
Abstract
Old age psychiatry's emergence as a subspecialty four decades ago stemmed from the vision of British pioneers such as Felix Post, Brice Pitt and Tom Arie that the long-stay psychogeriatric units in mental hospitals were manifestly inadequate to meet the needs of a rapidly growing aged population with complex social, psychological and medical needs [1]. Patients had previously been confined to ‘back wards’ after a limited evaluation and remained there, often till death, with little contact with psychiatrists.
Under the new regime, multidisciplinary teams were established to prevent admission to hospital wherever possible by means of home-based assessment and treatment programs, with a focus initially on dementia and chronic psychosis. Patients with particularly complex problems were admitted initially to short-stay assessment units and only those with severe, intractable conditions were moved to long-stay wards. Great emphasis was attached to accurate diagnosis; assertive treatment of reversible medical and psychiatric conditions; support to carers; and collaboration with general practitioners, geriatricians, residential facilities and social services. This model proved so useful that eventually British aged psychiatry services assumed responsibility for the care of all older patients, including those with affective disorders and late-onset psychoses.
Australian and New Zealand psychiatrists adopted this approach quickly, with the result that community teams and acute assessment units grew in number from the 1970s onwards. In 1987, specialists formed a Section of Psychiatry of Old Age within the Royal Australian and New Zealand College of Psychiatrists to advocate for older people and to encourage service development by promoting professional contacts and auspicing scientific meetings. The Section was promoted to Faculty status in 1999 and currently has over 200 members in both countries and nearly 60 advanced trainees. Membership of the Faculty now requires completion of a 2-year training program in an accredited centre.
The kind of multidisciplinary, community-focused care espoused by ‘old age’ psychiatrists generally works best in publicly funded settings. While Australian private psychiatrists see large numbers of older people, and a few private psychiatric hospitals have dedicated psychogeriatric units, older adults in 1998 received only a quarter of the Medicare-rebated psychiatric consultations provided on a per capita basis to younger ones [2]. Similar findings emerged from an earlier analysis in 1999 [3]. Frail, multiply handicapped elderly people have diffi- culty accessing office-based private practitioners, with the result that referrals are mostly directed to public sector services, whether generalist or specialist in nature. In New Zealand, where health insurance payments are limited for geriatric or psychiatric consultations, private aged psychiatry services are modest and confined to a couple of major centres.
For reasons of history, public mental health services in Australia are funded not by the federal government but by individual states and territories whose budgets vary greatly. In 1998, Western Australia, for example, expended 31% more per capita than Queensland on mental health services in general and 153% more on aged psychiatry [4], p.23. New Zealand services are not uniform either. Extensive health sector reforms there led to responsibility shifting from Area Health Boards to Regional Health Authorities, then back to District Health Authorities. As a result, about half the country's aged psychiatry services were amalgamated with geriatric medicine and the rest with adult mental health [5]. Notwithstanding this, District Health Authorities are required to provide aged mental health services that fit with nationally promulgated policies and guidelines [6–8].
Of all Australian states, Victoria was the first to articulate a policy dictating the funding, composition and distribution of child, adult and aged public mental health services. This policy, which stipulated that services should be distributed equitably based on local population size weighted for socioeconomic vulnerability, led to the replacement of large mental hospitals with multidisciplinary community teams and inpatient units linked to local health care networks [9]. Victoria also took the initiative in converting its long-stay psychogeriatric wards to purpose-built, federally subsidized specialist nursing homes with state government top-up. The need for dedicated services for older people was never in doubt in this massive, and fundamentally successful, service realignment [10]. Old age psychiatry has grown in other states too but in a patchier fashion with varying funding and governance arrangements.
Members of the Faculty of Psychiatry of Old Age contribute to state, territory and national planning deliberations, but their input is hampered by a lack of accurate information about current service provision. The survey outlined here, which was conceived and funded by the Faculty, aimed to furnish accurate data to clinicians, academics and administrators about the state of affairs in both countries in 2003. Its objective was to identify every dedicated, publicly funded aged psychiatry service, no matter how small, and to provide a snapshot view of staff, physical resources and clinical activity. This apparently simple task proved more difficult than expected.
Method
We drafted a brief structured questionnaire enquiring into the numbers of publicly funded acute, subacute and residential aged psychiatry beds, the numbers of staff in acute inpatient and community aged psychiatry services and the numbers of registered aged community patients in 2003.
A covering letter defined an aged psychiatry service as follows. With respect to staff, we included professionals who worked exclusively with older mentally disordered people, even if only part-time. Thus, we included a community nurse funded by an aged care agency who visited elderly people with a range of mental disorders for one afternoon a week. Conversely, we excluded a psychiatrist caring for a mixture of young and old people with no special time dedicated to the latter. With respect to facilities, we sought information on acute beds, subacute (i.e. rehabilitation, slow-stream or long-stay) hospital beds and residential beds to which aged psychiatry clinicians admitted patients or residents under their personal supervision. This definition included beds occupied by elderly people on a general psychiatry ward or nursing home unit provided that care was supervised by a psychogeriatrician (not necessarily a Faculty member) but excluded the ones supervised primarily by a general psychiatrist, geriatrician or general practitioner. Where bed numbers varied, we asked what numbers had been occupied typically by elderly people in the previous year. We included all specialist services, irrespective of size or source of funding. Some were very small (e.g. a visit to a town once a month by a psychiatrist or community nurse), others were much larger.
Survey forms were distributed to state representatives of the Faculty of Psychiatry of Old Age together with service directors and managers known to the authors and also persons and agencies identified through national and state government publications and electronic searches. Over a period of several months, we established a network of respondents who told us of clinicians and teams known to them. All avenues were explored by means of 200 or so telephone calls and more than 600 email messages until we were certain that every service that met our definition had been identified. Once forms were returned, all missing, inconsistent or anomalous entries were resolved to our satisfaction.
The resources allocated to services by territories, states and countries must be set in the context of the size and distribution of their aged populations. Relevant details were sourced from the most recent census reports in Australia [11] and New Zealand [12].
Results
Aged populations
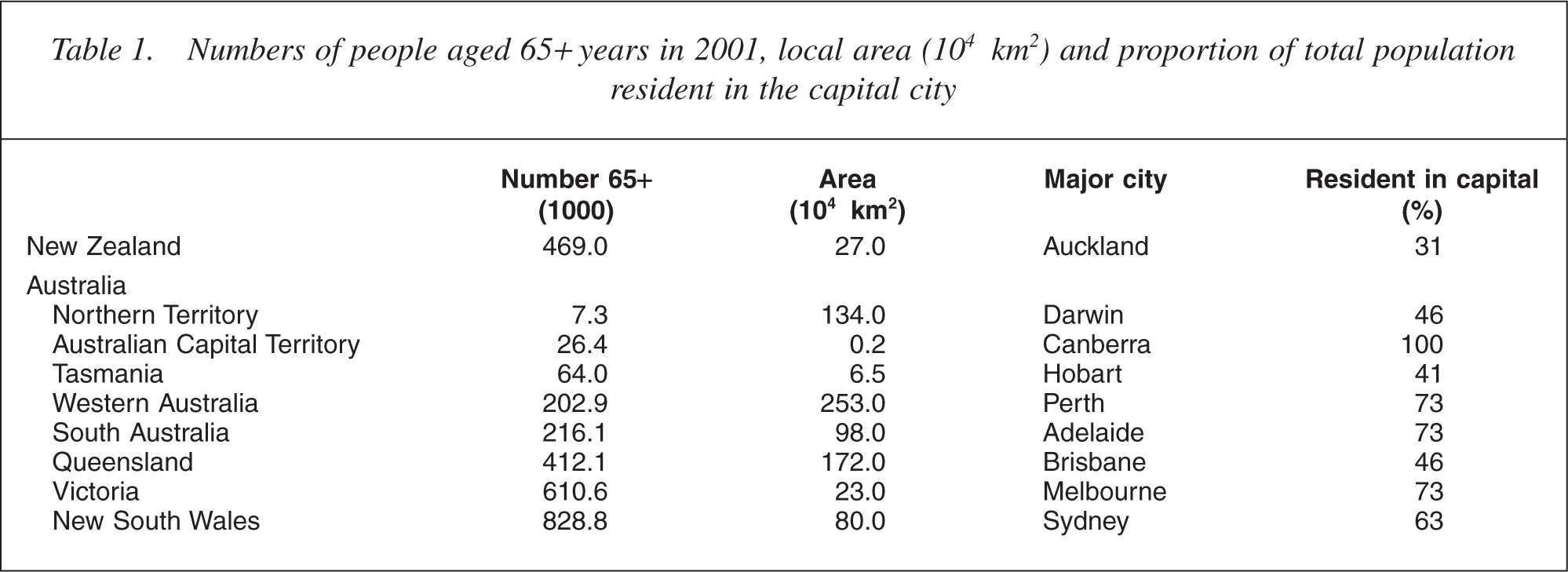
Table 1 lists the numbers of people aged 65 + years together with each jurisdiction's geographical area and the proportion of people resident in the local capital city. The contrasts are striking. Victoria had almost as many older residents as New South Wales, but is only a quarter its size. Western Australia is three times larger than New South Wales but had only a quarter its aged population. Queensland had twice as many aged people as Western Australia and they are dispersed more widely. Tasmania, at the other extreme, is tiny and the Northern Territory, while huge in size, had a negligible aged population. New Zealand is different again. Its substantial older population, equivalent in size to Queensland's, is widely dispersed with only one-tenth of its people resident in the national capital.
Numbers of people aged 65 + years in 2001, local area (104 km2) and proportion of total population resident in the capital city
Services
Table 2 shows the number and size of specialist services in each jurisdiction. The number of services, when adjusted for aged populations, was relatively uniform with two exceptions. South Australia, a large but sparsely populated state, had only two services, both in Adelaide. By contrast, Western Australia, a much larger state with a similar aged population, had seven times more services with one-fifth of them located in regional centres.
The numbers of services with adjustments for local populations, and numbers of EFT staff excluding residential care staff
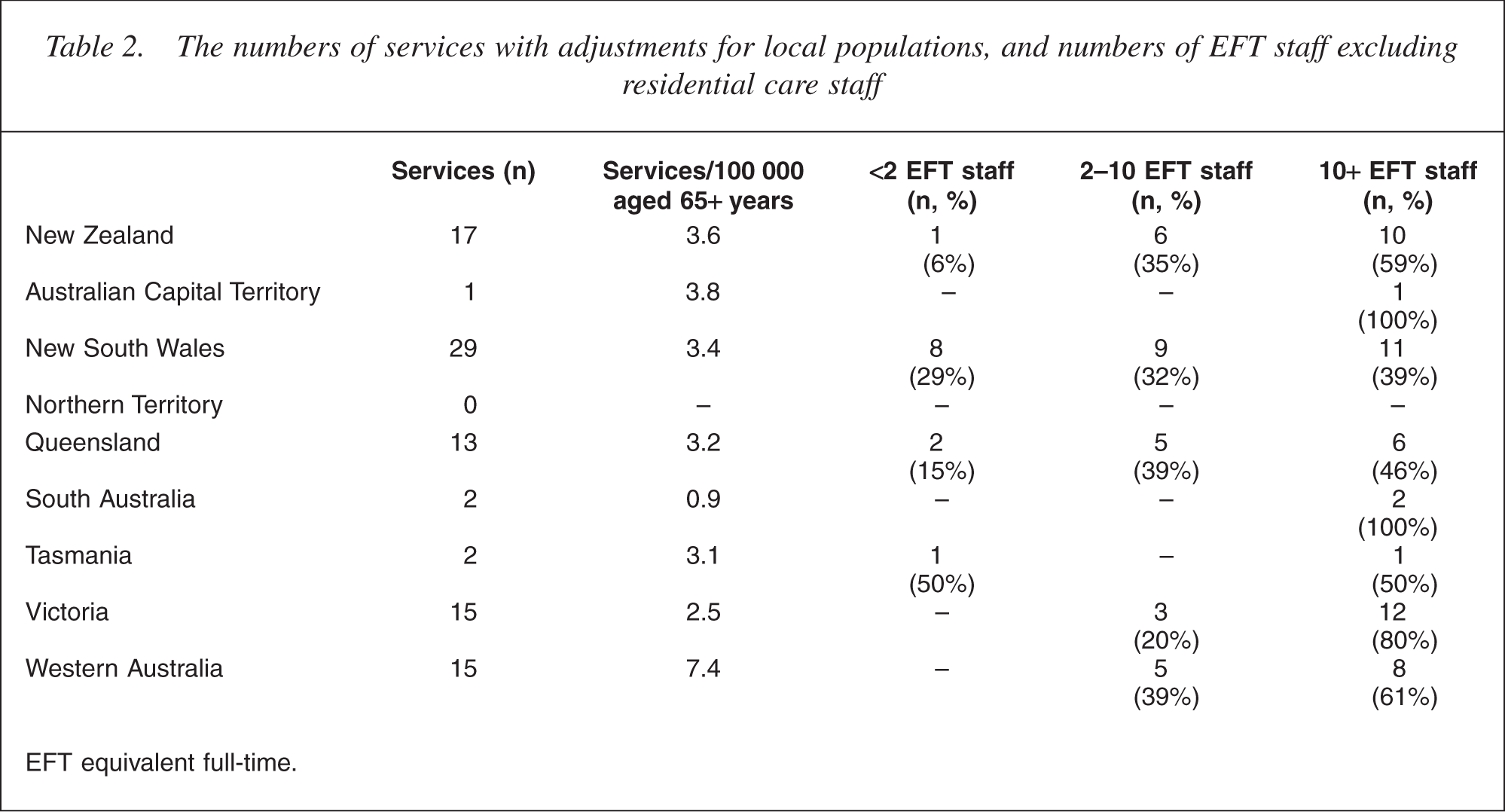
Services varied greatly in size. While New South Wales, the most populous state, had the largest number of services, almost a third were comprised just of a psychiatrist who flew in and out by plane for 1 day or so, some with part-time support from a nurse. The contrast with Victoria was striking. The latter state has a slightly smaller aged population, but 80% of its services were comprised of 10 or more equivalent full-time persons compared with 39% in New South Wales.
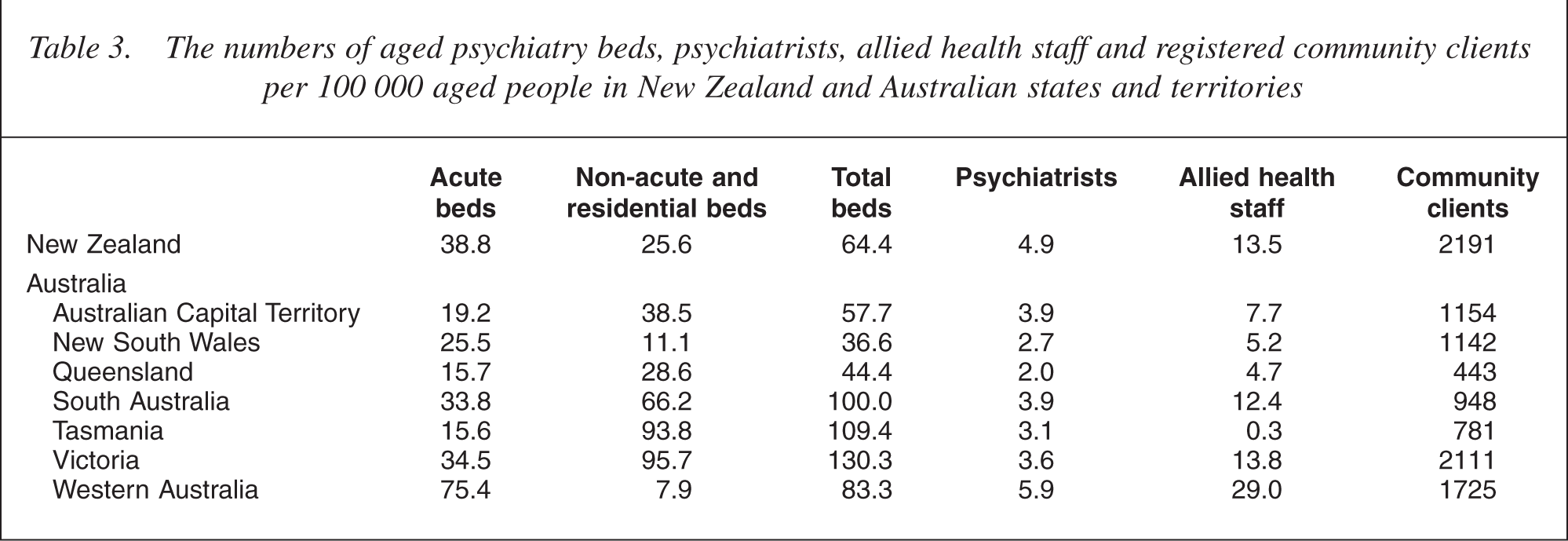
Table 3 lists the numbers of dedicated aged acute, non-acute and residential mental health beds; the numbers of equivalent full-time psychiatrists, allied health staff and nursing staff (excluding those in specialist residential facilities) working exclusively with aged inpatient and community patients, and the numbers of aged patients, all adjusted for local aged populations. Queensland and Tasmania had very low numbers of acute beds in contrast to Western Australia. Other jurisdictions occupied intermediate positions. With respect to non-acute and residential beds, New South Wales and Western Australia had low numbers in contrast to Tasmania and Victoria. Taken overall, South Australia, Tasmania and Victoria had the largest bed capacity. New South Wales and Queensland had the lowest.
The numbers of aged psychiatry beds, psychiatrists, allied health staff and registered community clients per 100 000 aged people in New Zealand and Australian states and territories
Admitting arrangements varied greatly. All aged psychiatry services in Victoria and South Australia had access to their own acute beds. By contrast, patients had to be transported to beds in another sector in 23% of services in Queensland, 29% in both New South Wales and New Zealand, 31% in Western Australia and 50% in Tasmania. Conversely, the proportions of services with their own self-contained aged psychiatry wards were as follows: Queensland 15%, New South Wales 29%, Tasmania 50%, Western Australia 54%, New Zealand 59%, Victoria 60% and South Australia 100%. Note that Tasmania and South Australia had only two services each.
Numbers of equivalent full-time psychiatrists, when adjusted for aged populations, were more uniform. Figures were highest in Western Australia and lowest in Queensland, but contact times were often low. All aged psychiatry services in Victoria, Tasmania and South Australia had access to a psychiatrist for at least half a day a week. The proportions of services in other states that lacked this level of access were as follows: New Zealand 12%, Queensland and Western Australia 15% and New South Wales 29%.
Numbers of nursing staff were so much higher in states with large numbers of residential beds that comparisons are meaningless. The provision of allied health staff (psychologists, social workers, occupational therapists, etc.) was most generous in Western Australia, Victoria and New Zealand and leanest in Tasmania.
The adjusted numbers of registered patients seen in the previous year varied greatly from place to place. New Zealand led the way followed closely by Victoria and Western Australia. Rates were much lower in Queensland, Tasmania and South Australia.
Discussion
Our findings derived from diligent, systematic enquiries of well-informed psychiatrists, service managers and government officers and we are confident that we identified every specialist, publicly funded aged psychiatry service in place in 2003 irrespective of size or source of funding. It is reassuring that the numbers of beds reported here fit closely with those listed in the most recent Australian Government National Mental Health Report [13], p.28 with the proviso that we identified more acute beds in Western Australia (75.4 per 100 000 aged people compared with 55.8 in the Government report) and fewer non-acute and residential beds in New South Wales (9.2 compared with 34.3). The latter discrepancy stemmed from our judgement that most of the state's so-called ‘confused and disturbed elderly units’ failed to meet our criteria for mental health facilities.
Victoria was the only Australian state to provide specialist, multidisciplinary aged psychiatry teams with community, acute inpatient and residential arms in all its major towns. In other states, services were based mostly in capital cities with limited coverage to regional and rural areas. To be fair, Victoria is so compact and highly urbanized that equitable coverage is relatively straightforward. Large jurisdictions with highly dispersed populations like Queensland and New Zealand are much more challenging. States like South Australia and Western Australia lie somewhere in-between. While vast in size, their populations are restricted to modest numbers of fairly compact centres and specialist coverage is therefore more practicable than appears at first sight.
New South Wales, the state with the largest aged population, performed relatively poorly on most indicators. Its many ‘services’ were often comprised just of a psychiatrist visiting briefly from Sydney; its total bed numbers were low and often distant from patients' homes, and its adjusted community contact rates were two-thirds the number of Victoria's. It became clear while conducting the survey that area mental health services in New South Wales operated autonomously with little if any knowledge of their neighbours' activities. Matters are likely to change now that areas have been reduced in number and a position dedicated to old age mental health issues has been created in the state's Department of Health.
Services in other states varied considerably. South Australia's larger-than-average stock of acute and nonacute beds was confined to Adelaide and its community contacts were relatively low. Queensland's bed provision, while smaller, was more broadly distributed, but community penetration was the lowest of any jurisdiction. Western Australia had generous numbers of acute beds, almost all in Perth, and widespread community activity but very few specialist residential beds. New Zealand, which has about as many older people as Queensland, had widely dispersed services with relatively good numbers of beds and psychiatrists and excellent community penetration.
Older people with serious psychological or behavioural disorders also receive support from private psychiatrists and private psychiatric hospitals in Australia (where they exist). As noted already, private practitioners' offices are based mostly in the wealthier suburbs of major eastern Australian cities and offer little if any access to frail, confused old people and residents of regional and rural areas [2,3].
Public ‘adult’ mental health teams are more accessible and equitably distributed than private services, but mapping their contacts with aged people was beyond our capacity. They certainly treat older patients with established affective disorders and psychoses and doubtless assist many thousands of patients and carers. There is evidence, however, that specialist aged psychiatry services produce better outcomes for certain older people, in particular the frail, housebound aged and residents of aged care facilities; those with mixed organic and functional mental disorders and those whose dementia is complicated by behavioural or psychological symptoms [14]. Such people command few resources in deprived areas where public attention is focused so strongly on younger and middle-aged groups. This shifts responsibility to general practitioners and aged care assessment teams whose expertise in diagnosis and treatment is probably limited.
North American and Australian studies show that aged psychiatry teams conduct more detailed evaluations of older patients, and monitor their progress more scrupulously, than generic services [15] and do better at treating depression [16]. Australian services are rated highly by carers and referring agents [17–19] and local randomized controlled trials confirm the effectiveness of multidisciplinary input to nursing home residents with dementia [20,21]. Psychiatrists in Victoria, New South Wales and the Australian Capital Territory have all described the wide range of conditions they treat, their close relationships with other aged care providers and their strong research and educational commitment [19,22,23].
Aged psychiatry is now an established subdiscipline in Australia and New Zealand. This makes sense: both countries face huge increases in the numbers of very old people, including those with dementia [24]. Its strength lies in its capacity to respond to frail, housebound older people with functional mental disorders and to the minority of those whose dementia is complicated by debilitating psychological and behavioural symptoms [25]. This perceived advantage should be exposed to scientific scrutiny. From an epidemiological viewpoint, it would be of interest to compare similarly sized regional centres with and without aged psychiatry services in respect to their aged clientele, the numbers of visits to aged residential facilities and the numbers of patients with dementia. From a clinical viewpoint, outcomes can be compared prospectively of older patients with affective disorders and psychosis treated by generalist and specialist teams.
Our survey is a mapping exercise, intended to provide essential information to those responsible for planning mental health services in Australia and New Zealand in coming years. It consumed many dozens of hours and was conducted with great rigor. We freely acknowledge its limitations but trust that our findings will prove useful.
Footnotes
Acknowledgements
The following people kindly provided information regarding their services: Adesina Adesanya, Megan Alle, George Atartis, Martin Atkins, Stergia Avgoulis, Jeanette Best, Ravi Bhat, Mike Bird, Richard Bonwick, Leesa Bradshaw, Neridah Brinkley, Sarah Brooker, Gerard Byrne, Margaret Chapman, Sudarshan Chawla, Brett Coulson, Ed Darby, Alison Davamoni, Sandra Davidson, Anthony Devis, John Dobrohotoff, Brian Draper, Anthony Duncan, Crawford Duncan, Noel Fernando, Dawn Fisher, Mark Fisher, Jenny Fowler, Kuruvilla George, David Grace, Liz Goyer, Mark Henson, Laurence Herst, Trevor Hollingsworth, Ian Hosford, Sandie Kirkman, David Kitching, Lana Kossoff, Robert Llewellyn-Jones, David Lie, Margaret Lowndes, Caroline Luke, Christine McDougall, Bede McIvor, Rod McKay, Daryl McMahon, Martin Morrissey, Paul O'Hara, Carol Onley, Anne Osman, Sue Pacey, Sally Perks, Jill Pettigrew, Gavin Pilkington, Russell Porter, Judy Raymond, Sam Restifo, Kerri Rivett, Bob Russell, Peter Ryan, Geoff Siedel, AnneLise Siefert, Barbara Simons, Simon Stafrace, John Snowdon, Jon Spear, Danny Stone, Doug Subau, Stephen Swartz, Edward Tan, Brent Thomas, Jacinta Thompson, Sandra Thomson, Stephen Ticehurst, Toni van Hammond, Sandy Wallis, LS Wettasinghe, Chanaka Wijeratne, Sid Williams, Greg Young, Rasiah Yuvarajan. We also thank David Ames, Brian Draper, David Lie and Rod McKay for helpful comments on an earlier draft of this paper.