
Abstract
Diagnosis in psychiatry increasingly struggles to fulfil its key purposes, namely, to guide treatment and to predict outcome. The clinical staging model, widely used in clinical medicine yet virtually ignored in psychiatry, is proposed as a more refined form of diagnosis which could restore the utility of diagnosis, promote early intervention and also make more sense of the confusing array of biological research findings in psychiatry by organizing data into a coherent clinicopathological framework. A selective review of key papers in clinical medicine and psychiatry which describe clinical and clinicopathological staging, and a range of related issues. Clinical staging has immediate potential to improve the logic and timing of interventions in psychiatry just as it does in many complex and potentially serious medical disorders. Interventions could be evaluated in terms of their ability to prevent or delay progression from earlier to later stages of disorder, and they could be selected on clear-cut risk/benefit criteria. Biological variables and a range of candidate risk factors could be studied within and across stages, and their role, specificity and centrality in risk, onset and progression of disorder could be greatly clarified. A clinicopathological framework could be progressively constructed. Clinical staging with a restructure across and within diagnostic boundaries with the explicit operationalization of criteria for extent and progression of disorder should be actively explored in psychiatry as a heuristic strategy for the development and evaluation of earlier, safer, and more effective clinical interventions, and for clarifying the biological basis of psychiatric disorders.
Diagnostic diffusion in psychiatry
Diagnosis is central to quality medical care, yet in psychiatry its value has been repeatedly questioned. The function of diagnosis is to indicate what treatments should be chosen and to predict outcome or prognosis. How well these tasks are achieved determines the utility and validity of the diagnostic process. Psychiatric diagnosis is at best syndromal. Despite efforts to shore up reliability, the latter remains a problem outside of research settings, and serious concern persists regarding clinical utility and predictive validity [1, 2]. Diagnostic concepts such as psychosis, schizophrenia and depression are too broad for treatment selection and prognosis, yet even at the macro level, these boundaries may be carving nature at the wrong joints, so subtyping could also be awry. Our official diagnostic systems have also impeded the search for neurobiological and psychosocial risk factors. The DSM-IV and ICD-10 are characterized by artificial divisions based on cross-sectional symptom sets infused and confused with course of illness variables. Clinical features that occur early in the course are not differentiated from those that become apparent as a disorder persists. Diagnostic concepts are typically derived from tertiary and chronic samples where the impression of stability and validity is enhanced. Such diagnoses make more sense in those settings and can be best viewed as stable outcome variables rather than useful tools for guiding early intervention or treatment of less severe cases. Most importantly for clinicians, the greater recognition of ‘comorbidity’ and the rise of polypharmacy and broad-spectrum psychosocial interventions are reflections of our lack of progress in diagnostic reasoning. Is there a more useful framework for clinical reasoning available in other areas of clinical medicine that can be usefully applied, particularly earlier in the course of most mental illnesses?
Clinical staging as a solution
Clinical staging is a deceptively simple and practical tool in other areas of medicine. Most often its value is recognized in the treatment of malignancies, where quality of life and survival are both thought to rely on earliest possible delivery of effective interventions. In fact it is a somewhat broader concept, which has been applied in diseases as diverse as osteomyelitis, sarcoidosis, autoimmune diseases and idiopathic myelofibrosis [3–5]. Originally, in Hodgkin's disease [6], staging was purely clinical and there is still an obvious preference for rapid and non-invasive methods of staging of disease. Dorothy Reed [6] referred to two clinical stages of Hodgkin's disease, the first characterized by lymphadenopathy and the second by systemic symptoms. Clinical staging is often enhanced, where the pathology of the disease can be characterized, by clinicopathological staging, which involves blood tests, biopsies, imaging and even diagnostic surgical procedures. Clinical staging could now be readily applied in psychiatry and progressively buttressed by linkage with clinicopathological correlates.
What is clinical staging?
Clinical staging is simply a more refined form of diagnosis. It differs from conventional diagnostic practice in that it tries to define the extent of progression of disease at a particular point in time, and consequently places greater emphasis on detailed description of where a person lies currently along the continuum of the course of illness. The differentiation of initial and milder clinical phenomena from those that accompany illness extension, progression and chronicity lies at the heart of the concept. It strengthens the clinician's capacity to select treatments relevant to earlier stages, and assumes that such interventions will be both more effective and less harmful than treatments delivered later in the course. Additionally, it seeks to improve prognostic estimates both with and without available interventions. Like diagnosis in general, while staging links treatment selection and prediction, its role in treatment selection is more crucial than its role in prediction, particularly since early successful treatment may change the prognosis and thus prevent progression to subsequent stages. The fundamental assumptions of clinical staging are twofold. First, patients in the early stages of an illness have a better response to treatment and a better prognosis than those in later stages. Second, the treatments offered in the early stages should be more benign as well as more effective. The latter is also based on established principles for early diagnosis and risk-benefit considerations [7]. The lessons emerging from aggressive treatment of early cancers, which can lead to severe complications including secondary malignancies, underline this second principle [8].
What kinds of disorders lend themselves to the clinical staging model, and could it be applied in psychiatry? It may be thought that it would be of most utility in disorders which are believed to inevitably progress without treatment, and most notably malignancies. We would argue that such ‘extreme diseases’ are not the norm, and that even many cancers do not inevitably progress. The advent of more effective interventions has clearly supported the utility of clinical staging in cancer. Perhaps the disorder needs to be capable of spontaneous remission or arrest, or be curable in some cases, for staging to be of value. Staging and early treatment should increase the chances of cure or of reducing mortality and disability. Schizophrenia was once thought to be inevitably progressive, even though soon after its formulation, clinicians such as Bleuler highlighted the fact that the syndrome could arrest or even gradually improve over time. We now know that its outcome is very heterogeneous and that it responds to earlier intervention strategies [9]. Clinical staging can potentially be useful for any disease or disorder which tends to progress or which may progress. This includes many or most psychiatric disorders. Staging would be probably of lesser value in disorders, such as Huntington's disease, that are inevitably progressive at the present state of knowledge.
Course of illness and staging
Consideration of the course and so-called ‘natural history’ of disorders is an essential part of the context for developing clinical staging. However, course and outcome variables have been used as a proxy to validate syndromal diagnosis in a confusing and non-systematic manner from Kraepelin to DSM IV. This has been characterized as prognosis invading diagnosis. To some extent it is unavoidable since some persistence of symptoms beyond the trivial is required for a syndrome to be meaningful, and some impact on functioning or quality of life should be part of the ‘need for care’ [10] aspect of a clinical diagnosis. Two clinical examples are relevant here. First, it is more useful to recognize that anxiety disorders often precede the later development of depressive disorders rather than arguing for separation of these conditions into distinct diagnostic categories. Second, persistent subthreshold psychotic phenomena, depression and other clinical features, in the context of early psychosocial decline often herald the onset of frank psychosis or severe mood disorders. In both situations, traditional cross-sectional approaches would argue that the ‘real’ diagnosis can only be made after development of the eventual outcome. Similar thinking underpins the time-honoured questioning of a schizophrenia diagnosis if the patient remits or responds well to treatment. The ‘real’ diagnosis is challenged. While diagnostic stability is undoubtedly improved by postponing clinical decisions, the opportunity for provision of early interventions that potentially change the clinical outcome is tragically lost. The search for neurobiological correlates of the major psychiatric disorders currently dominates international research efforts. Importantly, much of this activity utilizes patients with long-standing disorders that present more stable diagnostic features. However, the results of such research may be quite misleading. For example, while hippocampal atrophy may be characteristic of persons with major depressive disorder [11, 12], it is unclear as to whether this is reflective of differing aetiological processes in some subgroups (e.g. early vs late-onset) or is simply a correlate of duration of untreated illness [13]. Similarly, while frontal and temporal cortical changes, including the same hippocampal atrophy seen in depression and posttraumatic stress disorder, are common in persons with established schizophrenia, it appears that while some aspects may be present prior to onset of psychotic phenomena, others emerge only after the onset of frank psychotic features [14]. A staging approach would help to distinguish vulnerability markers from sequelae of disease, which may in turn be common across current syndromal categories. A staging model in psychosis is also challenging the hitherto dominant neurodevelopmental paradigm in schizophrenia which is now being shown to have overstated the specificity and importance of perinatal vulnerability, and prematurely attributed biological changes that are active around onset to a much earlier phase of development.
Principles and criteria for staging
Clinical staging was first proposed over a decade ago in psychiatry by Fava and Kellner [15] as a ‘neglected dimension in psychiatric classification’ (p.225) and specifically elaborated by our group for psychotic disorder [16, 17]. Since then it has been constructed and extensively researched through the early psychosis paradigm [18–20]. Although Fava and Kellner [15], who also highlighted the importance of prodromal research, focused on anxiety and mood disorders, there has been little practical development of staging in this arena to date [21]. As with any diagnostic process, clinical staging imposes subcategories on dimensional phenomena [22]. Early psychosis represents a clinical research paradigm which has shown that treatment needs are indeed phase-specific, that pathophysiological changes differ according to phase and duration of illness, and indeed some of these can progress. The staging model in early psychosis represents a broad prototype for a more comprehensive approach in all severe mental disorders. However, in contrast to staging in medical illnesses where anatomic extent and impact of the disease determine stage, it has been hitherto based in a potentially circular way on a course-based ‘phase’ of illness model, which utilizes duration and relapse criteria in defining stages. Can the early psychosis model be evolved to more closely resemble the staging models for severe medical illness and in the process cover other potentially severe mental disorders? Table 1 depicts our prototype of a clinical staging framework for psychotic and mood disorders, within which biological markers can be progressively introduced to build a clinicopathological model.
Clinical staging model framework for psychotic and severe mood disorders
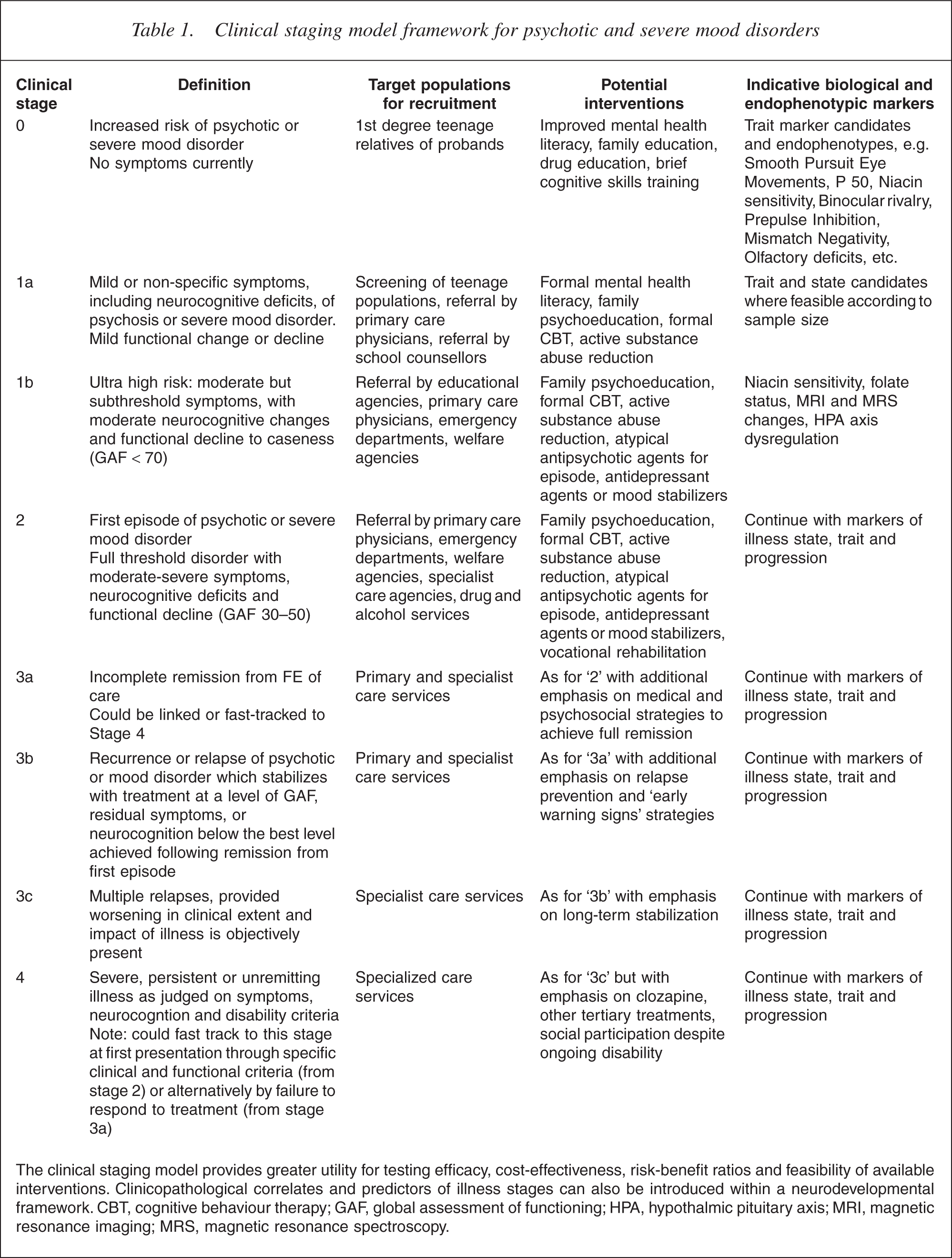
The clinical staging model provides greater utility for testing efficacy, cost-effectiveness, risk-benefit ratios and feasibility of available interventions. Clinicopathological correlates and predictors of illness stages can also be introduced within a neurodevelopmental framework. CBT, cognitive behaviour therapy; GAF, global assessment of functioning; HPA, hypothalmic pituitary axis; MRI, magnetic resonance imaging; MRS, magnetic resonance spectroscopy.
The ideal staging model is clinicopathological, where clinical features are augmented by objective measures that link to pathophysiology and hence might more accurately guide treatment selection and prognostic statements. Clinical staging always remains of central importance however [23]. ‘Vascular depression’ is a clinically derived concept which has been strengthened by magnetic resonance imaging (MRI)-determined structural change, resulting in new therapeutic foci and outcome targets [24]. Determination of serotonin-transporter polymorphisms in younger persons with emerging anxiety or affective phenomena may help to determine those who could be prevented from subsequently developing severe depressive disorders with pharmacological or behavioural interventions. Prediction of outcome in first episode psychosis is substantially enhanced by the inclusion of the magnetic resonance spectroscopy variable NAA/Cr ratio [25]. However, despite these encouraging signs, we are not yet close to defining a clinicopathological model of staging in psychiatry, although we hope that it may progressively be built on the foundations of a clinical staging model.
Clinical stages in other medical conditions are defined by the degree of extent, progression and biological impact of illness in the patient, which in turn must correlate with prognosis. This approach depends upon a capacity to define pathologically as well as clinically the limits or extent of the disease process. In clinical psychiatry this could involve not only a cross-sectional biological definition, but also a wider biopsychosocial definition of extent or progression. Intensity, persistence and frequency of clinical phenomena such as hallucinations, delusions, obsessional thought, panic attacks or depressed mood form one element. Quality of clinical features can be useful, so bizarre and Schneiderian content does reflect more serious progression and portent in psychosis, and early intervention may reduce the prevalence of such content [26]. Neurocognitive impairment, neurological soft signs and other motor signs could also be incorporated. Non-invasive biological markers, such as MRI determined change in brain volume in cortical and subcortical regions, olfactory deficits, genetic variables such as COMT and serotonin-transporter gene status, and other endophenotypic markers which can be shown to reflect progression or greater severity of the disorder could ultimately be included. A clinical staging model could then be used to determine which biological markers could ultimately be useful in treatment selection and prognosis.
To further customize our model for use in psychiatry, we could draw in key social variables as indicators of illness extent and progression, such as social isolation or vocational failure, which typically flows from untreated or poorly treated illness. As with biological phenomena, such as hippocampal atrophy in people with depression or schizophrenia, this may be simply a consequence of late intervention and be correlated with duration of untreated illness. However, it may be partly true that late treatment is also a marker of more severe intrinsic illness [27]. In any case, a person who presents for initial treatment with a great deal of collateral personal and social damage is less likely to respond to interventions (i.e. be more treatment resistant at that point whether primary or secondary) and hence more likely to have a worse prognosis (whether on a social or biological basis). Some of these patients, as in cancer medicine, first present with advanced or extensive disorder and may therefore need a stage 4 initial treatment plan, rather than a simpler and more benign stage 1 package. Others graduate to stage 4 in the course of (unsuccessful) treatment. The prevalence of the so-called deficit syndrome in schizophrenia [28] is 6–10% in first episode cases and rises to over 25% in established schizophrenia [29]. While dramatic responses to treatment still may occur in later stage cases (as seen with clozapine), it is likely that long-term disability will be hard to reverse.
Finally, the place of recurrence or relapse in clinical staging in psychiatry needs to be considered. In medicine generally, relapse is often linked with extension as well as recurrence of the underlying disease process. If so, first relapse would reflect progression to a more advanced stage, and might indicate the need for a different pattern of interventions, as well as a more guarded prognosis. Again, in psychiatry we could use not only biological and clinical criteria for assigning stage in the context of relapse, but also social criteria. So, simple return of the same clinical syndrome with no ‘extension’ of any kind (say the accretion of negative symptoms, or deeper neurocognitive impairment; further loss of grey matter; or more severe social deficits) would not lead to allocation to a higher stage. Examples would include recurrent episodes of schizophreniform disorder or major depression that are accompanied by full remission and social recovery.
The heuristic clinical and research benefits of clinical staging
Clinical benefits: practical prevention strategies
Defining discrete stages according to progression of disease creates a preventively orientated framework for the evaluation of interventions. The key outcomes are prevention of progression to more advanced stages or regression to an earlier stage. This requires an accurate understanding of those broad social, biological and personal risk factors which influence progression from one stage to the next. We especially need to know the relative potency of these risk factors and whether they are malleable by current interventions. While some factors may operate across several or all stage transitions, others may be stage-specific. Clinical examples include substance abuse, specific psychosocial stressors, cognitive style, medication adherence and social isolation, while genetic and biological risk factors are beginning to be uncovered.
Research benefits: towards clinicopathological clarity
One hundred years of research with traditional diagnostic categories of psychosis and severe mood disorders has failed to relate these concepts to any discrete pathophysiologies [1, 30]. Many have argued that the sequence should be reversed, and that we should seek more simply the clinical correlates of objective biological changes [1]. The problem with this suggestion is that we do not know which biological changes are central to disease and moreover to specific diseases, and which are epiphenomena, markers or consequences. The enthusiasm for determining ‘endophenotypes’ is the latest conceptual step which aims to solve this conundrum. It is, however, essentially a stepping-stone concept [31] for linking clinical states with biological deviations which fall short of disease status. Its success depends on the validity or centrality of the endophentypes, an elusive precondition for nosological reversal.
A clinical staging model, which allows the relationship of biological markers to stage of illness to be mapped, may help to validate the boundaries of current or newly defined clinical entities, and distinguish core biological processes from epiphenomena. The clinical staging model would also allow state to be better distinguished from trait and enable much existing knowledge to be better represented and understood. Moreover, it can be constructed and tested right now. In summary, clinical staging is a heuristic yet practical concept which bridges clinical and research domains. Finally, while an aetiological classification is often seen as a vital goal, this has not been achieved in a number of medical diseases, where treatment is nevertheless highly effective. Rees recently emphasized that biological understanding needs to flow out of sound clinical science: ‘The cause of disease is not some objective God's eye summary of pathophysiology, but rather an operational statement of where we think the Achilles' heel of a disease might be’ [32], p.699]. Aetiology is certain to be multifactorial in most cases of severe mental disorder, and a staging model for treatment may still be useful beyond the elucidation of causal risk factors, which are typically of most value for primary prevention rather than enhanced clinical care.
Challenges and complexities
As with any heuristic model, it is easy for critics to see the flaws and challenges inherent in a clinical staging approach. However, we are confident that staging can deliver greater utility in the targeting and evaluation of intervention strategies in psychiatry, and release the overwhelming logjam of biological research findings, with a progressive increase in clarity as to the significance and specificity of biological change in psychiatric disorder. Our current categories are pitched at precisely the wrong level. Our recommendation is for further ‘lumping’ at the macro level, for example merging psychoses and mood disorders at least, and then ‘splitting’ or subtyping within such a supercategory utilizing a staging approach.
There are important lessons to be learned from the experience of early diagnosis strategies in clinical epidemiology, where screening and proactive case finding change the prognostic mix of the sample, even though the clinical phenotype in focus remains constant. Various biases, notably lead-time bias and length-time bias, are introduced which will affect the evaluation of outcome. This fact alone means that in early intervention programs, definition of clinical stage and characterization of risk of progression has to be modified according to how the sample was attracted or assembled [33]. A key risk is that more toxic treatments from advanced stages will be applied universally in earlier stages, despite the fact that the prognostic mix does not yet justify this approach. So there is a genuine tension between early intervention and safety [20, 34].
The clinical staging concept has much to offer psychiatry but it must be explored in a scientific manner in settings which have the capacity to blend and quality treatment with clinical and biological research. Biological clarity will depend not only neuroscientific progress but also on the quality of our clinical science and critical thinking.
Footnotes
Acknowledgements
This work was supported in part by a National Health and Medical Research Council of Australia Program grant to the authors, and by generous research support from the Colonial Foundation. The authors also wish to sincerely thank Dr Rosemary Purcell for her assistance in preparing and editing the manuscript.