
Abstract

Affective disorders are heterogeneous group and the aetiology of this mood disturbance is to date unknown. Different studies provide strong evidence especially in bipolar disorder for a genetic component.
Possible participation of the renin angiotensin system in regulating of the mood has been suggested as the angiotensin II is a neurotransmitter that interacts with dopamine in certain brain areas and angiotensin converting enzyme (ACE) has been shown to modulate dopamine turnover in the corpus striatum [1]. The use of ACE inhibitors in hypertensive patients resulted with euphoric or depressive mood alterations and ACE levels have also been found to associate with various psychiatric disorders.
The ACE I/D polymorphism seems to influence therapeutic outcome in patients suffering from unipolar major depression [2]. In a case-control study, Arinami et al. reported a significant excess of D allele in 65 Japanese patients with affective disorders [3]. Thus, the aim was to explore the possible role of ACE I/D gene polymorphism in the functions of Turkish patients with bipolar or unipolar affective disorders.
Eighty-one mood disorder patients and 90 control subjects (all Turkish) were included. Forty-four patients with bipolar disorder (mean age: 37 ± 14 years, female: 54.5%) and 37 patients with unipolar depression (mean age: 35 ± 12 years, female: 63.9%) were consecutively recruited from the outpatients unit of Psychiatry Department, Karaelmas University. All patients and controls gave informed consent for participation in the study.
The insertion/deletion polymorphism within the intron 16 of the ACE gene resulted in 190 bp and 490 bp amplicons, respectively. Genomic DNA was extracted from peripheral blood and the polymerase chain reaction amplification was performed as described in the literature [4]. The SPSS v.11.0 for Windows (SPSS Inc., Chicago, IL, US) was used to analyse the data and p-value < 0.05 was considered statistically significant.
The distribution of ‘DD’, ‘ID’ and ‘II’ genotypes of the ACE gene were 18 (40.9%), 19 (43.2%) and 7 (15.9%) for patients with bipolar disorder, 11 (29.7%), 18 (48.6%) and 8 (21.6%) for unipolar major depression, and 32 (35.5%), 35 (38.9%) and 23 (25.6%) for healthy controls, respectively (see Table 1). There was no significant difference between the groups (p = 0.634) when either of the affective disorder groups were analysed separately or together.
The distribution of ‘DD’, ‘ID’ and ‘II’ genotypes of the ACE gene in both groups
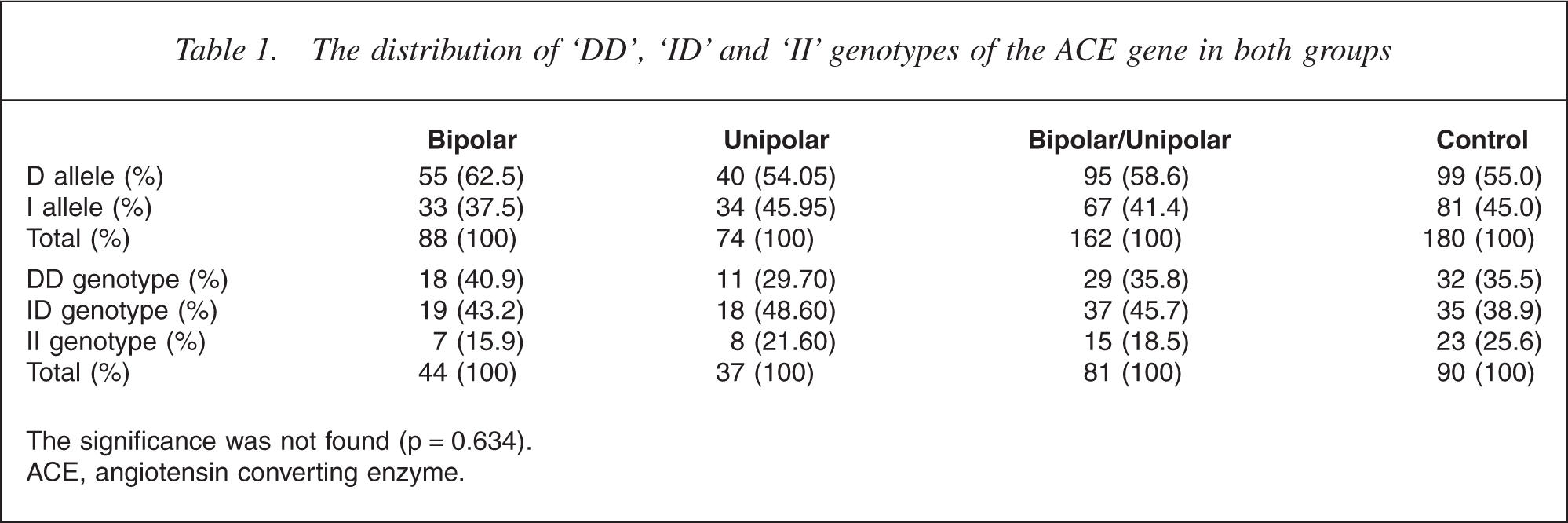
The significance was not found (p = 0.634). ACE, angiotensin converting enzyme.
Our results did not replicate the previous studies claiming the presence of an association between ACE I/D polymorphism and affective disorders in other population. In our study, the number of D alleles was higher in the bipolar and unipolar group than I alleles while it was vice versa in controls. And the number of I alleles and II genotype was the least in both groups.
Our negative finding confirms the recent studies which have demonstrated negative associations for major depressive disorder and the ACE gene I/D polymorphism [5, 6].
In conclusion, our result suggested that this polymorphism does not play a major role in the pathogenesis of major depressive disorder in our populations. Ethnic differences might be responsible for these discrepancies. The possible relation between ACE gene polymorphism and clinical manifestations such as age of onset, treatment response, family history, course of illnesses and gender differences ought to be investigated in a larger groups.