
Abstract
Little systematic evidence is available about how violent offenders remember and think about their violent crimes. The general aim of this article is to selectively review a range of different ‘types’ of memory disturbance and their risk factors, in an attempt to draw together different strands of research concerning memories of offending that might usefully be considered together for clinical purposes. A selective review of psychiatric or psychological studies related to amnesia, intrusive memories, posttraumatic stress disorder (PTSD), ruminations, and pleasurable memories was performed. The body of research on amnesia in relation to violent crime is relatively small and is subject to significant limitations. The empirical base of studies identifying intrusive memories arising from violent crime is also very limited, with no previous published study primarily focusing on description of the form and content of intrusive memories related to acts of violence in a population of violent offenders. A small number of studies have investigated PTSD directly arising from the commission of a violent or sexual crime, in those with mental illness. No published studies that investigated the presence of ruminations related to violent offending were identified. No systematic comparative studies were identified that described the form and content that positive memories of non-sexual violence might take. Relevant phenomenological reports from extreme populations raise concerns about selection bias. A memory-based approach to eliciting descriptions of violent offending may elicit clinical information relevant to violence risk assessment and therapeutic interventions within forensic settings.
It is striking that very little systematic evidence is available about how violent offenders remember and think about their violent crimes. For example, the literature related to the nature of memories of violence is significantly more developed with respect to victims of violence [1–4], than for those who perpetrated it.
Theoretically, there are several different ways in which violent offenders might remember what they did, in terms of phenomenological form and content. First, there is the possibility that memory for the assault is absent. It is well-recognized that some offenders claim that they cannot remember their criminal behaviour at all (amnesia), which is not only a controversial medico-legal issue, but is also problematic clinically: how does one proceed to formulate a case and evaluate risk if the individual claims they cannot remember what happened? To this point, investigation of claimed amnesia has been the predominant focus of attention with respect to memory research in forensic psychiatry.
A second possibility is that some offenders might be distressed by memories of their violent behaviour. Although the existence of ‘negative’ memories of violence in some violent offenders is non-controversial clinically, it has received little research attention. For example, intrusive memories have been defined by one of the major psychiatric classification systems as memories of a traumatic event that are recurrent, distressing and involuntarily triggered (diagnostic criteria of posttraumatic stress disorder (PTSD), Diagnostic and Statistical Manual of Mental Disorders [DSM]-IV [5], although they are generally thought of in terms of victims of trauma. These recollections tend to be vividly sensory and experienced as relatively uncontrollable, unwanted, and evoke extreme distress [6]. Leaving aside the issue of whether committing a violent act should be considered potentially traumatic, it is of considerable clinical interest to know whether some violent offenders do experience distressing intrusive memories of their violent acts.
A different but potentially related unwanted phenomenological experience is suggested by recent theories, which argue that a distinction should be made between intrusive memories and intrusive thoughts because they are functionally distinct, with intrusive thoughts appearing to represent problematic elaborations of the experience [7–10]. For instance, people might ruminate about why the trauma happened to them or how it could have been prevented, matters arising from the traumatic event rather than representing thoughts that were actually held at the time of event.
Finally, it is clinically important to know whether some violent offenders experience positive or pleasurable emotions in relation to memories of previous violence.
The literature relating to offenders' memories of violent crime is disjointed, with most reviews or articles isolating one particular kind of memory disturbance, especially amnesia for violent crime. No previous review has attempted to provide an overview, let alone synthesis, of the different ‘kinds’ of memories reported in relation to offending behaviour. The general aim of this article is to selectively review a range of different ‘types’ of memory disturbance and their risk factors, in an attempt to draw together different strands of research concerning memories of offending that might usefully be considered together for clinical purposes. The focus in relation to amnesia for violent will on the limitations of published research, as the merits of such studies have previously been reviewed [11, 12].
Method
Computerized Medline and PsychINFO searches were performed covering the period from 1872 to March 2005 using the terms: (i) crim$, amnesia, memory, offence, perpetrator; (ii) PTSD, memory, crime, offence, perpetrator; (iii) rumination, crime, perpetrator; and (iv) crim$, memory, positive, pleasure, sadism. All articles needed to be in English and in a peer-reviewed journal or book. The abstracts were searched for studies in which the focus was on (i) measurement of amnesia for crimes in remanded or sentenced prisoners; (ii) identification of PTSD or intrusive memories of violent offending behaviour in perpetrators; (iii) identification of ruminations related to violent crime in perpetrators; and (iv) identification of positive memories of violent offending. The reference lists of relevant articles were examined for further relevant articles. The review included other relevant papers known to the author.
Results
Amnesia for violent crimes and limitations of empirical data
Table 1 summarizes studies that have addressed the issue of amnesia in offenders, either directly or indirectly. In homicide cases, 25% to 45% of offenders claim amnesia for the offence [11].
Studies of amnesia and crime: clinical and legal findings
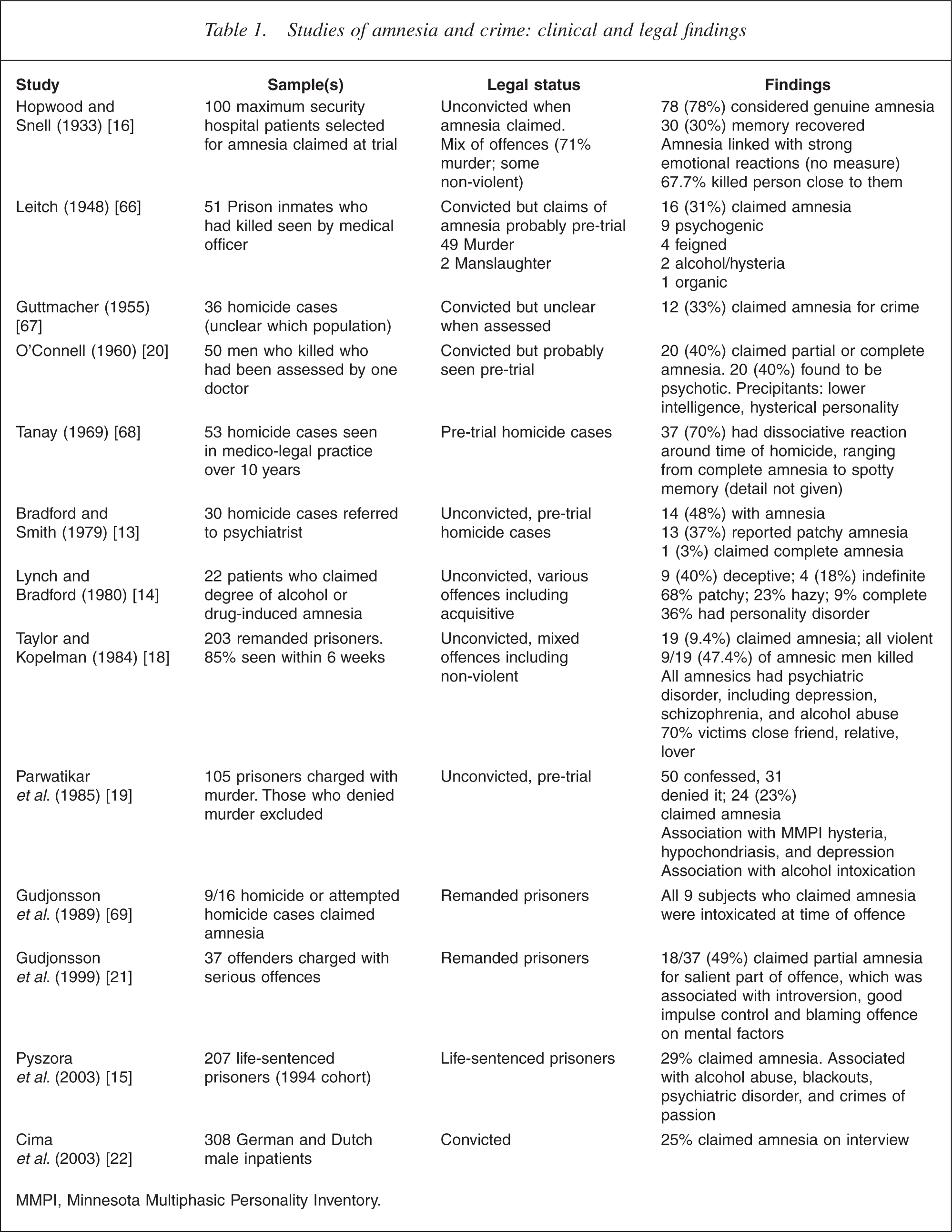
MMPI, Minnesota Multiphasic Personality Inventory.
In overview, the body of research on amnesia in relation to violent crime is relatively small and is subject to significant limitations, including the following:
Inadequate phenomenological description. Previous studies have either not considered the distinction between partial and complete amnesia, or did not report it in detail, leading to a lack of clarity about what could and could not be recalled. Some researchers that have attempted to report the phenomenology of memory gaps for offending in more detail but have used unsatisfactory classifications, for example, the use of ‘hazy’, which implies memory rather than amnesia [13, 14]. There have been suggestions that the majority of alleged offenders report memory impairments circumscribed only to the action of the crime itself [13, 14].
Inconsistent and inadequate measurement of the dependent variable (amnesia). Most studies have failed to provide operational definitions of amnesia and appear to have relied on simple selfreport answers to only very general enquiries. The lack of use of transcripts in study designs has led to an absence of interrater reliability testing, although one study used comparison of some individual's reports to probation officers and psychiatrists as a proxy measure of interrater reliability [15]. Some studies have relied on retrospective case note descriptions relating to information gathered for purposes other than the research study, raising questions of reliability [16].
Pre-trial nature of evaluations. Most studies of amnesia for violent crime are vulnerable to questions about the reliability of amnesia reported by offenders who were unconvicted at the time of assessment because of the potentially confounding effects of the legal process [17]. In some studies, participants were told that the interviews were confidential, and therefore it was assumed that there was no motivation for the subjects to dissimulate because there were no legal implications [18], but this may not adequately capture the complexity of the remand setting and the characteristics of participants in studies of this kind (Evans C: unpublished data, 2004). Although some studies reported that participants were drawn from convicted populations, the data used for analysis actually corresponds to accounts recorded pre conviction, for purposes other than assessment of amnesia [16].
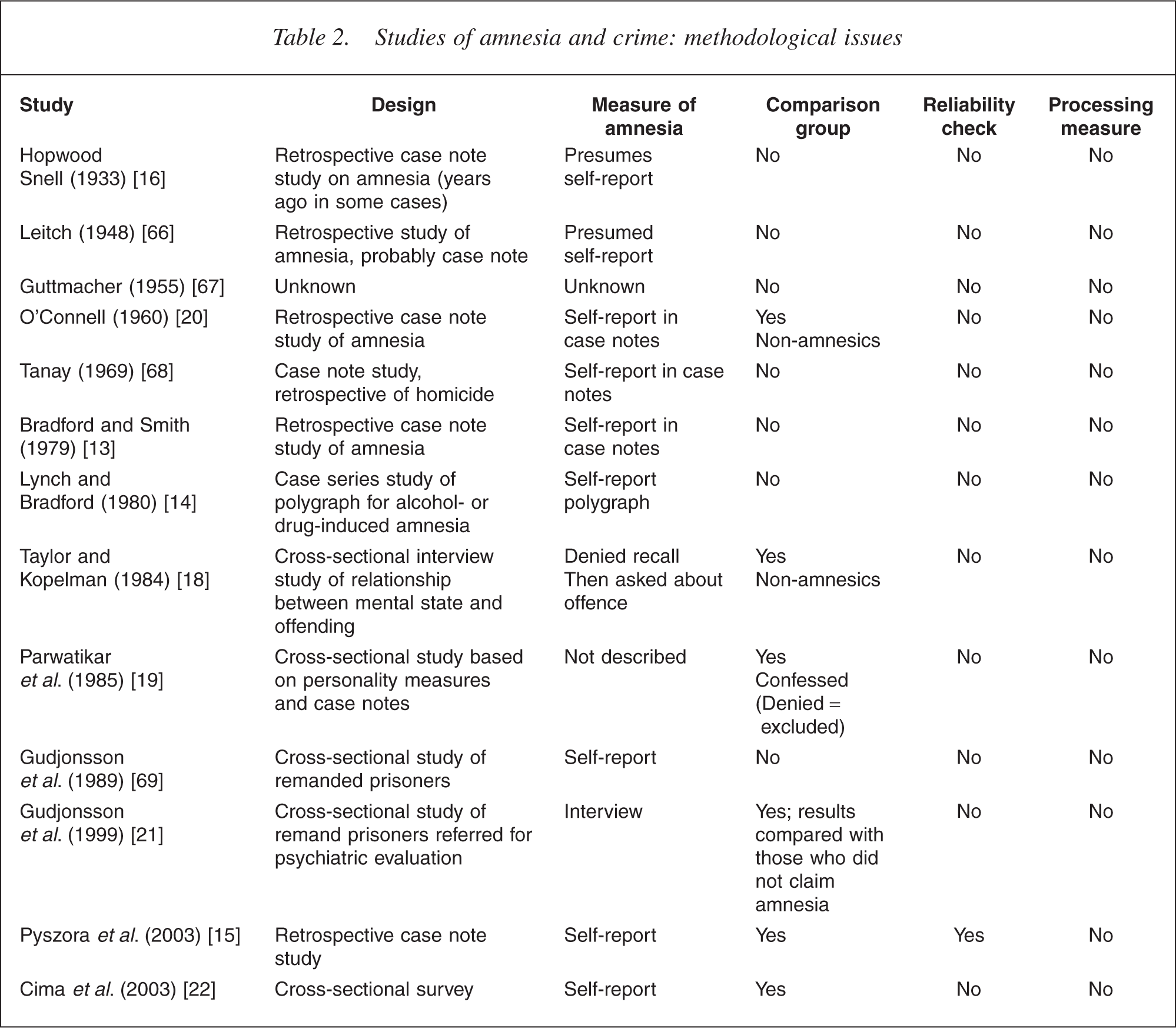
Selection bias. Several study designs did not incorporate a meaningful comparison group. Earlier studies were typically based on a series of cases' referred to specialist services. Similarly, research in this area has mainly focused on offenders who have killed, itself an unusual event, and the extent to which conclusions drawn from homicide studies are generalizable to perpetrators of more common non-lethal violence is uncertain (Table 2).
Studies of amnesia and crime: methodological issues
Risk factors for amnesia for violent acts
There is some preliminary agreement about the risk factors for amnesia related to offending. Histories of both chronic alcohol abuse [14, 16, 18, 19] and/or acute alcohol intoxication [13,18–21] are commonly found in those who claim amnesia for crime. However, examination of these claims shows that three of the four studies usually cited to support this view did not describe how alcohol intoxication was measured. The remaining study found significant more reports of amnesia in those who had consumed ‘high levels’ of alcohol (more than one or two pints of beer in the previous 12 hours) compared with those who consumed less than this, but not for the distinction between those who had consumed any alcohol at all versus those who had not [18].
Some studies have argued that extreme emotional arousal at the time of the offence is associated with claimed amnesia [13, 16, 18, 20] but the available empirical data do not provide strong evidence for this association. The level of emotional arousal present at the time of the offence has typically not been measured directly but, rather, has been implied from a proxy measure, such as the closeness of the relationship with the victim, or even suicide following homicide. There is an absence of more direct measures of emotional states related to the violent incident is unsatisfactory.
Empirical data about cognitive mechanisms is similarly lacking. For example, several studies have suggested that ‘dissociation’ leads to amnesia for offending but no study has attempted to systematically measure the nature of cognitive processing at the time of the offence.
No clear relationship between formal psychiatric illness and the presence of amnesia for criminal offences has been identified, apart from a small number of offenders reported to be psychotic at the time of their offence [11, 18]. The role of personality variables has been inconsistently investigated. An association has been reported between subclinical depressed mood and amnesia, although the claim that depressed mood was ‘usually’ present some weeks or months prior to the offence was not measured systematically and the rates of depressed mood in the non-amnesic group were not given [18]. Personality factors such as introversion and good impulse control [21] and lowered levels of intelligence and relatively poor performance on frontal lobe tasks [22], have been reported as being associated with claimed amnesia for crimes, although the strength of evidence is weakened by absence of replication, relatively low participant numbers, and selection bias, including the presence of mental illness in some participants.
Intrusive memories of violence
The empirical base of studies identifying intrusive memories arising from violent crime is also very limited (Table 3). No previous study has primarily focused on describing the form and content of intrusive memories related to acts of violence in a population of violent offenders. Two small case series and two single case reports that addressed grief and ‘traumatic responses’ in violent offenders were identified, although none gave comprehensive phenomenological descriptions of the intrusive memories [23–26].
Studies including data related to intrusive memories in violent offenders
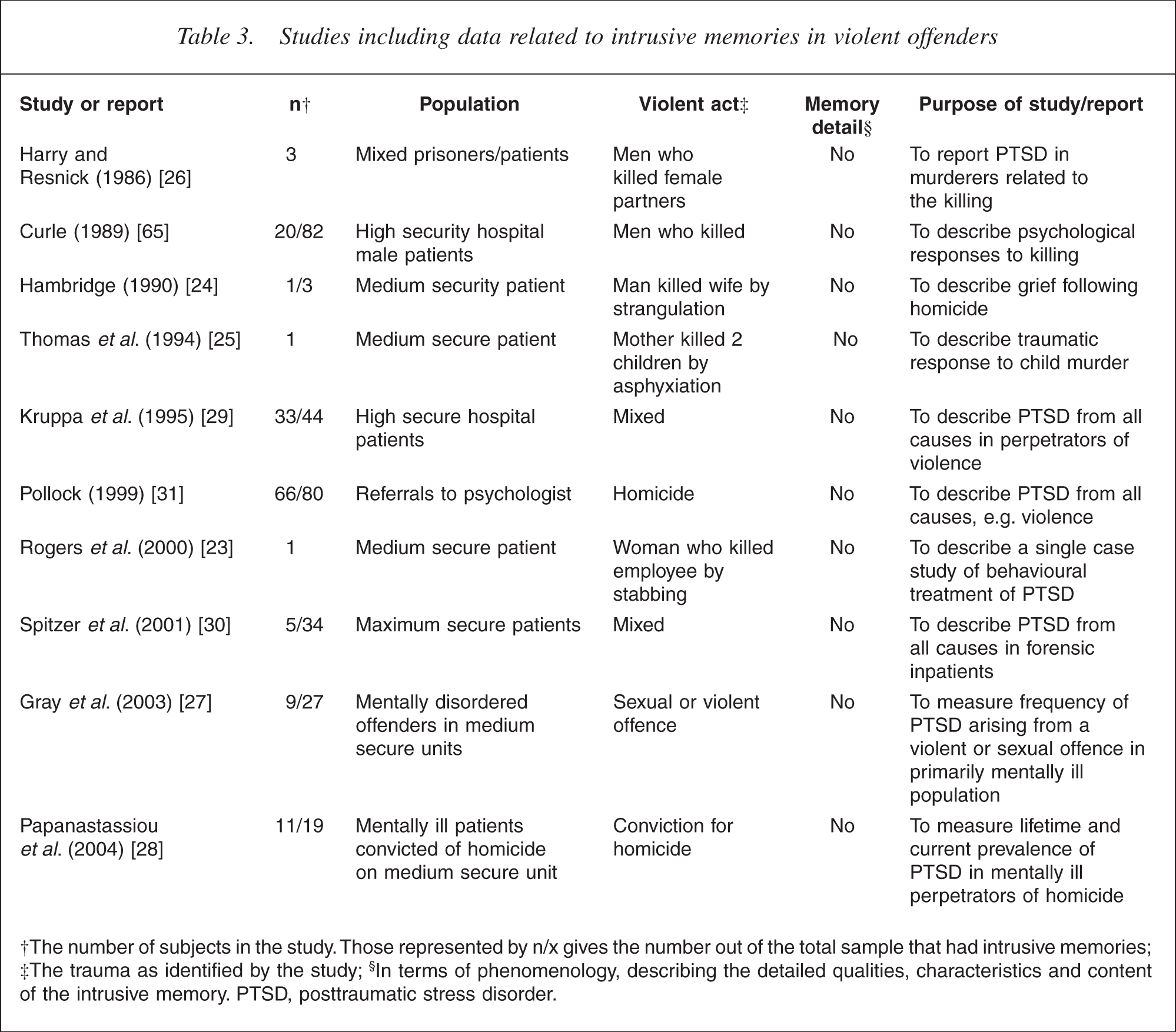
†The number of subjects in the study. Those represented by n/x gives the number out of the total sample that had intrusive memories; ‡The trauma as identified by the study; §In terms of phenomenology, describing the detailed qualities, characteristics and content of the intrusive memory. PTSD, posttraumatic stress disorder.
Two studies have investigated the prevalence of PTSD directly arising from the commission of a violent or sexual crime, in those with mental illness. Gray et al. found that diagnostic criteria for PTSD were met in nine of their sample of 27 (33%) medium secure unit inpatients [27]. In a similar study conducted at around the same time, it was reported that 11 out of 19 patients (58%) had lifetime PTSD arising from their homicide, with eight out of 19 (42%) fulfilling current criteria [28]. However, neither study reported which kind of re-experiencing of the traumatic event was present [5], and, as both of these studies measured psychopathology at the diagnostic level, neither reported phenomenological detail of the specific intrusive memories. These findings are supported by two studies designed to identify PTSD from all causes in forensic inpatient samples, which reported that 33 out of 44 (75%) and five out of 34 (15%) of their selected samples had PTSD in relation to their own criminal offence, respectively [29, 30]. Again, phenomenological description of the specific memories was absent as this was not the purpose of either study. Finally, an investigation of the incidence of PTSD symptoms in 80 perpetrators of homicide found that 52% of the sample met diagnostic criteria for current PTSD, although the homicide was identified as the traumatic event in the majority (82%) of cases [31].
An unpublished study on male homicide patients detained in a maximum security hospital in the UK has more directly addressed the existence of intrusive memories of violent offending in perpetrators (Curle C: unpublished data, 1989). Twenty out of 82 (24%) patients interviewed reported current intrusions and 28 (34%) reported past intrusions related to their act of killing. However, while possibly contributing more than other studies to our phenomenological understanding of the traumatic and psychological responses to having perpetrated serious violence, the study design limits the usefulness of the data for current purposes, including (i) probable confounding of ruminations with intrusions; (ii) minimal phenomenological detail was provided; (iii) the absence of descriptions of the intrusions and the consequent absence of interrater reliability testing, a point related to the decision not to tape-record subject responses; (iv) the highly selected nature of the study participants; (v) the very long length of time from index offence to interview (median time more than 12 years); and (vi) the exposure of participants to potentially confounding clinical interventions.
Ruminations related to violence
No published studies that investigated the presence of ruminations related to violent offending were identified.
Pleasurable memories of violence
No systematic comparative studies were identified that described the form and content that positive memories of non-sexual violence (This article primarily focuses on non-sexual violence, although it is acknowledged that the division is somewhat arbitrary. There is a more substantial literature concerned with the way in which sex offenders incorporate memories of previous offending into current fantasies.) might take. Selection bias is an obvious concern, with samples of patients typically taken from extreme populations. For example, sadism has been reported in descriptive papers of case series of patients detained in maximum security hospitals [32, 33]. The apparent pleasure and satisfaction that the sadistic murderer is said to derive from a capacity and propensity towards detailed recall of their violence [32] has given rise to theoretical explanations of how such extreme behaviour might develop. MacCulloch et al. have argued that sadistic offenders are ‘driven’ to commit their crimes by sadistic fantasies that have been progressively elaborated over time [33]. The power of the fantasies are enhanced by incorporating real-life vignettes from behavioural ‘try-outs’ as part of the fantasy sequence, meaning that the fantasies are partly based on memory of previous crimes. The nature of positive memories of violence (as opposed to non-memory-based fantasies) in less extreme populations is uncertain.
A broader investigation: preliminary report
Some of the methodological and conceptual issues raised by the foregoing selective literature reviews have been addresses in the first study that has systematically investigated both the nature of memories of violent crime and memory gaps in the same offender population, using first-hand accounts from the perpetrators (Evans C: unpublished data, 2004). The design involved a cross-sectional approach, marked out from previous research by combining a relatively large sample of post-conviction participants, including clear operational definitions for dependent variables, having interrater reliability checks, including a meaningful comparison group, and undertaking qualitative and quantitative methods to describe phenomenological features of interest in detail.
The study aimed to investigate the nature of memories of young offenders of their violent assaults in general and, more specifically, to investigate whether some young offenders experience amnesia, intrusive memories, ruminations or positive memories of their violent crime. Although the results of the study will be published elsewhere, examples of all of these categories of memory were found and described in detail. Almost half of the sample reported distressing intrusive memories of the offence even though the average time to interview approached 2 years after the offence. A significant minority reported distressing ruminations related to their offence. A smaller number of offenders reported pleasurable memories in relation to the offence. Complete amnesia was very uncommon but partial amnesia was found in about one-fifth of the sample.
The intrusive memories reported by violent offenders were reminiscent of those reported by victims of trauma, including (i) a predominance of sensory detail such as vivid visual images and may include sounds and other sensations [4, 34, 35]; (ii) a sense of time distortion, such that they seem to be happening in the present rather than the past, an experience called ‘re-experiencing’ [10, 36, 37]; (iii) a tendency to be triggered involuntarily by specific reminders that relate in some way to the circumstances of the assault; and (iv) an associated high level of distress. The phenomenological study also included the first systematic description of the form and content of ruminations consequent to acting violently, which replicated previous reports by victims of violence [38] that ruminations are typically intrusive, difficult to terminate, are both triggered by and precipitate intrusive memories of the offence, and are distressing. The participants seemed to be able to adequately differentiate intrusive memories from intrusive ruminations about the offence. A small number of violent young offenders reported pleasurable memories, and confirmed findings from previous research using university student samples [39], that positive memories may have an intrusive quality.
The phenomenological study of amnesia challenged the findings of a number of previous studies in finding that complete amnesia is very uncommon. Partial amnesia, with good memory recall for the immediate antecedents of the assault, and the aftermath of the violence, was the most typical pattern in those reporting amnesia. The results of the cross-sectional amnesia study replicated previous findings that intoxication with alcohol, and having emotional ties with the victim, were associated with amnesia for the offence. The study also extended previous knowledge by providing the first empirical evidence that cognitive processing at the time of the assault, including dissociation, was associated with amnesia. Contrary to a popular hypothesis in the literature, the intensity of negative emotional states, particularly extreme anger, were not associated with amnesia.
Discussion
Memories of violent offending: a limited database
The selective literature reviews identified a relatively small body of scientific research specifically investigating perpetrators' memories of violent offending, which has significant scientific limitations. An emerging research effort has recognized the capacity of violent offenders to be traumatized by their own violent actions, but our knowledge of the phenomenological characteristics of intrusive memories of violent offending remains in its infancy [Evans C et al. unpublished data, 2004]. No published research papers on ruminative thoughts related to violent offending were identified, and little systematic research on positive memories related to offending outside of the sex offender context was available. It is somewhat ironic that the area of memory research attracting the most attention so far in forensic psychiatry is that of amnesia for crime, that is, lack or absence of memory rather than memories per se.
Although amnesia for crime has attracted relatively more research attention, the methodological limitations of the scientific findings may be at odds with the degree of acceptance that some forensic clinicians appear to have for the phenomenon and its causation. For example, it may surprise forensic clinicians to know that no published research study has used a measure of ‘dissociation’ in its design to support clinical claims that the mental mechanism underpinning psychogenic amnesia is, in fact, dissociation. Despite plausible case reports in individuals who do not contest their culpability for homicide [40], too little is known about the nature of memory disturbance related to the commission of violence to draw strong conclusions about the nature of memory for violent offending.
While no published studies of ruminations related to violent offending were identified, there are preliminary empirical grounds for suggesting that intrusions and ruminations can be seen as associated phenomena [40]. The two different types of experience appeared to be related in a functional sense: ruminations were frequently triggered by intrusive memories, and ruminations also appeared to sometimes trigger intrusive memories. These findings are consistent with the view that the relationship between intrusive memories and ruminations can be described as ‘bi-directional’ [38].
The difficulty in summarizing research on positive memories related to violent offending is related to its diffuse origins and absence of specific research focus with a surprising absence of controlled studies that have directly addressed the phenomenology of positive memories of violent offending. Overall, the phenomenological knowledge base in this area is limited and is largely restricted to accounts of extreme cases involving serial homicide offenders, ‘psychopaths’, and sadistic offenders. Much less is known about the existence of positive memories in less extreme cases, particularly those involving non-lethal violence.
The status of the empirical base regarding risk factors for the various anomalies of memory should also be considered preliminary. As an example, even one of the areas with the most consistent empirical support, the role of alcohol intoxication in amnesia for offending, poses difficulties in interpretation. Caution has been suggested in attributing memory deficits to alcoholic blackouts because blackouts have been held to erase all memory for the duration of time corresponding to serious intoxication [41], whereas, in contrast, the descriptions of amnesia for homicide have been characterized by memory gaps con- fined to the most violent aspects of the crime, with details of what happened immediately before and after the crime being recalled vividly [42, 43]. Reports by the majority of violent offenders with amnesia that memory gaps are partial in nature even in those under the influence of alcohol [Evans C et al. unpublished data, 2004] suggests that further investigation is necessary before a particular ‘type’ of memory gap is held to be the characteristics of alcohol intoxication.
Controversies
As research on memories of violent offending increases, empirical findings will need to be considered within the broader context of important current scientific debates, arising mainly from research on the nature of memories of victims of trauma.
For example, the role of dissociation in causing amnesia for offending is hotly contested. It has been argued that components of the stressful (violent) experience may not become integrated into personal memory and the information in question becomes ‘split’ from autobiographical memory and is not available to consciousness [43]. Evidence cited for a causative role for dissociation in causing amnesia in offenders is limited to specific case reports suggestive of altered mental states; and the general finding that many homicides involve the offender killing a family member, which has been interpreted as indirect evidence that the offender was in a state of extreme emotional arousal at the time of the offence. In line with this hypothesis, it has been suggested that some offenders in a state of uncontrollable rage, coined a ‘red-out’, when they are violent [44], which precipitate an extreme form of emotional statedependent memory, whereby to recall what happened the individual has to regain the emotional state they were in when the memory was initially encoded [44]. In opposition to such views, McNally has argued that many cases of amnesia for traumatic events are better accounted for by either ordinary forgetting or a lack of encoding into memory in the first place [42]. He also cites a substantial breadth of literature that shows that far from undermining recall, emotional stress actually improves memory for traumatic events, at least for its central elements (e.g. [45]). McNally emphasizes that research on dissociative phenomena has been undermined by its application to a range of phenomena and a lack of definitional precision.
A second controversy is the status of ‘traumatic’ memories. Since the 19th century, there have been claims that memories for highly emotional or traumatic events have different properties to those of other memories [4, 46]. Trauma victims have reported memories that appear to consist of sensory fragments, which are unusually vivid, detailed, and enduring and are imbued with strongly negative emotional states reminiscent of the initial trauma and a sense that the trauma is happening again (hence the term ‘flashbacks’) [4, 36]. However, the concept of traumatic memory has been challenged. Claims that traumatic memory primarily consists of sensory segments in the absence of a coherent narrative [4] have been undermined by empirical evidence that some trauma survivors can produce coherent narratives as long as they have adequate verbal intelligence [47]. Some trauma memories, such as those in relation to being the victim of rape, contain less sensory components and were less bright and detailed than other nominated unpleasant memories [48, 49]. Further, some commentators have concluded that rather than postulating special kinds of memory qualitatively different from everyday autobiographical memory, the phenomenology of memory related to highly emotional events can be adequately explained by a combination of ordinary mechanisms and variables, such as cognitive capacity, perceived personal relevance, unusualness of the event, and so on [42]. An especially important mechanism is suggested by the Easterbrook hypothesis, which claims that with increasing levels of arousal due to stress, attention is directed to central features of the arousing event at the expense of peripheral features [50], such as ‘weapon focus’, whereby robbery victims often remember details of the offender's weapon such as a gun, but do not remember much about his appearance [51]. Finally, it has also been argued that every memory, traumatic or not, is fragmented because memory represents a reconstruction of what happened rather than an exact record [42, 52, 53].
Strategies for research
The initial requirement is for further careful qualitative and quantitative descriptive studies of the phenomena concerned [Evans C et al. unpublished data, 2004]. Brewin has noted that our knowledge about psychologically based amnesia is so inadequate as to make any a priori exclusion of certain types of study design inappropriate [54]. Recent advances in understanding the phenomenology of intrusive memories in trauma victims has helped to highlight corresponding gaps in our basic phenomenological knowledge about intrusive memories in perpetrators of violence [1, 2, 8,55–57], such as which aspects of the trauma memory are typically re-experienced, whether individuals experience different parts of the memory at different times, whether they experience parts of the event or the whole event, and how the intrusive memories are experienced [Evans C et al. unpublished data, 2004].
Our understanding of the phenomena concerned would benefit from investigation of the psychological factors underpinning their origin and maintenance. It is clinically important to distinguish between the factors that predict intrusive memories, and those involved in their persistence [58] because while re-experiencing symptoms such as intrusive memories are common in response to a traumatic event, intrusive memories that persist for more than a few weeks are associated with chronic PTSD [59–61]. Several theorists have argued that specific cognitive appraisals of events during the trauma or its sequelae play a role in persistence of PTSD and traumatic symptoms [7, 10, 36,62–64]. Recent investigation of cognitive appraisals of violent offending and its sequelae have been productive in identifying relevant treatment targets for victims of violence, but little research attention has been placed on such appraisals in violent offenders [Evans C et al. unpublished data, 2004].
It has been argued that an alternative route to the development of PTSD symptoms in violent offenders is the development of strong feelings of guilt and shame (as opposed to contemporaneous fear, helplessness or horror, as required by DSM-IV) following the transgression of an important moral code [42]. Theoretically, it can be argued that antisocial appraisals would protect against such feelings of guilt, and in this sense antisocial beliefs and guilt represent opposite sides of an important mediating factor in terms of the development of intrusive memories in violent offenders, an hypothesis that has received some recent empirical support [Evans C et al. unpublished data, 2004].
Investigation of memories of violent offending would benefit from a broader conceptual approach, with a lack of coherence and balance about the nature of the research effort so far (Evans C: unpublished data, 2004). This has probably arisen because the primary motivation for relevant studies has varied, with studies on amnesia for offending driven by legal concerns, while studies on PTSD arising from violent offending may arise from more therapeutic motivation. Study designs that investigate the presence of different phenomenological forms and content of memory for violent offending concurrently are required to tease out the relationship between the different ‘types’ of memory for violent offending.
Clinical implications: mental state examination, therapeutics and risk
A patient's ‘account’ of their offending should not necessarily be taken at face value as representing the totality of their memory of their violence. The way that an individual describes what happened is necessarily underpinned by their memory of the event, but the memory itself, other motivations, or situational factors may modify the account given. For example, an individual may fabricate a false story for perceived legal or personal gain; their intrusive memories or personal discomfort may lead to cognitive avoidance and underreporting of some aspects of memory; or a lack of systematic questioning may limit the nature and extent of the information elicited. Although it is standard practice within the forensic psychiatric community to ask patients for their ‘account of events’, it is far less common to see precise accounts of exactly what the individual can remember, what they cannot, whether any specific areas of memory intrude and, if they do, their specific nature, the patient's interpretation of these, and so on. For example, the author has encountered individuals who are able to describe in detail their violent crime when questioned about form and content of memories, only to later claim that they ‘cannot remember’ what happened when asked for their account (Evans C: unpublished data, 2004).
Therapeutic possibilities arise from a phenomenological or memory-based approach to the description of violent offending –such strategies have been used for treatment of victims of violence with good effect [7, 10, 36,62–64]. Memory is central to human behaviour because it underpins our ability to learn from past behaviour and to adapt to new situations. The provisional findings that intrusive memories are both relatively common and of great personal significance in an offending population suggests that clinicians may not be accessing important information about an individual's core beliefs about the acceptability of their violence [Evans C et al. unpublished data, 2004]. As our ability to identify treatment targets improves, new challenges are likely to emerge, for example, whether intrusive memories and ruminations related to guilt should, in fact, be ‘treated’ in a violent offender.
A memory-based approach to eliciting descriptions of violent offending may also elicit clinical information relevant to violence risk assessment. The presence of intrusive memories for specific aspects of a violent offence accompanied by a credible interpretation involving guilt may be interpreted as (some) evidence that the individual has transgressed an important personal moral code. On the other hand, an individual who does not experience any intrusive memories or ruminations in relation to a specific violent incident may be of more concern clinically because this may imply a lack of discrepancy between their violence and their world view. Although such observations would be suggestive rather than conclusive, they would be supported by phenomenological detail and an indirect method of inquiry, rather than just self-serving reports to ‘obvious’ or leading questions enquiring about regret or remorse.
In conclusion, human interest in serious violence typically wanes once the perpetrator is caught [65]. The starting point for research leading to this article was a sense of intrigue about how violent offenders remember and think about their offence in the months and years that follow (Evans C: unpublished data, 2004). Our knowledge in the area of memories (or amnesia) of violent offending is lacking and focused research is likely to be clinically relevant.