
Abstract
Court diversion schemes have been running for a decade in New Zealand and are increasing in number in Australia. This paper aims to give an international and historical context to these developments, by reference to psychiatric initiatives at courts in the US and in England and Wales. From a review of the specialist literature, an account is given of three forms of psychiatric intervention in courts over the last 90 years: court psychiatric clinics and mental health courts in the US, and court diversion schemes in England and Wales. High levels of psychiatric morbidity among prisoners, coupled with a continuing increase in prisoner numbers, demonstrate the need for systems for dealing with mentally ill people who come before the courts. Court diversion in England and Wales developed as part of a system where the mentally ill who are found guilty are sent to hospital in lieu of any other sentence. Its focus is on a form of psychiatric triage, and its ethos is the health of the patient. Court psychiatric clinics in the US grew up as an alternative to assessment in prison. Their focus has been on full psychiatric evaluation in an insanity and incompetence jurisdiction. The ethos has been that of serving the court. Mental health courts are heavily influenced by ideas of therapeutic jurisprudence, and their emphasis has been on a judge holding minor offenders in community care through the threat of judicial sanction. Experience in England and Wales has shown that court diversion can be a powerful and effective intervention. In order for it to function properly, those running court schemes need direct admission rights to psychiatric beds, both open and locked. Court diversion schemes are best as part of a spectrum of services to police stations, courts and prisons, which involved both general and forensic psychiatrists.
Australian and New Zealand Journal of Psychiatry 2006; 40:529–538
The term ‘court diversion’ has been employed to describe interventions for three different groups in the criminal justice system: adolescents – with some special services in existence since at least 1909 [1]; drug users; and the mentally disordered. This paper is restricted in focus to psychiatric interventions at the courts concerning the mentally ill. The shape that such interventions take depends on the provisions of mental health law in a given jurisdiction, and upon the way interactions between mental health services and the criminal justice system have developed historically. The account below aims to give an historical and international perspective to current court diversion efforts in Australia and New Zealand, mainly by reference to developments in the US and in England and Wales. Diversion, for these purposes, is taken as ‘a policy of transferring the mentally ill away from the criminal justice system and into psychiatric care’.
Background
The extent of the problem that has stimulated the growth of diversion schemes is illustrated by the high prevalence rates of serious mental illness in prison populations, particularly among those on remand, and by the continuing increase in prisoner numbers across the western world.
In England and Wales, 10% of unsentenced men and 21% of unsentenced women had experienced a psychotic illness in the last 12 months [2]. Equivalent figures for male prisoners in New South Wales were 10.9% [3] and in New Zealand 6.8% [4,5]. Figures for currently psychotic male remand prisoners were 5% for England and Wales [6], 4–7% for New South Wales (depending on definition) and 2.7% for New Zealand.
In the US, 16.2% of state prison inmates and 16.3% of jail inmates were thought to be mentally ill, using a definition based on self-report of a ‘mental or emotional condition’ or of previous admission to a psychiatric hospital [7]. In the year of the survey (1998), this amounted to an estimated 283 800 people. Jails and prisons have, in effect, become front-line mental health providers in the US [8]. However, of those with mental illness, 40% in state prisons and 60% in jails were receiving no treatment [7].
Over the past 10 years, the prisoner population in Australia has increased by nearly 50%, from 15 866 in 1993 to 23 555 in 2003. This increase has exceeded the 15% growth in the Australian adult population, resulting in the adult imprisonment rate increasing from 119 to 153 prisoners per 100 000 adult population between 1993 and 2003 [9]. The New Zealand prison population increased by 40% from 4443 in 1992 to 6240 in 2003 [10]. The prison population of England and Wales increased by 66% from 45 817 in 1992 to 76 069 in June 2005. In the US, the total prison and jail population rose from 501 886 in 1980 to its current figure, an increase of 420%. (See Fig. 1)
Numbers incarcerated in the USA. (——) Total incarcerated, (–––) state prisoners, (– · –) jail inmates, (····) federal prisoners.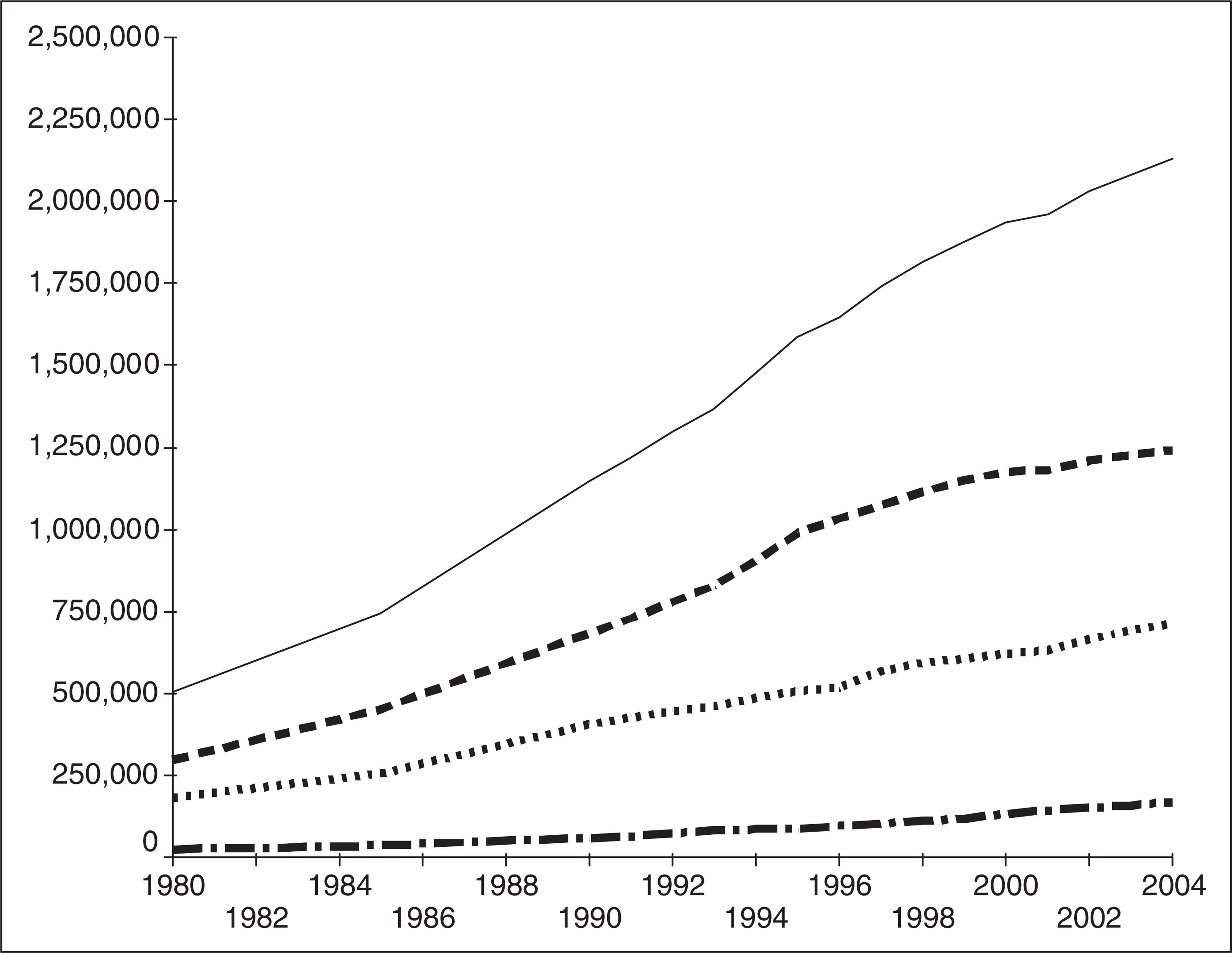
The rate of incarceration per 100 000 population for England and Wales in 2003 was 141, the highest in the European Union and above the mid-point of the world list. Equivalent figures for Australia were 115 (the whole population rate, rather than the adult population rate given above), for New Zealand 155, for Canada 116 and for the US 701, the highest in the world [11]. In the US at the end of 2003, 6.9 million people were on probation, in jail or prison, or on parole, this being 3.2% of all US adult residents or 1 in every 32 adults [12]. In mid 2004, there were 2.1 million people incarcerated in the US. Prisoner numbers in these countries have increased year on year and it is projected that they will continue to do so. There is no suggestion in the available literature that the proportion of prisoners with mental illness declines as prisoner numbers increase.
Reasons for attempting to intervene in this situation are various. The obvious humanitarian argument was well stated in the US in the case of Ruiz v Johnson (Ruiz v Johnson, 37 F. Supp.2d 855 [S.D. Texas, 1999]): ‘It is deplorable and outrageous that this state's prisons appear to have become a repository for a great number of its mentally ill citizens. People who, with psychiatric care, could fit well into society, are instead locked away, to become wards of the state's penal system. Then, in a tragically ironic twist, they may be confined in conditions that nurture, rather than abate, their psychoses.’ Second, in some jurisdictions, an improvement in the position is a legal necessity, whether relating to human rights law or individual cases brought in the civil courts.
However, a third motivating factor, at least within the US, is that of money. It is expensive to keep people in jail, and more expensive with the mentally ill. In 2004, Miami-Dade County in Florida reported spending $4 million per year on overtime in order to manage mentally ill prisoners on 15 minute observations. Figures from Broward County in Florida, where the first mental health court was established and which has a population of 1.5 million, indicated that the mentally ill cost $160 per day to keep in jail. In 1996, 3882 mentally ill people passed through the jail for an average of 23 days each, at a total cost of $14.2 million. Jail inmates who are not mentally ill cost on average $78 per day. Other counties in different parts of the US have reported similar figures. In this context, there has been a push to develop systems which keep the mentally ill out of jails. This has given a boost to diversion initiatives. In November 2000, President Clinton signed US Senate Bill S. 1865, authorizing the creation of up to 100 mental health courts and $10 million a year for 4 years for their maintenance [13]. In October 2004, the US Congress passed the Mentally Ill Offender Treatment and Crime Reduction Act, the stated purpose of which was ‘to increase public safety by facilitating collaboration among the criminal justice, juvenile justice, mental health treatment, and substance abuse systems’. The Act allocated $50 million in federal funds to support diversion programmes, including mental health courts.
The following account will consider and compare three different models of intervention: court psychiatric clinics, court diversion schemes and mental health courts.
Court psychiatric clinics
In England and Wales, services for the mentally disordered within the criminal justice system developed from assessment at remand prisons. In the US, input was from an early stage concentrated at the courts. The first court diversion service in England and Wales was established as a pilot in 1989. For a psychiatrist to examine people at court was new to London, but such arrangements had been established for three quarters of a century in the US.
The first formal psychiatric scheme at a US court, known as the Psychopathic Laboratory, started up in the Municipal Court of Chicago on 1 May 1914 [14]. In a 9 month period in 1929–1930, the Psychopathic Laboratory examined 722 separate cases, of which 47% were committed to institutions. The Laboratory had its own facilities at court and was staffed by a psychiatrist, an assistant psychiatrist, two nurses, a social worker and a secretary. There was emphasis on cooperation with other agencies and the need for the ‘maintenance of a suffi-ciently large, high-grade and scientifically trained personnel’. Assessments were intended to be comprehensive: ‘In order to examine an offender in a proper manner, it may be necessary, not merely to interview the prisoner, but to contact all available sources of information, such as relatives, the complainant or complainants, the school record, court record, and so forth. In addition thereto, each individual should have a physical examination, including an examination of his nervous system, and the absence or presence of definite mental disorder or mental retardation should be established by suitable tests. Field calls and follow-up work are frequently necessary’.
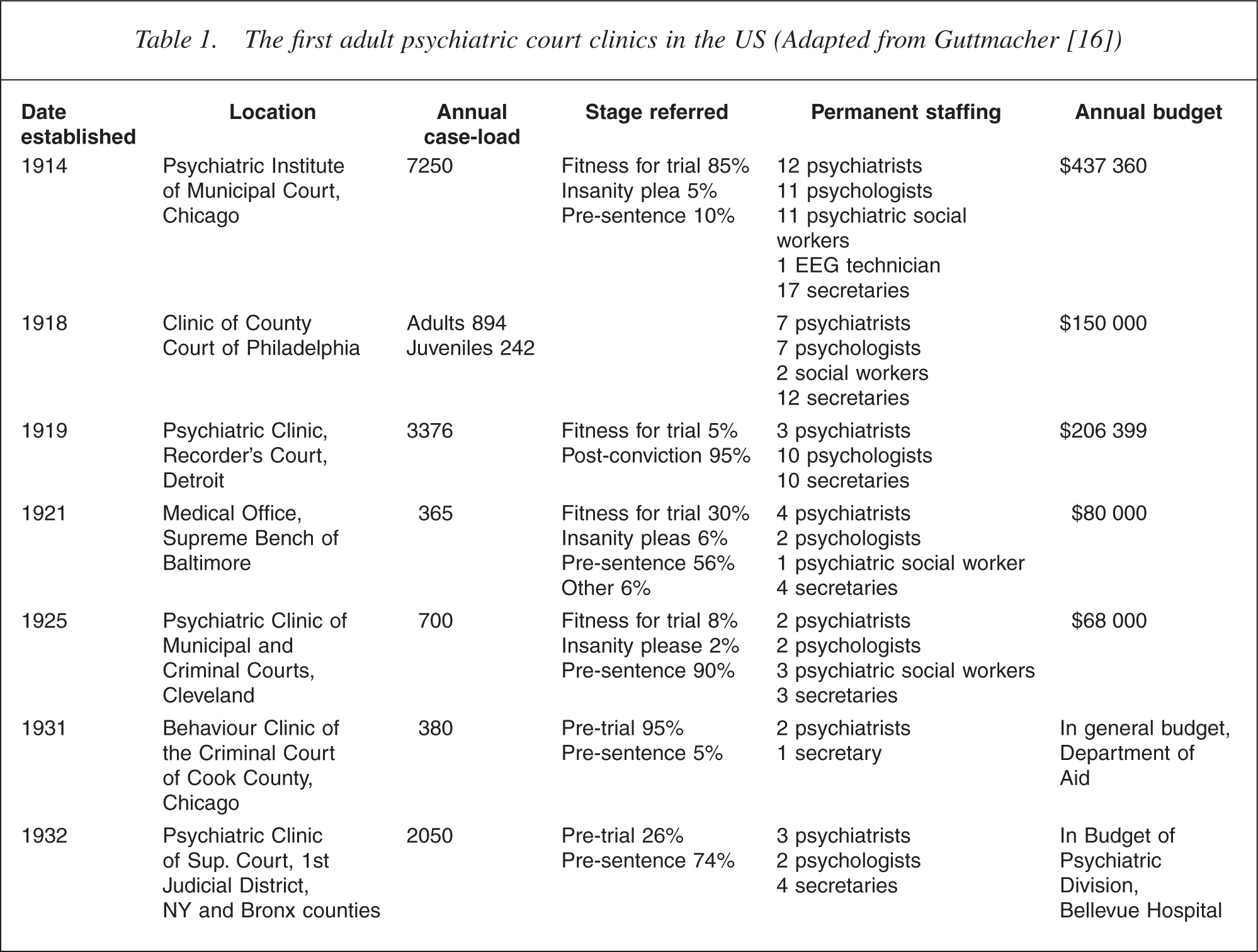
A second scheme began in Baltimore on an informal basis in 1917, with the psychiatrist being paid as a bailiff, before his post was formally constituted from 1921 onwards as the ‘Medical Office of the Supreme Bench’ [15]. Manfred Guttmacher, who was in charge of the Baltimore service from 1930 to 1966, listed 27 court psychiatric clinics that had opened in the US by 1962 [16]. The characteristics of the first seven are listed in Table 1 below. It is evident that the clinics were wellstaffed, well-financed and busy. This may in part have reflected a new optimism about the application of science to the problem of criminality. The number of psychologists is likely to have been linked to what was, according to Oliver [15], the ‘hey-day of mental tests’, in particular assessments of intellect. The considerable variation in function between the court clinics is evident from the differences in legal stages at which their cases were referred. This in turn reflected differences in function of the courts in which they were located and differences in law between individual states.
The first adult psychiatric court clinics in the US (Adapted from Guttmacher [16])
In 1989, it was estimated that court psychiatric clinics numbered ‘probably higher than 100 and closer to 250 – the approximate number of metropolitan areas in the United States’ [17]. It should be noted that many of the court clinics on the US model were set up in higher courts.
According to Selling [18], ‘the purpose, function, and value of the court clinic’ was ‘to provide the judge with scientific knowledge which will aid him to understand the defendant and to assess sentence accordingly; to recommend and in some instances to carry out various types of treatment procedures in particular cases; to demonstrate its worth to the judge; and to fulfil an educational purpose in showing what can be done with offenders through the medium of its reports and recommendations’. It is evident that the second of these purposes of court clinics, initiating and enforcing treatment procedures with the threat of legal sanction, was a small part of their function, and concerned minor offenders, and often involved juveniles, family court issues or drug and alcohol problems. Such treatment enforced by a court in conjunction with a psychiatric court clinic was not without its critics. Fersch [19] sought to determine the function of treatment in the court clinic setting, asserting that there should be ‘definite limits to the means employed to push unwilling patients into therapy’.
In more recent times, the function of psychiatrists operating at court in the US has diverged along two lines. The coercive role of courts in enforcing treatment has been reflected in the development of drug courts and mental health courts. Meanwhile, the function of court clinics is in most cases clearly separated from that of treatment. The psychiatrist at the court clinic has the court as his client and his function is to serve the needs of the court, not those of the people that pass before it [20,21]. This reflects the dominant view in US forensic psychiatry – alien to forensic psychiatrists in the UK, Australia and New Zealand – that those preparing reports to the courts should not be involved in the treatment of the individuals concerned [22]. It also reflects the reality of the legal position and service configuration in the US, where the mentally ill who are found guilty are incarcerated in the penal system, rather than being diverted into psychiatric hospital.
Mental health courts
The first mental health court was set up in Broward County in Florida in 1997 [23]. Their number increased rapidly to nearly 100 in 2004 [24]. Their structure and function has been extensively described [25–27]. Mental health courts follow the ‘therapeutic court’ model of the drug courts. Based upon ideas of therapeutic jurisprudence [28,29], they use various creative methods to enforce compliance to treatment in the community: ‘preadjudication suspension of prosecution of charges; postplea strategies that suspend sentencing; and probation’ [30]. The mental health court is dedicated to the processing of people with mental illness. The court has a ‘mental health judge’ with a particular interest in the area and cases are referred across from other courts, if there is ‘voluntary’ agreement of the accused to participate. The court will liaise with mental health agencies and mandate participation in treatment programmes, mainly in the community. The court retains control and monitors the progress of the case. If the person fails to comply, the court can apply sanctions, either by continuing with the prosecution in cases where the process has been suspended at the pre-adjudication stage, or by adopting another form of sentence in post-plea cases, including custodial sentences.
Mental health courts deal only with minor offences and cases involving violence are generally excluded. The courts do not have any resources of their own and rely upon other agencies for assessment and treatment. The ‘voluntary’ nature of the participation of the accused in the mental health court process has been questioned, and it has been suggested that the more severely ill may not be competent to make decisions about participation [31]. Some doubts have been expressed about the selection of referrals to mental health courts, with those referred being more likely to be older, white and women than the general population of individuals involved in the criminal justice system [24]. There have been some difficulties in evaluating the effectiveness and outcomes of the courts [32], particularly with regard to improvement in mental state, although measuring outcome variables such as social situation may be more appropriate in the chronically psychotic population concerned. It appears that those passing through the Broward County mental health court spent significantly fewer days in jail than a reference group, which is of both humanitarian and financial interest; there was, however, no significant difference in re-arrest rates or number of violent acts during the 8 month follow-up period [33]. It has also been pointed out that the length of time from referral to diversion is much longer in mental health courts than in other types of diversion programme [34]. If the courts are dealing only with minor offenders, then it should be possible to divert such cases at the pre-arrest stage or at least before they reached court. This would, however, remove the advantage of enforcing treatment in the community, which mental health courts provide.
Court diversion and liaison in England and Wales
The first court diversion in England and Wales began in 1999 in central London. This was only a few years before the first such arrangements were established in New Zealand [35]. The shape of the services reflects the nature mental health law in England and Wales and the way that psychiatric services developed in the UK. In England and Wales, those who are found guilty of a criminal offence and who are suffering from a serious mental illness are sent to hospital for treatment as a sentence by the court. Issues of criminal responsibility are irrelevant except in homicide cases, where a reduction in responsibility is enough to permit a hospital disposal. Because a guilty verdict results in a person being sent to hospital, at which point the court relinquishes all control over the case, there is usually little point in pursuing issues of fitness to plead and of insanity, which are generally avoided and have been reduced to something of an historical curiosity. In such a system, diversion schemes become a powerful tool, capable of dealing with both minor and serious offences.
Court diversion schemes are located at magistrates' (lower) courts. The logic of this is that such courts serve a number of police stations and concentrate cases from a given area, thus constituting an efficient place in the system to which to commit resources. In some cities where there are many magistrates' courts, the court diversion schemes are centred at one central court, to which the other courts can cross-remand cases for assessment, so resulting in a further improvement in efficiency.
It is clear that magistrates' courts (previously known as police courts) have long been frequented by the mentally ill, both in criminal and civil matters. The following description refers to the latter years of the 19th century: ‘Day after day, year after year, a never-ceasing progression of humanity passes through our police courts… the ever-increasing army of the demented ones in their hopeless conditions and with their inexplicable delusions. One is persecuted by the police; another is shadowed by an assassin; another someone is trying to poison. A poor woman wants the telephone-wire removed – it talks to her…’ [36].
There are little data on the current level of psychiatric morbidity among those passing through such courts. At one inner-city court, 6.6% of custody cases were found to be suffering from serious mental illness (i.e. psychosis or major depression): 1.3% of those bailed by police to appear at court were similarly afflicted [37]. Two sorts of system have grown up, depending on the number of mentally ill defendants passing through a given court. A low referral rate or need for admission leads to the development of ‘liaison schemes’, which are generally run by nurses and function by linking cases in to local psychiatric services, with an emphasis on those based in the community. Where the need is greater, ‘diversion schemes’ are developed with the aim of admitting people into hospital from the court. The most developed of these are consultant-led, with several psychiatrists, nurses, social workers and an administrator, working out of dedicated and well-equipped offices in the cell areas at court, with their own interview facilities.
The aims of diversion schemes are to assess, at court, people in custody and admit them to hospital where indicated, using either the forensic provisions of the Mental Health Act 1983 (UK), or the civil provisions where the offences are less serious. Minor offenders will be admitted to general psychiatry units, those committing serious acts of violence to forensic units. With charges that can be dealt with at the magistrates' court, admission to hospital is likely to be as a sentence after a finding of guilt or the discontinuance of a charge. In serious offences, which are destined for the higher Crown Court, admission to hospital will be organized pending trial after assessment by court schemes, often through Home Office warrants, rather than through court powers.
In effect, the schemes have two purposes: to increase the recognition of mental illness at the courts, and to accelerate admission into hospital. Where no scheme is present, the magistrate has to remand cases to prison for reports. The prison health-care staff has to identify the responsible sector consultant and arrange for him or her to visit the (often distant) remand prison. Once there, the patient will be seen without the benefit of access to prosecution papers or past medical history. If a recommendation is signed for a hospital disposal, there will then be a further delay until the person's next court appearance.
It is much more efficient to short-circuit this system by having the psychiatrist examine the accused at the originating court. At court, the psychiatrist will have access to the prosecution papers. Any past psychiatric reports will be gathered from hospitals, general practitioners and social services by fax or direct computer link. The referred person will be interviewed, a detailed typed report prepared, and admission to hospital arranged. The psychiatrist will be available to appear in court to resolve any problems, and the social worker will negotiate transport.
Quality standards for court diversion schemes and for their audit have been developed and published [38]. In practice, the system works best when staff running the schemes are from the psychiatric service local to the court, and have direct admission rights to psychiatric beds, including secure facilities [39,40]. Under mental health legislation in England and Wales, it is possible for local hospitals to attempt to obstruct admissions on forensic admission orders. There are no powers for hospitals to resist admissions on civil orders, for which they are obliged to find a bed within hours, even if this means funding placement in the private sector. This can lead to pressure to use a combination of civil orders and bail to hospital. It is important for the success of court diversion arrangements that they form a contractual part of the local core psychiatric service and are funded as such. This ensures that all parties involved are formally committed to the project, and determines that disputes between court diversion teams and receiving facilities are less likely to arise.
A weakness in current systems concerns case selection. In some schemes, there is a screening procedure for all custody cases at court, generally based on examination of files [41,42]. There is evidence that the use of questionnaires may improve detection rates [37]. But most schemes depend on referral procedures, which rely on the question of mental disorder being raised by nonmedical personnel. Another disadvantage of current schemes is that many only operate on certain days of the week. This results in referrals often requiring to be remanded into custody until the day on which the court scheme operates: this may act as a disincentive to the referral of appropriate cases.
Court diversion schemes were originally set up as personal projects by interested psychiatrists [43]. There followed 5 years of ‘pump-priming’ monies provided by the Home Office, rather than the Department of Health. When these finished, it became Department of Health policy that all general psychiatric services should make arrangements for psychiatric assessment at courts and police stations, as well as prisons [44]. In 1999, there were said to be 150 court diversion or liaison schemes operating in England and Wales. Annual surveys of the schemes, organized by National Association for the Care and Resettlement of Offenders, suggest that their number has declined and that many of the schemes are insuffi-ciently staffed and financed to carry out their function effectively. In the 2004 survey [45], 78% of schemes surveyed were unable to collect statistics describing their function. Fifty per cent had no input from a psychiatrist and 72% cited a lack of beds as a barrier to their scheme operating effectively. Twenty-five per cent of schemes had seen a decrease in their staffing in the past year. This is a picture of a system in decline, as predicted by James [39]. However, there are signs that the Department of Health is showing a renewed interest in court diversion in 2005, and a joint working group between the Home Office and the Department of Health has selected court diversion as one of three action topics. The NHS National Research and Development Programme on Forensic Mental Health has commissioned research on programmes for women within court diversion. At a time when 78% of schemes do not collect statistics and, of those that do, 42% do not record gender, there seems a disparity between central aims and the reality of practice. It is to be hoped that this may be resolved through a new impetus for the creation of effective schemes, even if this is partly driven by concerns about rising prisoner numbers.
Efficacy of court diversion in England and Wales: process
There has been extensive examination of the efficacy of court diversion schemes in terms of process. There are indications that such schemes can increase the identifi-cation rates for mental disorder. There was a fourfold increase in compulsory admissions from one court after the introduction of a diversion scheme [46]. Of those compulsorily admitted through another court scheme after a period in remand prison, 39% had not been recognized as ill at the remand prison [47]. A common finding is that time from arrest to admission is reduced from an average of 7 weeks to 1 week [46,48,49]. Court schemes have proved able to deal with serious offenders as well as minor offenders: in one area, there was no difference in seriousness of offending between admissions through court schemes and those through prison assessment [50]. The mechanism proved so powerful that, in 1 year, one court diversion scheme in London (and its two psychiatrists) were responsible for 12% of all the unrestricted hospital orders in England and Wales [51]. More details of these findings can be found elsewhere [39].
Efficacy of court diversion in England and Wales: outcome
Although the efficacy of the court diversion process appeared to have been demonstrated, concerns about the effects of such services on general psychiatry units were initially expressed. There were suggestions that those admitted through the schemes constituted a new population of patient, previously hidden in the criminal justice system and unknown to psychiatric services, and that, as such, their transfer to health services should have been accompanied by a dowry [52]. Marshall [53] asked: ‘Could there be a link between London having pioneered court diversion schemes and the level of violence on its acute wards?’ An early pioneer of the schemes questioned whether admitting cases into general psychiatry wards accomplished anything in the long run, given the standard of care available: ‘There is a danger that court psychiatrists, whilst improving the quality of life of the magistrates before whom they appear, will do little for their patients, simply leading them out of the “revolving door” and up a blind alley’ [54].
A comprehensive case–control study, funded by the Home Office, examined outcomes of those admitted through court diversion schemes, comparing a sample of 214 such cases with 214 compulsory admissions from the community under the civil provisions of the Mental Health Act, matched for hospital and month of admission [40]. The main findings were that court diversion admissions, when compared with civil community admissions: were no less likely to complete their admissions; had similar lengths of stay; were no more likely to be violent or to abuse substances in hospital; were less likely to use intensive nursing resources (i.e. ‘specialing’); achieved a similar improvement in mental state by the time of discharge; and were not readmitted any more quickly. The court admissions were more likely to be reconvicted in the 2 years at liberty following discharge. However, there were highly significant reductions in numbers of convictions in the 2 years at liberty following discharge from hospital than in the 2 years before admission. In addition, the reconviction rate for the court diversion admissions in 2 years at liberty following discharge was only 28%. This compares with 2 year reconviction rates in national cohorts of similar composition of 56% for discharged prisoners and 58% for those placed on community penalties [55]. The authors concluded that the court admissions were a similar population to the civil admissions and that admission through the courts probably represented a different style of accessing psychiatric care, analogous to the manner in which some people habitually access physical care through emergency departments, rather than general practice clinics. They suggested that there was no evidence that court admissions caused more problems to general psychiatry wards than civil admissions, and that admission appeared to have an effect in reducing offending. The reduction in offending concerned mainly theft and similar offences. The hypothesis was put forward that any reduction in offending might be a consequence of people being housed, linked into social security benefits and receiving social care and support as a result of their admissions.
Criminal justice liaison
Psychiatric diversion schemes at courts, of whatever type, should not be seen in isolation, but rather as part of an integrated spectrum of services at police stations courts and prisons. There are few areas in which this ideal has been properly established. However, there are well-developed systems, in the US and the UK, for diversion before the stage of appearing in court. In the US, these can be divided into pre-booking and post-booking schemes. In pre-booking schemes, mentally ill people who commit minor offences are directed towards care, rather than being charged. Post-booking schemes concern jail diversion schemes, in which those detained in jails are screened and directed towards health care [56]. In the UK, some areas have police station diversion schemes, in which psychiatric nurses are on call for police stations, where they examine those that appear to be mentally ill and organize compulsory admission where appropriate. This is a more sensible way of dealing with minor offenders. As with most court diversion schemes, these services are more logically a component of general psychiatry services, rather than forensic psychiatry services [57].
A comparison of the three court psychiatric systems
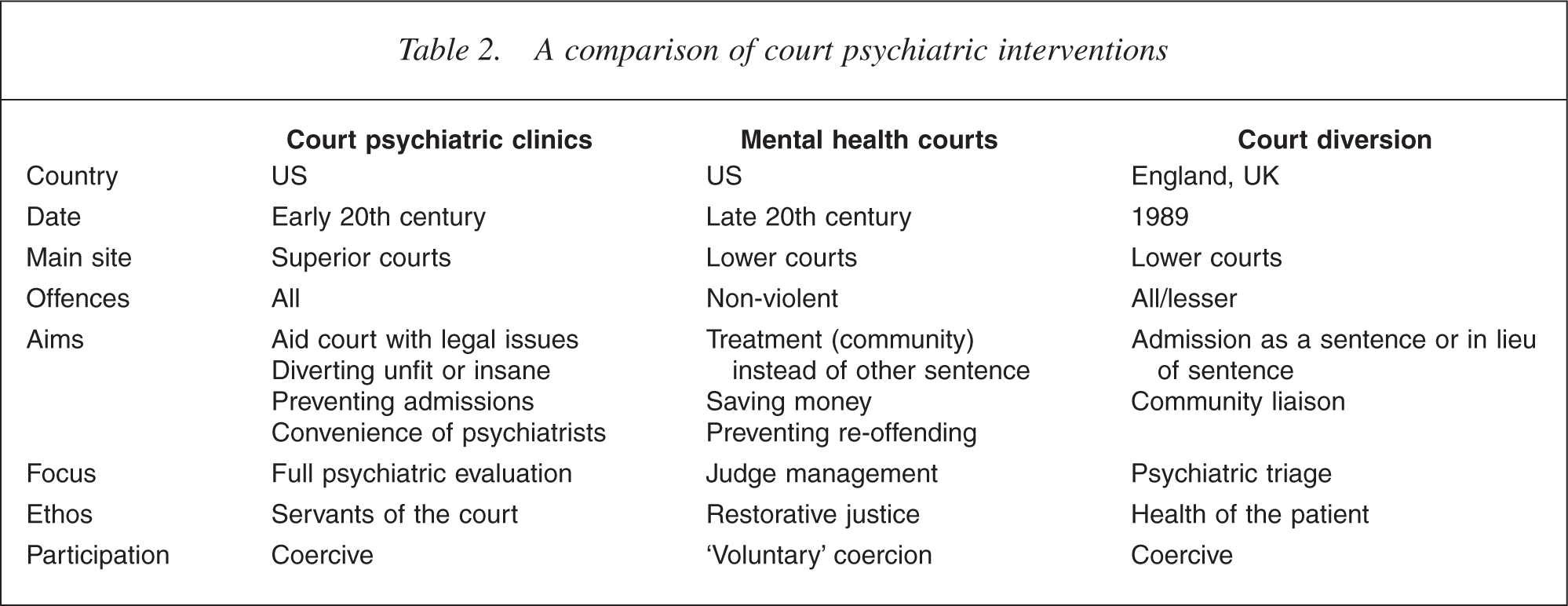
The main features of the three systems are summarized in Table 2. The major differences are in ethos. Those working for court psychiatric clinics function as servants of the court: mental health courts are courts, and their functioning is heavily influenced by ideas of restorative justice and therapeutic jurisprudence; the focus of court diversion is upon the health of the patient. Court psychiatric clinics, in a competency and insanity jurisdiction, aim at full psychiatric evaluation of offenders in a setting that avoids hospital admission. The setting is also one that is more convenient for the psychiatrists concerned than having to travel to a jail. Mental health courts are presided over by judges who manage mental health careplans. Court diversion schemes serve a triage function, with the most ill cases admitted, the less ill linked to community provisions and the remainder not offered any psychiatric input. Mental health courts practice a form of ‘voluntary’ coercion, whereas the other two are more openly coercive. Court psychiatric clinics are different from the other two in that the majority are located in higher courts, rather than lower courts. They deal with serious offending, whereas mental health courts deal with minor offending only, and court diversion schemes may deal with both serious and minor offending. Court diversion schemes aim to admit people to hospital, whereas court psychiatric clinics aim at avoiding admission to hospital for assessment where possible. Mental health courts are mainly concerned with treatment in the community and can be seen as a creative way of enforcing compulsory treatment in the community in states where there is no legislative provision for this.
A comparison of court psychiatric interventions
Although the three systems are very different, the factors that have been found to be important in making them successful are very similar. The most important elements are a firm funding base; adequate staffing for the intended function; ‘ownership’ of the project by all the agencies involved; and good outcome data and quality control. For court diversion schemes, direct admission rights to hospital beds, particularly on general psychiatry wards, are the key to ensuring efficacy: this is where schemes in Australia might fall down.
Perhaps the most fundamental similarity between the three systems is in what they represent. The need for the existence of such services is an indictment variously of poor investment in community psychiatric services, inadequate mental health legislation, and the inhumanity of societal systems which allow the imprisonment of the mentally ill.