
Abstract
Objective:
To develop evidence-based recommendations on best practices for delivery of clinical preventive services by chiropractors and to offer practical resources to empower provider applications in practice.
Design:
Clinical practice guideline based on evidence-based recommendations of a panel of practitioners and experts on clinical preventive services.
Methods:
Synthesizing the results of a literature search for relevant clinical practice guidelines and systematic reviews, a multidisciplinary steering committee with training and experience in health promotion, clinical prevention, and/or evidence-based chiropractic practice drafted a set of recommendations. A Delphi panel of experienced practitioners and faculty, primarily but not exclusively chiropractors, rated the recommendations by using the formal consensus methodology established by the RAND Corporation/University of California.
Results:
The Delphi consensus process was conducted during January–February 2021. The 65-member Delphi panel reached a high level of consensus on appropriate application of clinical preventive services for screening and health promotion counseling within the chiropractic scope of practice. Interprofessional collaboration for the successful delivery of clinical preventive services was emphasized. Recommendations were made on primary, secondary, tertiary, and quaternary prevention of musculoskeletal pain.
Conclusions:
Application of this guideline in chiropractic practice may facilitate consistent and appropriate use of screening and preventive services and foster interprofessional collaboration to promote clinical preventive services and contribute to improved public health.
Introduction
Over 30
The importance of preventing disease is indisputable. A great deal is known about disease prevention and health promotion; changing health behavior is a key approach. Between 2014 and 2018, the number of guidelines listed for disease prevention in primary care medicine doubled in the U.S. National Guideline Clearinghouse of the Agency for Healthcare Research and Quality. 2 However, providers delivered guideline-recommended preventive services to fewer than 40% of at-risk patients. 2
Interprofessional collaboration may address some of the shortfalls in health promotion and disease prevention by creating an overlap and sharing of the tasks among providers, especially for patients with multiple chronic conditions who often see several types of health professionals. 3 –5
Toward that end, this clinical practice guideline is designed to offer a practical model of interprofessional collaboration for chiropractors in the delivery of clinical preventive services—that is, services provided by health care providers that reduce risk factors and screen for early-stage disease 6 —to adult patients with musculoskeletal conditions. Utilizing the breadth of the available health care workforce, including chiropractors, would bolster at-risk patients' exposure to health promotion messages. Patients with musculoskeletal complaints are the primary patient population for the chiropractic profession. 7 They overlap with other health care providers, such as family physicians, thus increasing their exposure to health screening and counseling.
This guideline presents the spectrum of clinical preventive services as a context but focuses recommendations for services generally within the chiropractic scope of practice, which varies somewhat regionally and internationally, but generally includes non-drug, non-surgical approaches to patient care. 7 It also emphasizes the importance of practitioners developing collaborative referral networks to optimize patient care.
We also address two important barriers to the delivery of clinical preventive services: lack of time and providers' self-perceived lack of expertise in delivering preventive services.
2,8
This guideline includes a “Resource Guide,” which will be housed on the Clinical Compass (CC) website (
This project used a Delphi consensus process with a panel of health care practitioners and academicians (n = 65) to develop a clinical guideline that provided evidence-based recommendations on best practices for delivery of clinical preventive services by chiropractors and to offer practical resources to empower provider applications in practice.
Methods
The purpose of this project was to develop an evidence- and consensus-based clinical practice guideline on the role of chiropractic care in providing health promotion and clinical preventive services for adult patients with musculoskeletal pain.
The development of recommendations followed steps based on those used in previous projects
9
–12
: Establish a multidisciplinary Steering Committee (SC) with training and experience in health promotion, clinical prevention, and/or evidence-based chiropractic practice. Examine the most current clinical practice guidelines (CPGs) related to each aspect of management. Identify gaps in the CPG(s) that may form barriers to best practices. Perform targeted literature searches for the highest available evidence on the gap topics. Make recommendations on chiropractic management, based on the best available evidence. Conduct a Delphi consensus process with a panel of experienced practitioners and faculty. Gather additional feedback from a public posting of the consensus statements.
10,11
Human subjects' considerations
Before establishing the Delphi panel, the lead institution obtained Institutional Review Board approval. Delphi panelists signed an informed consent that specified that their participation was voluntary and without compensation. They were provided with a consent form after the consensus process was completed in which they agreed to be acknowledged by name in the resulting publication after we obtained their signed form.
Project SC
The SC was composed of clinicians and academicians with many years of clinical and/or research experience representing multiple health professions. Its responsibilities were to examine and evaluate the evidence; develop recommendations based on the best available evidence; revise the recommendations based on the Delphi panelists' ratings and comments to reach a consensus; and contribute to the final manuscript.
Of the 15-member SC, 13 are Doctors of Chiropractic (DCs). The two non-DCs are PhDs (one in psychology and one in health promotion). To address topic expertise, three of the members have public-health related PhDs (Preventive Medicine or Health Promotion), three are Certified Health Education Specialists, one is a certified health and wellness coach, and one has an MPH.
Professions represented, including cross-trained DCs, are chiropractic, massage therapy, medicine, nursing, psychology, public health, and health promotion education. Nine are employed at health care training institutions, three at the Veterans Health Administration as clinicians, and three in private practice. To ensure stakeholder representation, seven of the DCs on the SC are in leadership positions of the CC, a chiropractic organization that represents U.S. state chiropractic associations as well as the U.S. chiropractic colleges and other chiropractic organizations. All but two of the SC members are located in the United States; two are located in Australia.
Literature search
A health sciences librarian, working with the SC, conducted literature searches in two stages. At least two investigators independently screened articles resulting from the searches for eligibility. Disagreements were resolved by discussion.
First stage search
To identify “seed documents” on which to base development of the initial set of seed recommendations, we conducted a search to identify the most recent clinical practice guidelines for clinical preventive services. We restricted the search to articles published from 2018 to 2020, because it has been recommended that CPGs be updated approximately every 3 years. 13
Inclusion criteria for articles were:
Published January 2018–December 2020
English language
PubMed (It is unlikely that higher levels of evidence would be found in databases other than PubMed.)
Addressed non-pharmacological, non-surgical clinical preventive services in adults
Guidelines (clinical practice guidelines)
Exclusion criteria: Articles were excluded if they addressed:
Topics typically outside chiropractic scope of practice (e.g., managing specific non-musculoskeletal conditions or diseases; pharmacological preventive interventions)
Special populations (any other than non-pregnant adults)
Specific local populations or geographic areas only
Because chiropractic practice is predominantly concerned with the management of people with musculoskeletal conditions, we created search strategies for topics that might contribute to clarifying an appropriate role for chiropractic care in primary, secondary, and tertiary prevention. These were:
Health promotion and disease prevention
Diet, physical activity, and obesity management
Tobacco cessation
Immune response related to manual therapy
Lifestyle factors related to immune system support
Hygiene for infectious disease prevention related to chiropractic practice
Details of the construction of these search strategies are provided in Supplementary Data. In addition, we used reference tracking and consulted topic experts on the SC to ensure that relevant papers were not missed. We also included evidence from our previous CPG on chiropractic management of patients with chronic musculoskeletal pain, which involves tertiary prevention. 11
Second stage search
For topics on which no CPGs were identified, the search was extended to include systematic reviews and meta-analyses.
When there were gaps in or lack of detail for implementing guideline recommendations, we made additional targeted searches of specific preventive services/health promotion topics.
Evaluation of the quality of the evidence
The articles identified in our searches were then evaluated for quality. A Literature Review committee was formed to perform the evaluations. The project director developed an orientation manual for the committee members. It included a brief review of key aspects of study design and detailed notes for each evaluation instrument to standardize their application. At least two investigators rated each study and discussed differences in ratings until they reached agreement.
We evaluated CPGs by using the AGREE-Global Rating Scale (Table 1), which we have used in other studies. 11,12,14 We evaluated systematic reviews by using a modified Scottish Intercollegiate Guideline Network (SIGN) checklist, 15 which has been used in other studies (Table 2). 11,12,16 –19 The SIGN checklist rates the studies as “high quality, low risk of bias,” “acceptable quality, moderate risk of bias,” “low quality, high risk of bias,” or “unacceptable” quality. We did not assess the quality of other types of studies, simply identifying their design and categorizing them as “lower level.” Articles rated as “high” or “acceptable” quality were used as primary evidence to support recommendations; lower-level studies were used to support details to aid in implementation.
AGREE Global Rating Scale a
Brouwers et al. 14
Systematic Review/Meta-Analysis Modified SIGN Checklist
Rating: “Yes” = 1; “No” or unable to tell from the article = 0.
Scoring—sum of items as follows: 10–12 = high quality, low risk of bias; 8–9 = acceptable quality, moderate risk of bias; <8 = low quality, high risk of bias.
SIGN, Scottish Intercollegiate Guideline Network.
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system
20
to assess the overall quality of the evidence:
Grading of Recommendations Assessment, Development, and Evaluation System a
Source: GRADE Working Group. 129
Determination of Strength of Recommendations a
Seed statements development
A 2012 set of “best practices” recommendations on the role of chiropractic care in health promotion and disease prevention served as a seed document to inform the development of the seed statements for this project. 22 We also used our 2020 clinical practice guideline on chiropractic management of chronic musculoskeletal pain as a blueprint for the format of this project. 11 The content of the seed statements was based on the results of the literature search, focusing on recent relevant clinical practice guidelines and adapting their recommendations as appropriate to chiropractic scope of practice. The SC developed the seed statements, revising them for clarity and congruence with the literature, until they agreed that they were ready to be sent to the Delphi panel for rating.
Delphi consensus panel
We conducted a Delphi consensus process as per the RAND-UCLA methodology: This method “generally involves multiple rounds, in which a questionnaire is sent to a group of experts who answer the questions anonymously. The results of the survey are then tabulated and reported back to the group, and each person is asked to answer the questionnaire again. This iterative process continues until there is a convergence of opinion on the subject or no further substantial changes in the replies are elicited.”23(p. 6) We have an established, broad-based panel of DCs and other health professionals who value and are familiar with the evidence base of chiropractic and who represent both practice and academic experience. Previous projects focused on the United States, due to its specific practice parameters and reimbursement issues. However, for the current topic of health promotion and disease prevention, we expanded the panel to include international representation.
We developed the current Delphi panel by (i) inviting those who participated in our previous consensus projects and (ii) nominations by the SC of experienced practitioners from the United States and other countries. Nominees submitted a practice characteristics form and their CV for the SC to review and after approval were invited to participate. Seventy-one were invited, and 65 accepted.
Delphi process
We sent the panelists a brief summary of the project that included relevant background literature and a document orienting them to the Delphi process. All communications, and the consensus process, were conducted via email by the project coordinator. Panelists were de-identified during the rating process, to avoid possible bias.
We followed the RAND-UCLA methodology, which uses a rating scale anchored by 1 (highly inappropriate) to 9 (highly appropriate), with “uncertain” placed over the middle of the scale. 23 In keeping with this methodology, we defined “appropriateness” to mean that the expected health benefit to the patient exceeds the expected negative consequences by a sufficiently wide margin that it is worth doing, exclusive of cost. 23 If panelists rated a statement as inappropriate (rating 1–3), they were asked to state a reason and provide a citation from the peer-reviewed literature to support it, if possible. Without a specific reason, the response was considered incomplete and no number was recorded. This procedure was used to facilitate creation of an appropriate, evidence-based revision that accurately represented the panelists' input as well as the available literature.
Data management and analysis
After each Delphi round, the project coordinator entered the ratings data into an SPSS (v. 25) database, and she and the project director computed medians and percentages of agreement. To maintain the rigor of the methodology, the threshold for consensus was 80% with a median rating of at least 7. We calculated agreement by categorizing ratings of 1–3 as “inappropriate” (disagreement with the statement); 4–6 as “uncertain”, and 7–9 as “appropriate” (agreement). We sorted the panelists' comments in a Word table by panelist ID, statement number, and rating to facilitate review. The SC reviewed the ratings and the deidentified comments. The SC revised any statements that did not reach at least 80% agreement, basing the revision on both the panelists' comments and the available literature. We recirculated the revised statements, along with all comments, and repeated the process until a consensus was attained.
Stakeholder engagement and external review: public comments
In keeping with recommendations by organizations such as the AGREE Enterprise, 24 we used several means to ensure both transparency and stakeholder involvement into developing this guideline. (i) Stakeholders were included in the broad-based Delphi panel. (ii) We invited public comments on the draft CPG after the conclusion of the Delphi process.
Public comments were solicited through methods we had established in previous projects. 10,11 We used several routes to disseminate an invitation for comments on the draft CPG:
Email blast through MailChimp to the CC email list. This included the Clinical Compass Board, which includes U.S. state chiropractic organizations; a number of national chiropractic professional and academic organizations (a total of ∼900 individuals); and vendors, which included interested laypersons.
ChiroCongress, a professional organization whose member associations represent more than 35,000 chiropractors.
CC Facebook and LinkedIn pages. These are available to both health professionals and interested laypeople.
Chiropractic Summit (
These different dissemination routes overlapped to some extent, which provided reinforcement of the message. We sent a two-week reminder after the initial mailing. The comment period was 30 days.
The invitation sent to all groups contained a link to a dedicated page on the CC website. This site included several documents: (i) A repetition of the initial invitation for comments; (ii) Background and introduction to the project; (iii) Summary of the methodology, including the names and credentials of all project personnel to promote transparency; (iv) Definitions of key terms and concepts for readers who were not familiar with health promotion and disease prevention terminology; (v) The draft consensus statements; these included their references and also the percent agreement attained in the Delphi process; and finally, (vi) A user-friendly comment form to facilitate responses and instructions to email the form directly to the project coordinator. The project director and the SC reviewed and decided how to respond to each comment. In the event that comments resulted in substantive change, the revised statements were to be recirculated in an additional Delphi round(s) until a consensus was reached.
Results
Literature search
First stage search: clinical practice guidelines
Topics for which CPGs were identified were health promotion and disease prevention, diet, physical activity and obesity management, and tobacco cessation. Figure 1 shows the results of this search (2018–2020). Of 89 citations, 27 remained after screening for duplicates and eligibility (see Table 5 for list of articles). 12,25 –49 (Excluded studies are listed in Supplementary Data) We included several guidelines that were published before 2018 if there were no comparable guidelines published more recently.
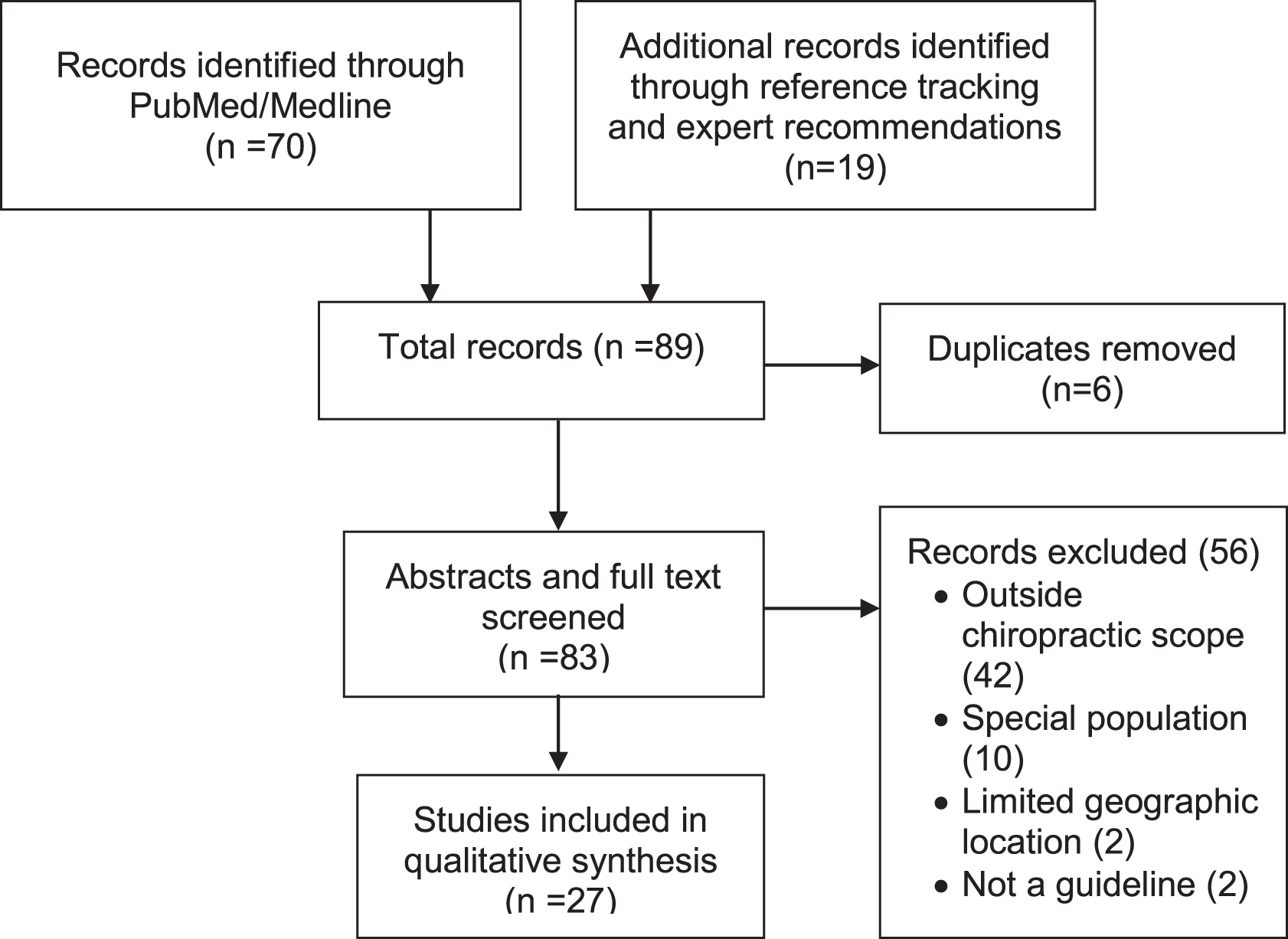
PRISMA flow diagram for clinical practice guidelines literature search. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Clinical Practice Guidelines Quality Assessment
In some cases, the first author was an individual but we have listed USPSTF because it was a set of recommendations made by USTSPF.
Quality was assessed by using the AGREE Global Rating Scale (Table 1). Based on the published methodologies for USPSTF, AHRQ, and WHO, we classified all their guidelines as high-quality.
Although the publication date is 2002, this guideline is still recommended by the Centers for Disease Control and Prevention.
This was published early in 2021 so that we were able to incorporate it although it fell outside the formal search parameters.
AHRQ, Agency for Health Care Research and Quality; MSK, musculoskeletal; RACGP, Royal Australian College of General Practitioners; USDHHS, U.S. Department of Health and Human Services; USPSTF, United States Preventive Services Task Force; WHO, World Health Organization.
Second stage search: systematic reviews
Topics for which no CPGs were identified were effects on the immune system of spinal manipulation and lifestyle factors. The search for systematic reviews yielded 112 articles, as shown in Figure 2. After screening for eligibility and relevance, eight articles remained (shown in Table 6). 50 –57 (Excluded studies are listed in Supplementary Data.)
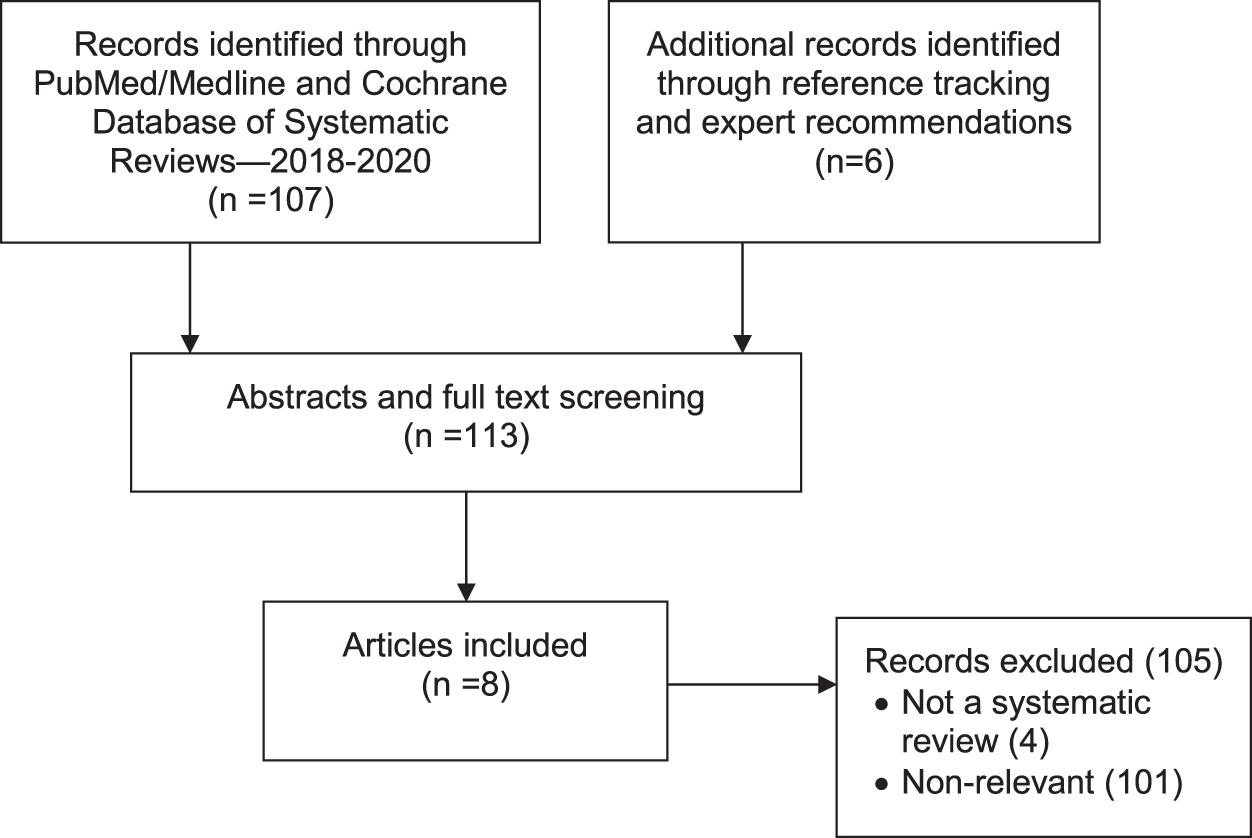
PRISMA flow diagram for second-stage literature search including only systematic reviews.
Systematic Review Quality Assessment
Quality was assessed by using a modified SIGN checklist (see Table 2).
Published early in 2021 so that we were able to incorporate although outside the formal search parameters.
Quality assessment
These 27 CPGs were all rated as high or acceptable. Table 5 lists the articles and quality rating for each. 12,25 –49,58 The eight systematic reviews were all rated as high quality. Table 6 lists the articles and quality rating for each. 50 –57
Table 7 displays the rating of the quality of evidence and strength of recommendations for general topics. For screening and counseling on health behavior, infection control procedures for ambulatory care, and chiropractic management of tertiary prevention of pain, the evidence was strong, and there were no factors to lessen the strength of the recommendations in favor of these. For the effect of physical activity and environmental risk factors on the immune system, evidence was less robust, but because there are a few risks and multiple benefits of these, the recommendation in favor is strong.
Quality of Evidence and Strength of Recommendations for Specific Topics
Quality of evidence uses GRADE classifications (see Table 3 for details): A = high; B = moderate; C = low; D = very low.
SoR = Strength of recommendation; uses GRADE classifications: ↑↑ = Strong recommendation in favor of the intervention; ↑ = Weak recommendation in favor of the intervention; ↓↓ = Strong recommendation against the intervention.
For the effects of spinal manipulation on immune function, systematic reviews were high quality. However, the evidence they evaluated was low level and based on non-clinical studies. The strength of our recommendations varied. Although there is a low risk of side effects, the low-level evidence is outweighed by the possible delay or avoidance of interventions with more substantial evidence.
Public comments
After the 30-day public comment period, three comments were received. All were from chiropractors (one each from Florida, Oregon, and Australia). They were supportive of the project but wanted more details to be included about examinations and nutritional recommendations. Because of the defined scope of the project, the SC did not consider these comments to affect the validity of the consensus statements.
Delphi panel characteristics
The final panel composed of 65 individuals represented 6 health professions (acupuncture, chiropractic care, medicine, mental health counseling, nursing, and physical therapy). The distribution of professions was 94% DC, 3% MD, and 3% PT. The other professions listed were dual-trained DCs. The panelists were primarily male (78%) and Caucasian (85%). Other races/ethnicities reported were: other, unspecified (3), Hispanic (2), Asian/Pacific Islander (1), Black/African American (1), East Indian (1), Multiracial (1), and one missing response.
Delphi process
The list of key terms and concepts was provided to the panelists to be read before they began rating the statements, to be sure they were making decisions based on common terminology.
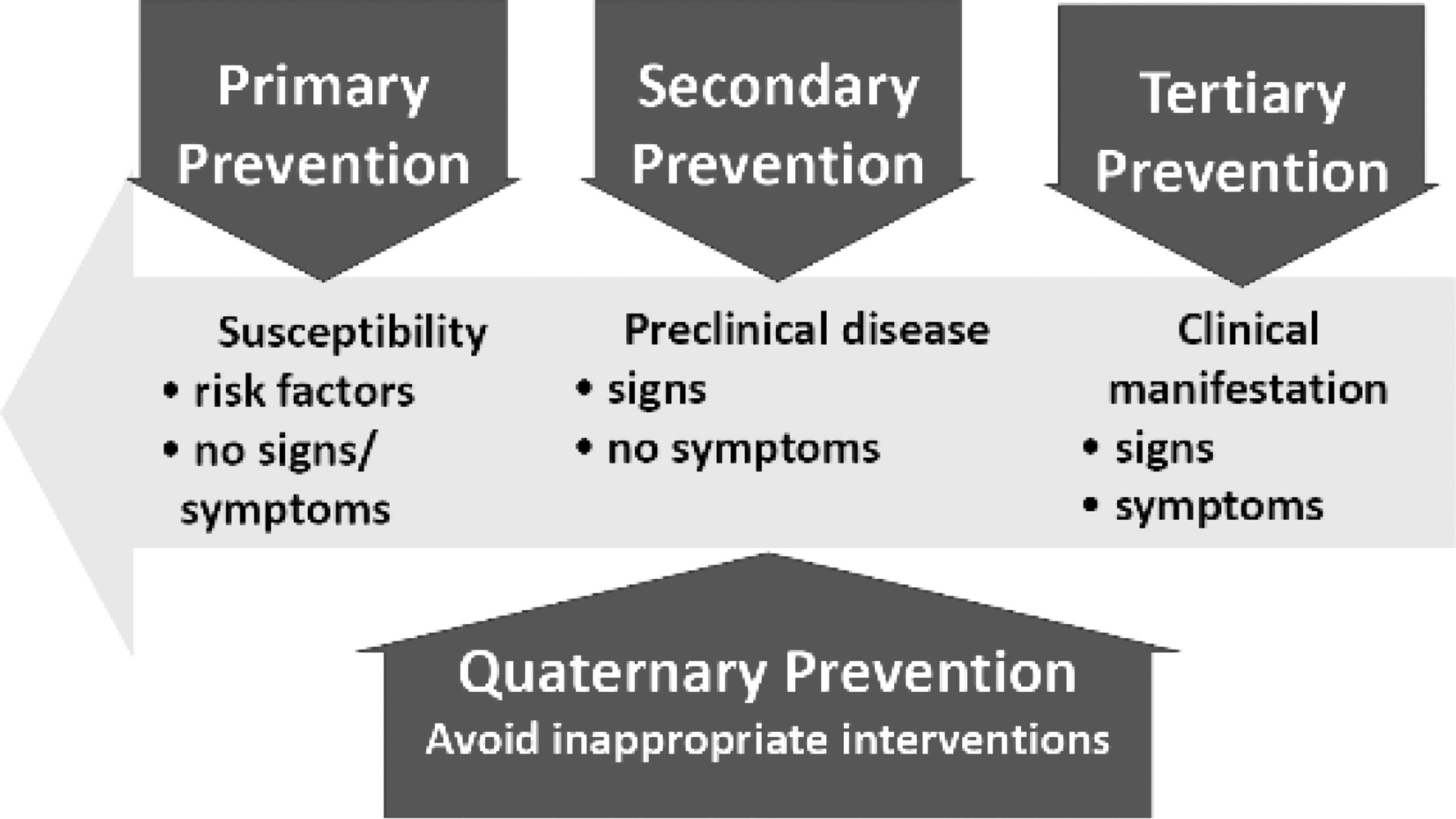
Levels of prevention.
Primary: remove the cause or risk factors for a condition/disease before it occurs
Secondary: detect a condition/disease at an early stage and reduce or prevent long-term effects (e.g., screening)
Tertiary: reduce the chronic effects of a condition/disease, minimizing sequelae (e.g., rehabilitation)
Quaternary: protect individuals from health care “interventions that are likely to cause more harm than good”60(p. 106)
Primary prevention of pain: prevention of acute pain (example: injury prevention)
Secondary prevention of pain: prevention of transition of acute to chronic pain
Tertiary prevention of pain: reducing the effect of chronic pain on health and health-related quality of life.
There were 60 statements for the panelists to rate in the first Delphi round. All 65 panelists responded to all Delphi rounds. All but two statements reached at least 80% consensus. Both statements were revised as per the comments and based on the evidence. One statement reached a consensus in Round 2 after being revised. The other required a third round and was rewritten as three statements before reaching a consensus. The following statements are the final product of the Delphi process.
Consensus Recommendations
Recommendations for general topics on health promotion and clinical prevention
Clinical preventive services, which include screening and counseling on health promotion and disease prevention, contribute to reducing current epidemic levels of chronic disease, chronic pain, obesity, and opioid use. 6
Specific health behaviors are risk factors for most chronic conditions for which people seek health care. 6
It is the responsibility of health care providers to identify these risk factors and facilitate health behavior change through providing appropriate evidence-based interventions or access to resources for such interventions. 6,65,66
A biopsychosocial model is most appropriate for health promotion and disease prevention, particularly for typical chiropractic patients who present with chronic musculoskeletal pain and comorbidities/risk factors such as obesity, diabetes, cardiovascular disease, and other chronic conditions. 44,67
Interprofessional collaboration contributes to the successful delivery of clinical preventive services. 3 –5
Within their regulated scope of practice, chiropractors, similar to other health professionals, should follow established best-practice guidelines for disease prevention and health promotion, such as those recommended by the United States Preventive Services Task Force (USPSTF) and other recognized authorities. 11,22,68
Use health promotion counseling strategies established for use in primary care settings that can be delivered as brief interventions (3–10 min, which may be spread over multiple visits) to facilitate health behavior change in patients with risk factors for or presence of chronic disease. Emphasize key principles 8 :
To encourage willing collaboration between patient and provider and gauge patient readiness to change, ask the patient for permission to discuss a behavioral issue directly related to the presenting complaint. 8
Provide necessary information appropriate to the patient's level of health literacy.
Mutually agree on a specific behavior change, emphasizing its importance to the individual.
Provide readily accessed resources (ehealth/mhealth or conventional) so the patient can immediately take action. 62,64,69
Follow up at subsequent visits with brief questions and encouragement.
Address patients' cultural values as appropriate within the context of the specific health care topic on which you are counseling them. If these are not known, respectfully ask about their health beliefs and customs. 25
Informed consent, risks, and benefits
Chiropractic management should be consistent with the principles of evidence-based practice, which depend on: (i) the best available published scientific evidence combined with (ii) the clinician's experience and expertise and (iii) the patient's preferences and values. 12
Inform the patient about any serious potential risks and costs as well as the possible benefits of a proposed intervention.
The informed consent process involves active provider–patient communication. Explain all procedures, including diagnostic and treatment options (including no treatment and the natural history of spinal pain), in terms that are appropriate for the patient's level of health literacy. 11,70 After answering the patient's questions and obtaining their signature, enter the informed consent into the health record.
Assess the patient for possible contraindications to manipulation or other procedures, particularly high-velocity, low-amplitude “thrust” maneuvers. 11,12,45
Chiropractic-specific health promotion and disease prevention model
Health promotion and disease prevention in chiropractic care should be based on a biopsychosocial model encouraging patient empowerment and engagement in self-care practices. 22,67
Clinical preventive services within the chiropractic scope of practice are congruent with those of other providers and emphasize the following three components 22,37 :
Screening for risk factors for disease, particularly lifestyle-related risk factors such as tobacco use, lack of physical activity, poor diet, and obesity.
Evidence-based health behavior counseling to promote health and prevent disease and injury, placing an emphasis on physical activity, dietary, and lifestyle factors that promote optimal function.
Manual procedures, including spinal manipulation, to enhance the patient's ability to engage in an active lifestyle. 11
The phases of prevention for chiropractic management of musculoskeletal pain may be appropriately applied as follows:
Primary prevention of pain: Chiropractic management that includes counseling on exercises or safety measures to decrease the risk of acute injury addresses primary prevention of pain. 61 However, clinical evidence does not currently exist to support the use of spinal manipulation alone for direct primary prevention of any condition or disease. 53
Secondary prevention of pain: Chiropractic management that includes spinal manipulation, lifestyle counseling and other non-pharmaceutical approaches may contribute to secondary prevention of pain by shortening the duration of acute pain but little evidence supports spinal manipulation alone in preventing the transition from acute to chronic pain. 47,61,71
Tertiary prevention of pain: Substantial evidence supports chiropractic management that includes spinal manipulation, lifestyle counseling, and other non-pharmaceutical approaches for tertiary prevention of pain. 11,72 –75
Recommendations for primary prevention of disease and disability
Overall screening and counseling
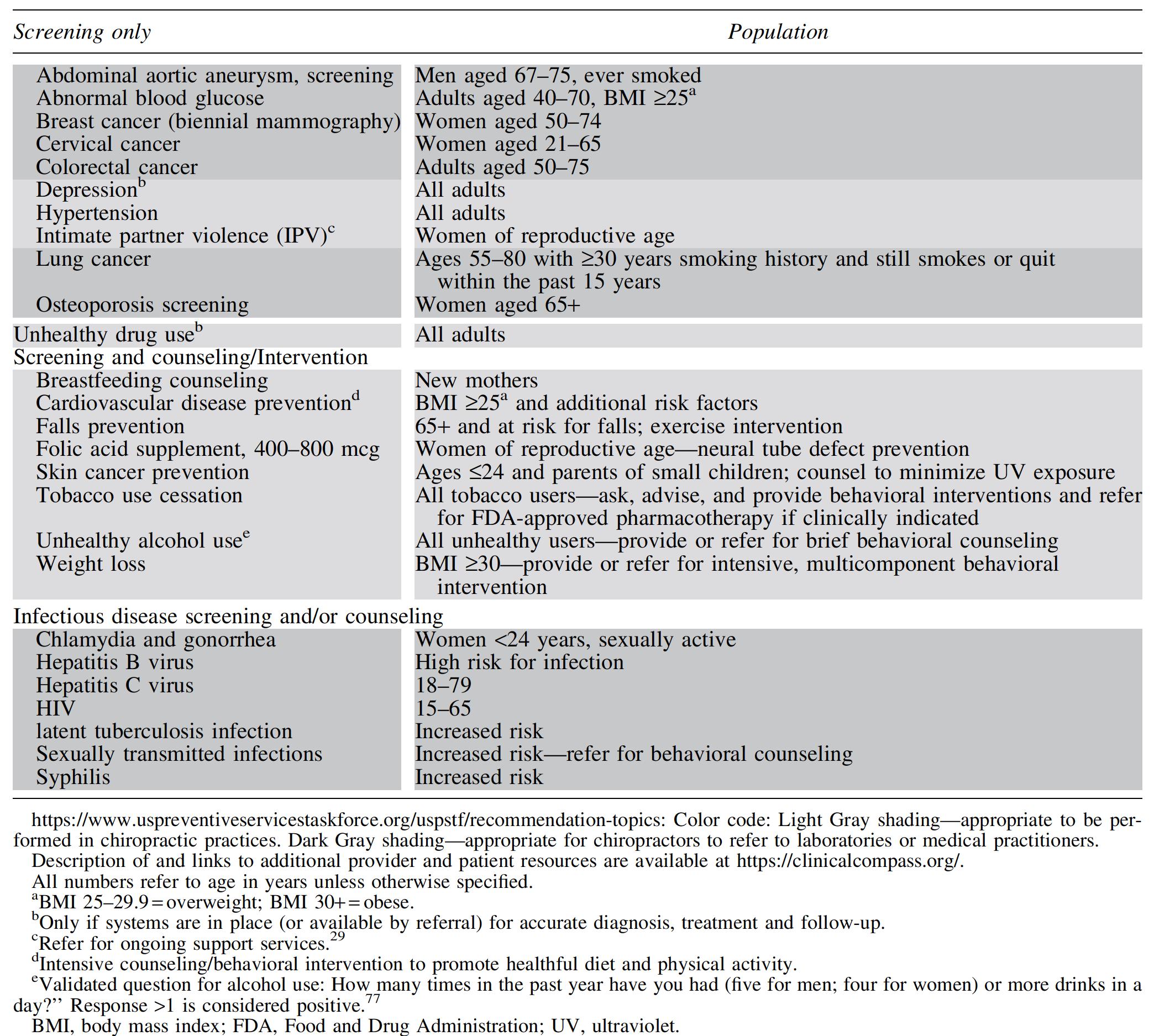
Tobacco use, obesity, poor diet, and physical inactivity are key risk factors for chronic disease that are of paramount importance to the health of the public. Like all health care providers, DCs should screen for these risk factors and provide or refer for evidence-based resources and/or counseling. 22,37 Table 8 summarizes all screening and counseling recommendations of the USPSTF. 29,37,76 –78
Clinical Preventive Services Recommendations for Nonpregnant Adults, Based on A- or B-Level Rating from United States Preventive Services Task Force
Tobacco cessation
Determine the tobacco use status of all adolescent and adult patients and record it in the health record. 41
Offer tobacco users information and/or resources for cessation. At a minimum, offer him or her the national quit line number (U.S. 800-QUIT-NOW).
Offer patients readily accessed online cessation resources.
Base tobacco cessation counseling on the Ask, Advise, and Refer or 5 A's (Ask, Advise, Agree, Assist, Arrange) approach. 37,49,79
Weight management
Identify patients who are overweight or obese and ask permission to initiate a health-focused and person-centered discussion with them. 28,38
Overweight patients with weight-related conditions (such as diabetes) and obese patients should be provided with a lifestyle program that includes (i) reducing calories; (ii) increasing physical activity; and (iii) interventions to support behavioral change. 37,38,80
Provide patients with individualized follow-up feedback by using technology-based strategies. 38,62 –64,81
Nutrition/diet
Make nutrition recommendations for adults of all body sizes personally and culturally acceptable and affordable to the patient as well as nutritionally adequate to support long-term adherence. 38,82
Advise patients with risk factors for chronic disease or presence of chronic disease to adopt a diet emphasizing vegetables, fruits, whole grains, and unprocessed food and minimizing added sugar and salt. 32,58
Physical activity
Advise currently sedentary patients to reduce sitting time and increase moderate-to-vigorous physical activity. 40,83 –86
Screening and Advising on Exercise Participation for Currently Sedentary Adult Patients a
Riebe et al. 35
CV, cardiovascular.
Injury prevention
Fall prevention for older adults
Advise older adults on balance, strength, and endurance exercises for fall prevention. 31,76,87 –89
There is limited evidence directly supporting manual therapy to improve balance in older adults. 90,91 However, spinal manipulation is supported for reducing chronic musculoskeletal pain and cervicogenic dizziness. 92,93 In the presence of these conditions, a multimodal approach that includes spinal manipulation combined with an appropriate exercise regimen 76,88 and resources for patients to correct home hazards 94 may be supportive to older adults at risk for falls.
Suicide prevention
Because chronic pain and opioid use are among a group of important risk factors for suicide, 95 –97 establish and maintain a list of qualified counselors experienced in suicide risk assessment and/or treatment for at-risk patients.
Maintain readily accessible community resources for suicide prevention, such as the National Suicide Prevention Lifeline.
Firearm safety
Infection control
Immunization is a well-established medical approach to primary prevention. Because it is not within the chiropractic scope of practice, refer patients who ask about vaccines to authoritative, evidence-based resources. 22
No definitive clinical evidence supports a protective effect of spinal manipulation on immune system function or infectious disease prophylaxis. 52,53,56
Provide office and clinical staff with an infection control protocol with training on hand hygiene, personal protective equipment, and environmental (surface) cleaning to prevent infection, consistent with evidence-based international or national guidelines such as those provided by the World Health Organization. 26,99
Base advice to patients on infectious disease, particularly COVID-19, on evidence-based international or national public health guidelines. 99
Risk factor reduction, particularly increased physical activity, tobacco use cessation, achieving and maintaining a healthy weight, healthy food choices, and stress management may have a supportive effect on the immune system. 50,51,54,55,57
Recommendations for secondary prevention of disease and disability
Provide patients with evidence-based screening procedures within the chiropractic scope of practice, such as the priority USPSTF-recommended procedures shown in Table 1. 100
Develop a referral network of appropriate primary care and specialist practitioners for recommended screening procedures outside the scope of chiropractic practice. 100
During routine physical inspection of the body, note the presence of any skin lesions that appear atypical according to the ABCDEs inspection (
Recommendations for tertiary prevention of disease and disability
Spine-related chronic pain
Patients' chronic musculoskeletal pain should not be expected to be “cured” within a specified time interval and/or number of treatment visits. Maintaining pain and function at optimal levels may be facilitated by planned treatment visits to prevent relapses and recurrences. 11,102 –105
The goal of pain management is to facilitate the patient's ability to function optimally. This requires engaging the patient in self-care and lifestyle modifications to avoid physician dependence.
Consider multiple approaches that include both active and passive interventions as well as both physical and mind–body interventions. 11
Active interventions for spine-related chronic pain include 11 :
Rehabilitation exercise, including strengthening and flexibility
Decrease amount of time spent sitting
Weight management for obese patients
Tobacco cessation for users
Walking or other moderate aerobic exercise
Yoga and qigong
Passive interventions should be focused on assisting the patient to become more active 11 :
Spinal manipulation/mobilization
Massage
Acupuncture
Low-level laser therapy
Electrotherapies: Transcutaneous Electrical Nerve Stimulation or interferential current to manage pain and assist patients in becoming active.
Mind–body approaches: Offer resources (online or by referral) for Cognitive-Behavioral Therapy and Mindfulness-Based Stress Reduction. 11
Osteoarthritis
Active physical interventions for osteoarthritis include:
Exercise to support both achieving and maintaining healthy weight and for fitness, strength, and flexibility. 46,48
Decrease sedentary time.
Multifactorial weight management if overweight or obese. 46,48,106
Passive physical interventions include 48 :
Manual therapy, including manipulation, mobilization, and/or massage 107 –110
Acupuncture, using “high dose” (greater treatment frequency, at least 3 × week) 111,112
Mind–body approaches 46,48 : Offer resources (online or by referral) for mind–body interventions, such as Cognitive-Behavioral Therapy and Mindfulness-Based Stress Reduction.
Quaternary prevention of disease and disability
For older patients with spinal pain, provide spinal manipulation to reduce use of opioid analgesic therapy. 65,66,115 –119
For adults with low back pain, provide chiropractic care to reduce risk of outpatient adverse drug events. 120
For adults with work-related back injuries, provide chiropractic care when appropriate to reduce likelihood of back surgery. 121
For older adults with spinal pain and no red flags, chiropractic care, including spinal manipulation, may be provided without imaging. 122 –124
Take a thorough health history on all patients, including opioid and other medication use. Because the unintended consequences of opioid analgesic therapy may complicate patient care, DCs should work closely with the medical physicians of patients using opioids to ensure appropriate clinical management and reduce risk of adverse drug events. It is outside the chiropractic scope of practice in most locations to advise patients to discontinue use of prescription medications, including opioids, so it is important to collaborate with patients' providers with prescriptive authority to support reduction of opioid use. 65,74
Discussion
Previous studies show that chiropractors already advise patients on preventive health behavior. According to the 2020 Practice Analysis by the United States National Board of Chiropractic Examiners, 60% of DCs report making specific recommendations to patients on changing health behavior at least once a day and 68% make recommendations on disease prevention and early screening at least weekly. 7
An analysis of U.S. National Health Interview Survey (NHIS) data indicated that for people who sought spinal manipulation as a part of complementary and alternative medical care in 2012, more than 40% reported using this care as a wellness or preventive measure. Eleven percent stated they used manipulation to improve immune function. 125 Further, another NHIS analysis found that a large majority (88%) of patients reported that they complied with health promotion advice, either from a DC or an MD. 126 Therefore, it is important to ensure that chiropractors are providing recommendations that are consistent with national and international evidence-based standards.
The volume of evidence available to clinicians presents a significant challenge, because it is not feasible for busy clinicians to routinely review primary research literature. 127 Guidelines may be considered “a convenient way of packaging evidence and presenting recommendations to healthcare decision-makers.” 128 To further narrow the gap between recommendations and clinical implementation, we will augment this CPG by providing a Resource Guide with tools for common methods of implementation of preventive services. Further, because the nature of chiropractic practice requires a number of visits, particularly for patients with chronic conditions, chiropractors have multiple opportunities to deliver health promotion messages.
A limitation of this guideline is that for certain practices, such as spinal manipulation, evidence is scarce to make recommendations regarding its use for any purpose other than addressing tertiary and perhaps secondary prevention of pain. Another limitation is that, although we included some input from countries other than the United States, and based some recommendations on international guidelines, these recommendations primarily address U.S. stakeholders. We did achieve broad representation of these stakeholders, however, through the SC, the Delphi panel, and the wide dissemination to the public. Another limitation is that, despite making the draft document widely available, we received very few responses from the public and none from professional organizations.
We have produced this consensus guideline not to create a set of prescriptive rules, but rather to develop a resource to assist practitioners in their implementation of best practices. The CPGs are a guide, not a rulebook. The application of evidence-based guidelines must always be contextualized within the best interests of each individual patient and the experience and expertise of the practitioner 70 along with feasibility and availability. 4,65
Conclusions
Application of this guideline in chiropractic practice may facilitate consistent and appropriate use of screening and preventive services and foster interprofessional collaboration to promote clinical preventive services and contribute to improved public health.
Footnotes
Acknowledgments
The authors thank Cathy Evans for her exceptional coordination of the consensus process and achieving the high response rate. They also thank the Delphi panelists for their essential role in the development of these recommendations: Wayne Bennett, DC, DABCO; Craig Benton, DC; Charles L. Blum, DC; Gina M. Bonavito-Larragoite, DC, FIAMA; Michael S. Calhoun, DC, DACBSP; Wayne H. Carr, DC, ACRB, CCSP, AFMCP; Jeffrey R. Cates, DC, MS; Kelsey L. Corcoran, DC; Matthew Coté, DC, MS; Thomas R. Cotter, DC, DACRB; Monica Curruchich, DC RN-BSN; John Curtin, MSS, DC, IANM; Vincent DeBono, DC; Mark D. Dehen, DC, FICC; Paul Ettlinger, DC; James E. Eubanks, MD, DC, MS; Jason T. Evans, DC, DIBCN, FIACN, ABIME, NASM; Drew Fogg, DC, MS, DACRB, Cert. MDT; David Folweiler, DC, DACRB; Margaret M. Freihaut, DC; Bill Gallagher, Jr., DC; Brian J. Gleberzon, DC, MHs; Jason Guben, BSc(N),DC; Gary Alan Jacob, DC, Lac, MPH; Brian L. James, MD; Jeffrey M. Johnson, DC; Valerie Johnson, DC, DABCI, DACBN; Louis A. Kazal, Jr., MD, FAAFP; Yasmeen Khan, DC, MS, MA; Robert E. Klein, DC, FACO; Charmaine Maria Korporaal, M Tech. (Chiropractic), CCSP, CCFC, ICSSD; Rick Louis LaMarche, DC; Lawrence Jason Larragoite, DC, FIAMA, CFMP; Robert A. Leach, DC, MS, MCHES; Duane T. Lowe, DC; Eric Luke, DC, MS; Peter McCann, MAppSc, BAppSc, DAppSc, FASLM, MACA, MANTA; Peter J. McGlynn, BAppSc (Chiropractic), MPH, PhD; Ralph C. Magnuson, DPT; Hans W. Mohrbeck, DC; Scott A. Mooring, DC, CCSP; Mark Mulak, DC, MBA, MS, DACRB; Marcus Nynas, DC, FICC; Juli Olson, DC, DACM; Colette Peabody, MS, DC; Mariangela Penna, DC; Tamara Glen Pooke, M Tech (Chiropractic), South Africa, PhD Radiology, Malaysia; Morgan R. Price, DC; Ranen Rambrij, M Tech (Chiropractic); Jeffrey W. Remsburg, DC, MS, DACRB; Vern A. Saboe, Jr. DC, FACO; Bruce Scott, DC; Chris Sherman, DC, MPH; Scott M. Siegel, DC, FIAMA; Charles Simpson, DC; Albert Stabile, Jr., DC; Neil Stakes, M Chiro, Singapore, SDCA, CKTP, FAKTR; Kevin Stemple, PT; James P. Stupak, DC; Lisa Thomson, DC; Jason Weber, DC, DACRB; Susan Wenberg, DC, MA; John S. Weyand, DC, DABCO; Clint J. Williamson, DC; and Morgan Young, DC.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The NCMIC Foundation provided partial funding for the project director; the Clinical Compass provided funding for the project coordinator.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.