
Abstract
Objectives:
The aim of this study was to establish a quantitative syndrome differentiation model with logistic regression analysis for phlegm and blood stasis syndrome (PBSS) in coronary heart disease (CHD) to offer methodology guidance for the quantitative syndrome differentiation of Traditional Chinese Medicine (TCM).
Design:
Tongue, face, and pulse information of each subject was obtained using the TCM-intelligent diagnosis instruments. Logistic regression model was used to construct the syndrome diagnosis model. The area under receiver operating characteristic curve (ROC-AUC) was used to evaluate the diagnostic value of the model.
Subjects:
Among the 141 subjects, 83 belonged to the PBSS group, and 58 belonged to the non-PBSS group.
Results:
The independent indexes used to predict PBSS in patients with CHD were length of the crack (LC) (p = 0.002), number of ecchymosis (NE) (p < 0.001), length of philtrum (LEP) (p = 0.022), and right hand pulse h1 (Rh1) (p = 0.021). The expression of combining predictor L in this study was L = LC +57.58 NE +4.53 LEP +2.68 Rh1. The ROC curve analysis indicated that the AUC values of LC, NE, LEP, and Rh1 were 0.646, 0.710, 0.619, and 0.613, respectively. The AUC = 0.825 of the syndrome diagnosis model was the largest.
Conclusions:
The quantitative study of TCM syndrome based on logistic regression analysis provides a good method for the objective analysis and application of TCM syndrome.
Introduction
Coronary heart disease (CHD) is a crucial part of cardiovascular disease, and remains the worldwide leading cause of death and disability. 1 –5 CHD has become a major public health problem, bringing great burden to the society and medical treatment. 6,7 With the increasing mortality of CHD in China, improving the level of prevention and treatment of CHD has become particularly important. 8
CHD is one of the dominant diseases of Traditional Chinese Medicine (TCM), accumulating for over 2000 years of treatment practice. 9,10 TCM has unique advantages in the treatment of CHD and exhibits favorable effectiveness. 11 Syndrome is the core of TCM treatment, and syndrome differentiation is the premise of the treatment. Recent studies on TCM syndromes of CHD show that phlegm and blood stasis syndrome (PBSS) accounts for an increasing proportion of CHD syndromes. 12 –14 However, syndrome differentiation of TCM mainly depends on the subjective judgment of doctors, thereby lacking objective, unified, and quantitative diagnostic criteria, resulting in adverse factors for clinical standardized diagnosis and treatment.
Tongue, face, and pulse diagnoses are keys for TCM syndrome differentiation. With the development of modern science and technology, the diagnostic instruments of tongue, face, and pulse have been applied, leading to the realization of the digitization and quantification of the typical tongue, face, and pulse information of TCM syndrome, and promoting the transformation of TCM syndrome differentiation from empirical medicine to objectification and quantification. 15,16
Over the years, the objective research on the tongue, face, and pulse diagnosis of the syndrome differentiation of CHD has increased. Cong et al. 17,18 used digital tongue, face, and pulse acquisition instruments to analyze the tongue and facial image characteristic parameters of PBSS in patients with CHD to provide an objective reference for clinical syndrome differentiation. However, at present, the limitation of these studies is that there are many quantitative indexes collected, making the key points of syndrome differentiation complex and not conducive to clinical application.
Multivariate statistics is a mathematical statistical method for the quantitative analysis of the complex relationships between multiple variables, which has great value for the diagnosis and differential diagnosis of TCM syndromes. 19 It is an important means to realize the quantification and standardization of TCM syndromes. Logistic regression analysis, a multivariate statistical method, is widely used in multivariate modeling and the quantitative study of TCM syndromes. 20
Therefore, in this study, PBSS in patients with CHD was considered as the study subject, and TCM-intelligent diagnosis instruments (TCM-IDIs) were applied to collect tongue, face, and pulse indexes. Then, logistic regression analysis modeling was used to study the quantitative diagnosis model of PBSS in CHD. Based on the TCM theory, this study attempts to establish a quantitative model of TCM syndrome differentiation, and explores a new method for the quantitative analysis and evaluation of TCM syndromes. A flow chart of this study is presented in Figure 1.
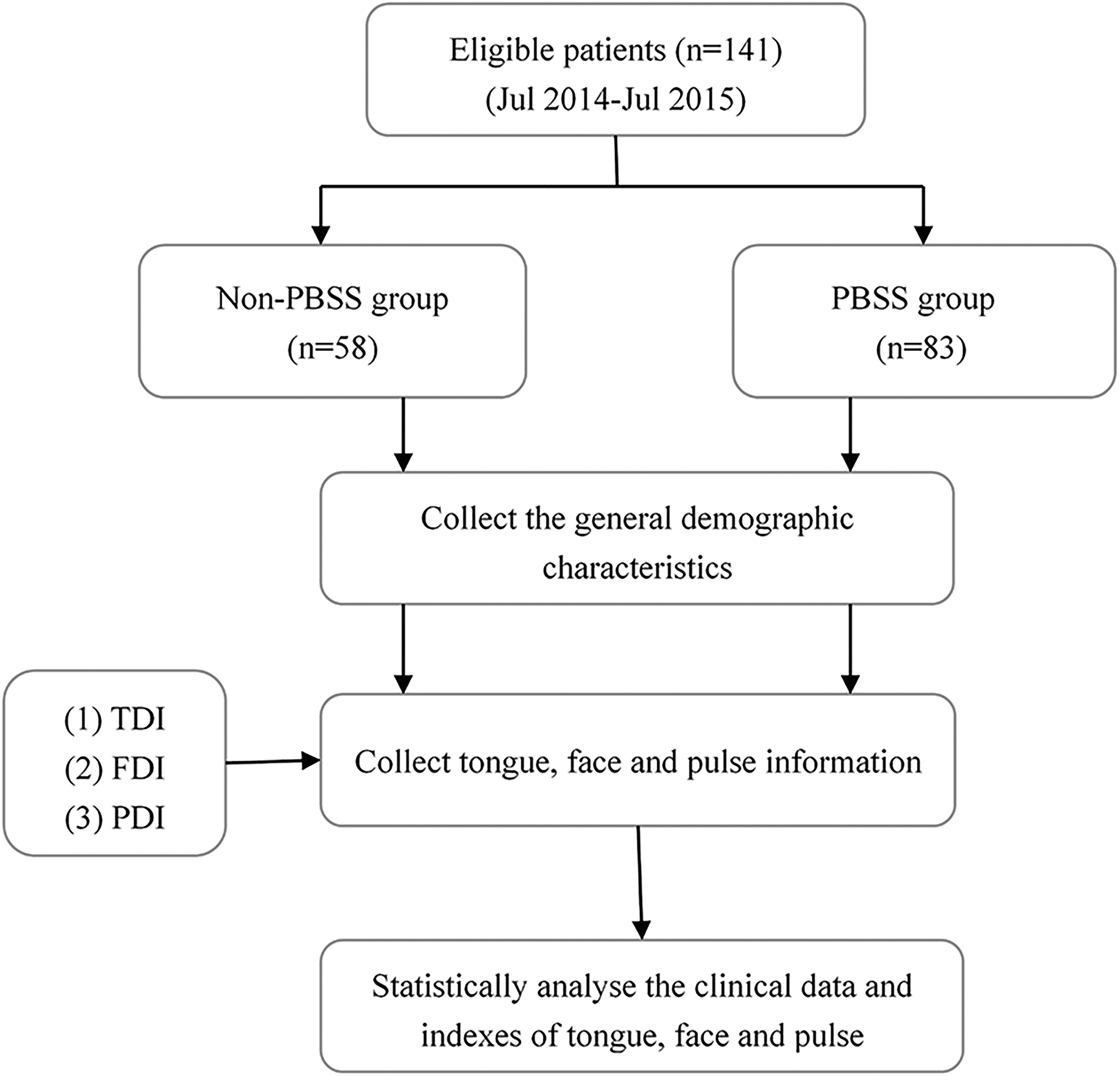
Study flow chart. FDI, Face Diagnosis Instrument; PDI, Pulse Diagnosis Instrument; TDI, Tongue Diagnosis Instrument.
Materials and Methods
Diagnostic criteria for the PBSS in CHD
Diagnostic criteria of Western medicine for CHD were based on the 2016 American College of Cardiology/American Heart Association guideline focusing on updates on the duration of dual antiplatelet therapy in patients with coronary artery disease, 21 and Chinese guideline for the diagnosis and treatment of patients with chronic stable angina published in 2007. 22
The diagnostic criteria of PBSS in CHD were based on the authors' previous research 23 and used as the “gold standard” for this study. The details are provided as follows: oppression in the chest or chest pain, obesity or head and body trapped, purple or dark tongue, petechia or ecchymosis of tongue, greasy coating, darkish or dim complexion, and string-like and slippery pulse. Moreover, the differentiation of other TCM syndromes except PBSS in CHD referred to the Guiding principles for clinical research of new Chinese medicine. 24
In this study, TCM syndrome differentiation was conducted by two TCM experts. If both experts agreed that the CHD patient had PBSS, the patient was included in the PBSS group; in contrast, if they both disagreed, the patient was included in the non-PBSS group. If experts had different opinions, grouping was decided by the independent diagnosis of a third expert. All of the three experts met the following criteria: (1) specialized in therapy of TCM or integrative Chinese and Western medicines on cardiovascular medicine; (2) had senior (high or vice-high) professional title; and (3) had worked in cardiovascular department for >20 years.
Subjects
From July 2014 to July 2015, patients diagnosed with CHD were recruited from Baokang Hospital of Tianjin University of Traditional Chinese Medicine and Wuqing Hospital of Traditional Chinese Medicine in Tianjin City. Before any study-related procedures, all subjects submitted individual consents. Inclusion criteria for patients with PBSS in CHD were as follows: (1) met the diagnostic criteria for CHD and PBSS in CHD; (2) >18 years old; and (3) voluntarily participated with a signed informed consent. Exclusion criteria were as follows: (1) acute episodes of myocardial infarction, heart failure, cerebral infarction, and cerebral hemorrhage; (2) severe primary diseases, such as liver, renal insufficiency, blood system diseases, and malignant tumor; (3) pregnant or lactating women; and (4) psychiatry, dementia, and other similar conditions that cause inability to cooperate.
Ethics
This study was approved by Medical Ethics Committee of Tianjin University of Traditional Chinese Medicine (No. TJUTCM-EC20150004) and conducted according to the Declaration of Helsinki.
TCM-IDI system
The YM-III Series TCM-IDIs were jointly developed by Tianjin University of Traditional Chinese Medicine, Tianjin University, and Tianjin Tianzhong Yimai Technology Development Co. Ltd. The instruments have been validated by clinical trials and have obtained the Registration Certificate for Medical Device (Supplementary Figs. S1 and S2).
Tongue and face diagnostic instruments (TDI and FDI, Registration No. 20152270135), sharing a set of hardware systems, collected tongue and face images, and their corresponding software systems conducted digital analysis of these images, respectively; meanwhile, the Pulse Diagnosis Instrument (PDI, Registration No. 20152270070) software system converted the radial artery pulse signals acquired by the hardware system into the corresponding pulse waveform (Fig. 2). More details about TCM-IDIs are provided in the Introduction of Traditional Chinese Medicine-intelligent diagnosis instruments section of Supplementary Data.
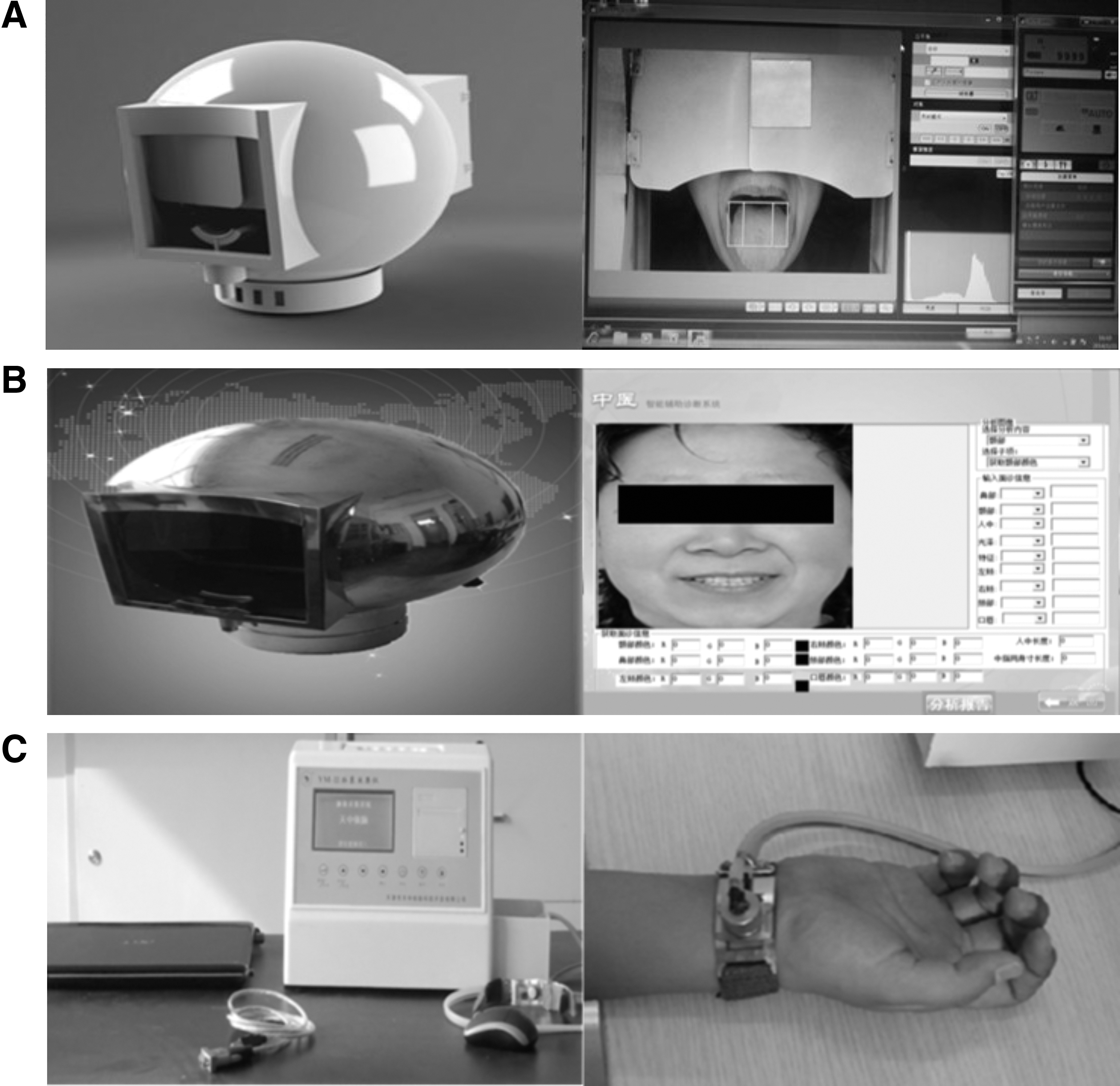
TCM-IDIs.
In the clinical diagnosis of TCM, tongue diagnosis mainly examined its color and coating, facial diagnosis mainly examined the cheek and lip, and pulse diagnosis mainly examined pulse pressure, pulse rate, and rhythm; these related indexes were collected by using TDI, FDI, and PDI (Table 1). All indexes were observed by two researchers who are qualified practicing physicians of TCM. Finally, these indexes were analyzed through consultation with two TCM practitioners.
Indexes of Tongue, Face, and Pulse Diagnoses Measured by the Traditional Chinese Medicine-Intelligent Diagnosis Instruments
FDI, Face Diagnosis Instrument; TDI, Tongue Diagnosis Instrument; PDI, Pulse Diagnosis Instrument.
Study procedure
First, basic information such as age, gender, number of chest pain episodes, nitroglycerin consumption, chest pain duration, and body mass index (BMI) was collected. Then, syndrome information such as tongue, face, and pulse of each eligible subject was collected.
Tongue image collection: the subjects were seated in front of the TDI, their mandible was placed on the mandibular bracket, and the tongue was extended out of the mouth naturally in a relaxed manner to fully expose the tongue body. Then, tongue images were collected quickly, especially when the tongue reached the optimum state.
Facial images collection: the subjects took the right seat, the face was positioned fully in the acquisition interface, and then facial images were collected. The images of tongue and face of typical CHD with PBSS are provided in Supplementary Figures S3 and S4.
Pulse diagnosis information collection: after 10 min of rest, each subject was asked to sit comfortably and put their forearms at the same level as their hearts. The pulse sensor was fixed at the radial pulse of the wrist after the instrument was debugged and stabilized. The pulse sensors detected the radial pulse of both arms. The subjects maintained their forearms and elbows relaxed. After the pulse waveform was clear and stable, the values were recorded. Finally, the indexes of tongue, face, and pulse were processed and analyzed by the corresponding software systems.
Colors are expressed in RGB color space to accurately describe the colors. The meaning of pulse index was based on the “Modern Chinese Medicine Pulse Diagnosis” written by Zhaofu of China. 25
Statistical analysis
All the statistical analyses were performed using the SPSS (version 22.0). The normality and equality of measurement indexes were assessed by the Kolmogorov–Smirnov test. Data are expressed as mean ± standard deviation (SD) for normally distributed variables, and as media and range for non-normally distributed variables. Continuous variables were tested by Student's t-test or the Mann–Whitney U test, and categorical variables were tested by χ 2 test.
The correlation between indexes and PBSS of CHD was accessed by binary logistic regression analysis. For univariate logistic regression analysis, the “Enter” method was used. Candidate variables with p < 0.1 on univariate analysis were included in multivariate logistic regression, which used a forward stepwise (likelihood ratio) approach. Only variables that remained significant at the 0.05 level (two sided) were included in the multivariate logistic regression for subsequent analysis.
Using the above binary logistic regression analysis, the combining predictor L of tongue, face, and pulse indexes was constructed; that is, a multiple-index syndrome diagnosis model was built suitable for this study. The receiver operating characteristic (ROC) curves of combining predictor L and significant indexes analyzed by multivariate logistical regression were drawn, and the area (area under ROC curve [ROC-AUC]) was calculated. According to the maximum principle of the Youden Index, the cutoff values of combining predictor L and significant indexes were determined to predict PBSS in CHD, and their sensitivity and specificity were calculated. p < 0.05 was considered statistically significant.
Results
Demographic data and indexes of tongue, face, and pulse
The detailed characteristics and measured indexes of the subjects are shown in Tables 2 and 3. The study was composed of 141 patients (83 patients with PBSS and 58 without PBSS). The PBSS group included 39 females (46.99%) and 44 males (53.01%), with a mean age of 63.29 ± 10.02 years, whereas the non-PBSS group included 32 females (55.17%) and 26 males (44.83%), with a mean age of 61.86 ± 7.68 years. Overall, no significant differences were found in gender distribution, age, number of chest pain episodes, nitroglycerin dosage, and BMI between the two groups. However, the chest pain duration between two groups was significantly different (Table 2).
Demographic Characteristics of Phlegm and Blood Stasis Syndrome and Nonphlegm and Blood Stasis Syndrome Groups
Data are represented as mean ± standard deviations for continuous variables and as n (%) for categorical variables.
p < 0.05.
BMI, body mass index; PBSS, phlegm and blood stasis syndrome.
Indexes of Tongue, Face, and Pulse in the Phlegm and Blood Stasis Syndrome and Nonphlegm and Blood Stasis Syndrome Groups
Abbreviations of indexes are fully explained in Table 1.
Data are expressed as mean ± standard deviation for normally distributed variables, or as medium and range for non-normally distributed variables.
p < 0.05.
As for tongue, face, and pulse indexes measured by TCM-IDIs, the NC, length of the crack (LC), number of ecchymosis (NE), AE, length of philtrum (LEP), and right hand pulse h1 (Rh1) in the PBSS group were significantly higher than those in the non-PBSS group. Meanwhile, the GN (green value of nose), BN (blue value of nose), GL (green value of lip), Rt1 (right hand pulse t1), and Rp (right hand pulse p) in the PBSS group were significantly lower than those in the non-PBSS group. Both results were statistically significant (p < 0.05). Other indexes did not show significant difference between the two groups (Table 3).
Results of logistic regression analysis for tongue, face, and pulse indexes
The relationships between indexes and PBSS in patients with CHD were analyzed by binary logistic regression. As demonstrated in Table 4, 14 candidate indexes with p < 0.1 on univariate analysis were included in the multivariable model. In multiple analysis, LC (OR = 1.019, p = 0.002), NE (OR = 2.986, p < 0.001), LEP (OR = 1.090, p = 0.022), and Rh1 (OR = 1.053, p = 0.021) were the independent indexes used to predict PBSS in patients with CHD.
Binary Logistic Regression Analysis of Indexes Predicting Phlegm and Blood Stasis Syndrome in Patients with Coronary Heart Disease
Abbreviations of indexes are fully explained in Table 1.
p < 0.05.
CI, confidence interval; OR, odds ratio.
Construction and results of combining predictor L
With the diagnosis of PBSS as the binary outcome variable and the indexes LC, NE, LEP, and Rh1 as independent variables, the binary logistic regression equation was established as follows: Logit(P) = β0 + β1 LC + β2 NE + β3 LEP + β4 Rh1, where β0 is the constant term; β1, β2, β3, and β4 were the partial regression coefficients of LC, NE, LEP, and Rh1, respectively. Then, the binary logistic regression equation was transformed, and the combining predictor L was obtained: L =
Results of the ROC curve analysis
The results of the ROC curve analysis showed that the ROC-AUC of combining predictor L and the indexes LC, NE, LEP, and Rh1 of PBSS in CHD were 0.825 (95% CI: 0.757–0.892, p < 0.001), 0.646 (95% CI: 0.555–0.737, p = 0.003), 0.710 (95% CI: 0.625–0.794, p < 0.001), 0.619 (95% CI: 0.526–0.712, p = 0.016), and 0.613 (95% CI: 0.520–0.707, p = 0.022), respectively. According to the maximum principle of the Youden Index (YI, YI = Sensitivity + Specificity −1), the cutoff values of combining predictor L and the indexes LC, NE, LEP, and Rh1 for the diagnosis of PBSS in CHD were 238.03, 20.22, 0.50, 26.05, and 21.50, respectively. In addition, the corresponding sensitivity was 72.3%, 49.4%, 53.0%, 65.1%, and 65.1%, and the specificity was 82.8%, 79.3%, 87.9%, 53.4%, and 63.8%, respectively, as shown in Table 5 and Figure 3.
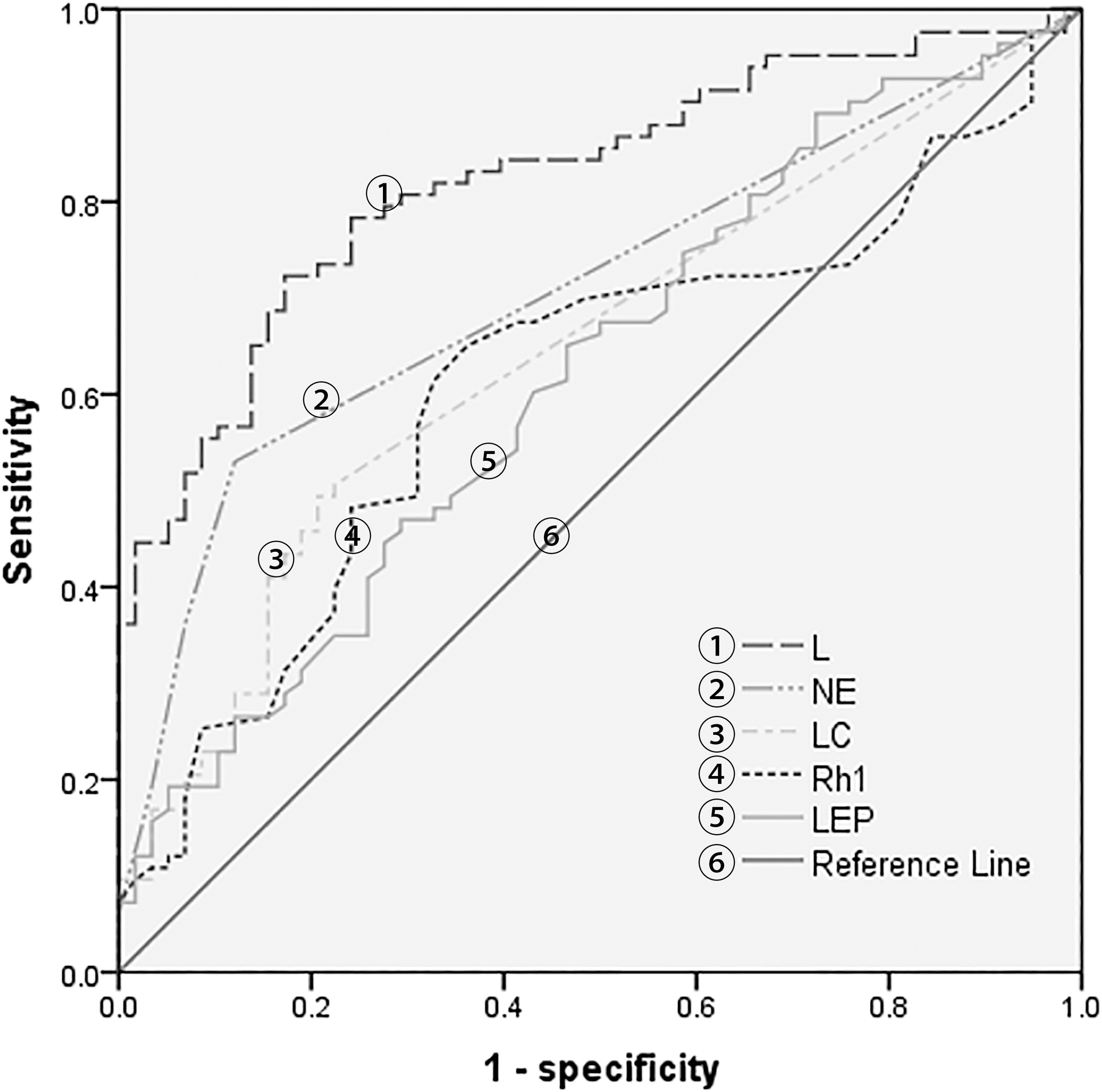
ROC curves of combining predictor L and the indexes LC, NE, LEP, and Rh1 for PBSS in CHD. CHD, coronary heart disease; L, combining predictor L; LC, length of the crack; LEP, length of philtrum; NE, number of ecchymosis; PBSS, phlegm and blood stasis syndrome; Rh1, right hand pulse h1; ROC, receiver operating characteristic.
Receiver Operating Characteristic Results of Length of the Crack, Number of Ecchymosis, Length of Philtrum, Right Hand Pulse h1, and Combining Predictor L for the Diagnosis of Phlegm and Blood Stasis Syndrome in Coronary Heart Disease
AUC, area under ROC curve; L, combining predictor L; ROC, receiver operating characteristic; YI, Youden Index.
Moreover, according to the results, the measured indexes LC, NE, LEP, and Rh1 can be brought into the expression of combining predictor L in clinical application. If the value of combining predictor L is >238.03, it may be helpful for the diagnosis of PBSS in CHD.
Discussion
As a bridge between TCM theory and clinical practice, TCM syndrome differentiation mainly depends on the experience of the doctors. With the development of clinical epidemiology, the introduction of statistical methods into the study of TCM syndromes is the trend for the quantification and standardization of TCM syndrome differentiation.
In this study, first, through logistic regression analysis, tongue, face, and pulse indexes that provide significant contribution to the syndrome differentiation of PBSS in CHD were screened. The logistic regression equation was used to form the combining predictor L, which was used as the diagnosis model of this study. The results suggested that LC, NE, LEP, and Rh1 were the key indexes to distinguish PBSS from non-PBSS in CHD. Furthermore, ROC curve analysis showed that the combining diagnosis model constructed by these four indexes had the highest diagnostic efficiency (AUC = 0.825).
Among these four indexes, LC, NE, and Rh1 were in accordance with the clinical manifestations of PBSS in CHD. According to the allegation of Chinese medical literature, Wang Zhen Zun Jing, the appearance of tongue crack is related to blood vessel and heart diseases. 27 A study on the correlation between cracked tongue and clinical syndromes showed that the incidence of cracked tongue was the highest in cardiovascular system diseases, and cracked tongue was associated with phlegm and blood stasis. 28 Tongue ecchymosis is one of the characteristic signs of blood stasis syndrome, and NE reflect the degree of blood stasis. Xuejuan et al. 29 found that ecchymosis tongue of cardiopathy was the result of microcirculation disturbance in tongue due to the abnormal change of hemorheology to a certain extent.
As for LEP, in recent years, it has been found that LEP is related to CHD and on angina pectoris attack, LEP shortens. 30 However, to date, there have been few studies on the relationship between LEP and TCM syndromes of CHD; therefore, there are no complete diagnostic criteria. Therefore, this study is only an exploratory study on the relationship between LEP and the diagnosis of PBSS in CHD that mainly focuses on the attempt of methods. Rh1 mainly reflects the ejection state of the left ventricle, and can represent the pressure and volume of the systolic artery wall of the heart. 31 Phlegm and blood stasis obstructed the heart vessel and increased the vascular resistance, thereby showing the increase of Rh1.
At present, in the field of TCM syndrome study, logistic regression analysis is widely used for the objective and quantitative diagnosis of TCM syndrome. In this study, through logistic regression analysis, the tongue, face, and pulse indexes, which had decisive significance for the syndrome differentiation of PBSS in CHD, were screened.
In addition, the quantitative relationship between each index and the syndrome was realized by constructing the combining predictor L. Pepe et al. 32 first proposed to establish combining predictor L by logistic regression model; eventually, it has been widely used in many fields. A previous study has found that the prediction ability of the combining predictor L established by fitting multiple independent risk factors was better than that established by a single independent risk factor, and could eliminate the interference among the indexes. 33 Based on this, this method was used to synthesize the multi-index into one index, which not only achieved the purpose of dimension reduction but also improved the diagnostic value of the diagnostic index.
However, it is worth noting that part of the results of logistic regression analysis in this study can only explain the correlation between symptoms and TCM syndromes from a statistical point of view, providing a reference for TCM syndrome differentiation. Therefore, the final judgment and interpretation of the results need to be combined with clinical practice or other research methods.
Limitations
This study possesses several limitations. First, considering the lack of funds and poor compliance of patients, a small sample size was obtained. Second, PBSS accounts for a large proportion in the syndrome types of CHD and is the focus of this study; thus, this study lacks research on other syndromes of CHD to verify the reliability of the method. Third, the data collected were all from Tianjin, which were geographically limited, not representative enough, and lacked the accuracy of large sample data. Fourth, relative to the objective measures of biomedicine, the sensitivity/specificity of the compound measure in this study is modest, and the diagnostic model still needs to be optimized. In addition, this study is only a pilot and exploratory study; therefore, the results of this study are not suitable for clinical application. The diagnosis model of PBSS in CHD needs to be verified through prospective studies. Future studies on quantitative and objective diagnosis of TCM syndromes of CHD will solve the above issues.
Conclusions
This study takes logistic regression analysis as the basic method through the analysis of the correlation between indexes of tongue, face and pulse and TCM syndrome, to achieve the preliminary analysis and screening of the characteristics of variables. This study not only provides a new method for quantitative syndrome differentiation of TCM but also provides a good basis for follow-up study.
Footnotes
Acknowledgments
The authors thank the team of Professor Yu Chun-quan of Tianjin University of Traditional Chinese Medicine for their help in this study. They also thank all the subjects for providing invaluable data and Enago for the English language review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Basic Research Program of China (973 Program, No. 2014CB542901).
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.