
Abstract
Keywords
Dissociation describes a state of apparent disruption in the normally integrated functions of consciousness, including perception, memory and identity. Borderline personality disorder (BPD) is characterized by core features of identity confusion and unstable relationships and is commonly associated with high rates of childhood trauma and dissociation [1]. Some authors have argued that dissociation is an intrinsic component of BPD [1]. This is supported by the inclusion of dissociative symptoms as a diagnostic feature of BPD in DSM-IV. However, an alternative hypothesis holds that dissociative symptoms are coincident with BPD, develop as a defence against significant childhood trauma and persist into adulthood. We therefore examined the association between dissociation and childhood trauma in adults with BPD and investigated the relationship between specific types of trauma and dissociation.
Method
The sample comprised 139 subjects (34 male, 105 female, mean age = 32.6 years, SD = 9.6) referred to the borderline treatment team in a regional psychotherapy service. Patients were referred to the service by health-care professionals in primary and secondary care. A DSM-IV diagnosis of BPD was made based on scores on valid and reliable [2–6] self-report questionnaires – either the Personality Diagnostic Questionnaire [4] or the Screen Test for Comorbid Personality Disorder [6] and confirmed by a trained psychotherapist during a three-session assessment. There were no exclusion criteria. All patients also completed the Dissociative Experience Scale (DES) [7] and the Childhood Trauma Questionnaire (CTQ) [8]. The DES contains a number of statements such as ‘Some people have the experience of finding themselves in a place and having no idea how they got there’ and asks the respondent to circle the percentage of the time this happens to him/her. The CTQ, a 28-item self-report inventory, provides a brief, reliable history with five subscales: emotional abuse, physical abuse, sexual abuse, emotional neglect and physical neglect. It contains a number of statements, such as ‘When I was growing up I didn't have enough to eat’ and the respondent is asked to answer on a 5-point Likert scale from ‘never true’ to ‘very often true’.
Data did not fulfil the assumptions of normality and were therefore analysed non-parametrically. The median DES score was used to categorize subjects as high dissociators (n = 73) or low dissociators (n = 66). The scores of CTQ subscale were compared between high and low dissociators using Mann–Whitney U-tests (two-tailed). Relationships between scores on the CTQ subscales and DES scores were examined using Spearman's rank order correlations. All statistical analyses were performed using SPSS version 10.0 (SPSS Inc., Chicago, IL, USA). Twenty-three subjects returned incomplete CTQ scales. Within each questionnaire, scores for all completed subscales were included in the analysis.
Results
The median DES score in the group was 21.0 (95% CI = 17–25; mean = 24.09%). Over 70% of subjects demonstrated levels of emotional abuse and emotional neglect at a moderate to severe/severe to extreme level based on the normative data for CTQ scores. A significant relationship was found between CTQ subscales and DES scores for emotional abuse, physical abuse and emotional neglect, but not for sexual abuse or physical neglect. Severity of childhood abuse was significantly greater among high compared with low dissociators for emotional abuse, physical abuse, emotional neglect and physical neglect but not for sexual abuse (Table 1).
Summary table of CTQ correlation and difference values among high and low dissociators
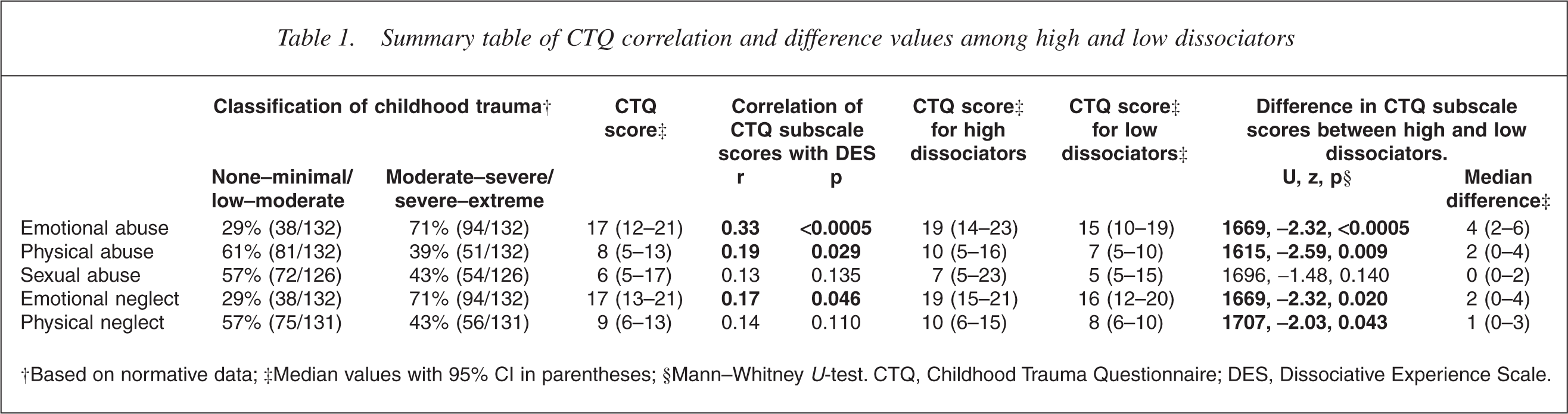
†Based on normative data; ‡Median values with 95% CI in parentheses;§Mann–WhitneyU-test. CTQ, Childhood Trauma Questionnaire; DES, Dissociative Experience Scale.
Discussion
Mean levels of dissociation are similar to those previously recorded in borderline patients [9]. Overall levels of dissociation increased with levels of childhood trauma, providing support for a putative causal relationship between traumatic experiences in childhood events and dissociative experiences in BPD. Such a relationship was further substantiated by our findings of significantly greater reported incidence of physical and emotional abuse and physical and emotional neglect among high compared with low dissociators.
The biological mechanism for the effects of sustained childhood trauma on dissociation is complex and likely to involve multiple factors. It seems likely that childhood trauma causes complex changes in neuroanatomy, neuroendocrinology and neurotransmitter sensitivity which persist into adult life. For instance, sustained childhood stress causes increased activity of the hypothalamic-pituitary-adrenal (HPA) axis which persists into adulthood [10]. Dissociation putatively reduces anxiety and the attendant HPA axis response. This thesis is supported by the negative correlation between cortisol and dissociation seen in military personnel during interrogation stress [11]. Adaptive changes secondary to the persistent, maladaptive use of this defence may explain the low cortisol levels and enhanced sensitivity of negative feedback mechanisms within the HPA axis in conditions associated with dissociation or trauma such as depersonalization disorder and post-traumatic stress disorder [12]. The amygdala is exquisitely sensitive to HPA axis perturbations [13]. Sustained childhood trauma may result in a hard-wired tendency to aggression and poor impulse regulation because such trauma may cause structural changes in the amygdala. It is possible only to speculate about the neural substrate underlying dissociation; however, overactivity in amygdala-orbitofrontal cortex circuitry represents a likely candidate and is worthy of further research.
While Freud's early papers focus on high-impact physical or sexual childhood trauma, recent psychoanalytic literature has highlighted the impact of perceived or real chronic emotional abuse and neglect on the developing personality leading to failures of ‘mentalization’ [14]. A child may dissociate as a developmental necessity to hold the self from potential breakdown and fragmentation in response to high anxiety or hyper-arousal caused not only by intrusive trauma, but also by the failure of the parents to provide an emotionally containing environment for the child. Repeated emotional trauma then has a cumulative effect and the tendency to dissociate under stress may become facilitated and habitual [15].
In our study, the strongest relationship with dissociation was found for emotional abuse. This replicates previous findings in patients with schizophrenia [16] and depersonalization disorder [17], corroborates a report that emotional abuse is a better predictor of subsequent dissociation than physical or sexual abuse among male forensic patients [18] and supports a previous study which suggested that maternal neglect may mediate the dissociative effects of physical and sexual abuse [19]. In this study, we did not demonstrate an association between childhood sexual abuse and dissociation. This may be because such abuse is usually a relatively low time frequency event when compared with a more cumulative, sustained effect of chronic emotional or physical abuse or emotional neglect [20].
Unfortunately, in the present study it was not possible to control for the presence of comorbid psychiatric diagnoses, nor abusive experiences during adulthood that may also have impacted on dissociation. In this respect, we note that dissociation is also observed in some patients with post-traumatic stress disorder [21], and the proportion of patients with this diagnosis in our study is not known.
Diagnosis was made on the basis of self-report questionnaires and a three-session diagnostic interview. Both interview and self-report diagnostic measures have poor convergent and divergent validity. This may reflect the conceptualization of personality disorders rather than the instruments per se [22]. The analysis relies on retrospective reports in adulthood of major adverse experiences in childhood. A recent review of data collection in this way suggests that false negatives are seen at a substantial rate, but false positive reports are probably rare [23]; other data suggest that the CTQ is a valid measure of abuse and neglect with good test–retest reliability [24].
We have demonstrated a relationship between childhood trauma (particularly emotional abuse) and dissociative symptoms in BPD. A similar relationship has been reported in other psychiatric conditions [16]. We suggest that rather than being an intrinsic component of BPD, dissociation and BPD may share childhood trauma as an aetiological factor. This could be further addressed in future studies designed to examine the subtleties of the expected complex interaction between the development of dissociative symptoms and borderline personality organization. The presence of a control group would also help to clarify the relationship between early abuse and dissociation and the extent to which the latter is intrinsic to BPD. Cross-sectional studies should integrate neuroendocrine and imaging data with rigorous psychodynamic assessment to more fully understand the aetiological relationships in dissociation. Prospective studies would also help to establish causality, but would require a considered design to avoid ethical and methodological constraints.
Footnotes
Acknowledgements
We are grateful to the patients, therapists and administrative staff of the Borderline Treatment Service. Ravi Lingham commented on an earlier draft of the paper.