conception and design of the study, acquisition/collection of the data, and analysis/interpretation of the data. J.L., W.C., C.S., R.H., and H.H. participated in the conception and design of the study, and analysis/interpretation of the data. A.V. participated in the acquisition/collection of the data, and analysis/interpretation of the data. All authors contributed to drafting/critical review of the article and approved the final version. Editorial support was provided by Caryn Gordon, PharmD, of Cello Health Communications/MedErgy, and was funded by Janssen Scientific Affairs, LLC.
Author Disclosure Statement
Z.Z. is an employee of Avalere Health—an Inovalon Company, which was retained by Janssen Scientific Affairs, LLC, for work and publication related to this systematic literature review. H.S., A.V., M.A., and C.S. were employed by Avalere Health at the time of this analysis. R.H. was employed by Avalere Health at the time of this analysis and is currently employed by Moderna as Vice President, Public Policy. J.L. is employed by Janssen Scientific Affairs, LLC, and owns Johnson & Johnson stock or stock options. W.C. was employed by Janssen Scientific Affairs, LLC, at the time of this analysis and owns Johnson & Johnson stock or stock options. H.H. was employed by Janssen Scientific Affairs, LLC, at the time of this analysis and is currently employed by Janssen Research & Development, LLC, and owns Johnson & Johnson stock or stock options.
Funding Information
This study was funded by Janssen Scientific Affairs, LLC.