
Abstract
An increasing focus on early intervention in psychiatry [1, 2] underscores the importance of identifying delays in help-seeking and referral for those with mental health problems. Goldberg and Huxley [3] identified the sequential filters to help-seeking pathways that may account for delays in treatment. Individual, family, social and cultural factors all may be relevant in determining if and when help is sought and who is consulted. In Australia, preliminary evidence has suggested that membership of ethnic minorities may influence the pathways leading to psychiatric services [4–6]. McDonald and Steel [5] found that Vietnamese-, Arabic- and Chinese-speaking immigrants were less likely than Australian-born to use specialist psychiatric care, but little is known about the delays or obstacles involved.
Gater et al. [7] examined the pathways to care for patients presenting for mental health across 11 countries. Pathways varied by disorder, with longer delays associated with non-psychotic disorders, somatic problems and referrals by non-medical practitioners. Although other international studies have supported the finding that ethnicity [8–11] influences time and mode taken to reach mental health services, other factors, including severity of symptoms [12], the nature and extent of social support networks [13–15], social disadvantage [16, 17] and concepts of illness held by patients [18–20], each play a role.
Methodological limitations of past research make it difficult to draw definitive conclusions about the factors delaying help-seeking behaviour [8]. Most studies 21– [28] have not distinguished between patients making their first contact with mental health services and those with previous contact. Pathways to first lifetime contact may be critical to developing models of engagement in early intervention programs. This limitation has been addressed to some extent by research examining pathways to care for first episode psychosis [29–31]. Nevertheless, while psychosis represents an important component of the caseload of specialist mental health services, the principles of early intervention are relevant to a broader array of mental health problems [32].
The present study examined a heterogenous group of patients making their first lifetime contact with community- or hospital-based mental health services with responsibility for an entire geographical catchment area. Our objective was to investigate whether pathways were influenced by illness type and severity; patient characteristics such as age, gender, education, social support, ethnicity and illness explanatory models; and the structure of health and mental health services.
Method
Sample
All consecutive patients 18–65 years old and born in Australia, Vietnam or a Chinese- or Arabic-speaking country presenting for the first time to public mental health services in two geographical catchment regions of Greater Western Sydney (Bankstown and Western Sydney) formed the target group. The relevant ethnic groups are the largest minorities in the catchment areas and all three appear to underutilize services [5, 33]. The first stage involved identifying all consecutive patients referred or admitted to one of eight community-based mental health services or four acute inpatient psychiatric units across the study period which lasted for approximately 6 months at each site. Patients were included if they were admitted to the service – in effect this means that a case file for the patient was opened, whether or not the patient was subsequently lost to follow-up.
A total of 429 patients presented to services during the study period. Of these, 95 (22%) could not be contacted for the research interview, with a further 63 (15%) refusing to participate, representing an inclusion response rate of 63%. One hundred and twenty-five reported a previous episode involving contact with a specialist mental health service. The present study focuses on the remaining 146 who had no previous contact with private or public mental health services. Patients who had a first contact with a private psychiatrist in the previous 12 months were also included in the first-contact group (n = 22). Eighty-two (56%) were interviewed at a hospital inpatient facility and 64 (44%) in a community setting. A diagnosis of psychotic disorder was made in 75 (51%) and a non-psychotic disorder in 71 (49%). There were 84 men (57%) and 62 women (43%) with an average age of 33 years (range 15–64, SD = 11). Eighty (55%) of the patients were from an English-speaking background, 25 (17%) from Arabic, 27 (18%) from Chinese and 14 (10%) from a Vietnamese background. A number of the Chinese-speaking had been born in Vietnam (30%), so we collapsed the latter two Asian groups into one composite group.
Measures
Semistructured interview
The semistructured interview assessed help-seeking behaviours and referral pathways of participants based on the Encounter Form developed by the World Health Organization [7]. For each of the major steps in the referral process, retrospective information was collected on the professional seen, the approximate timing of consultations, the language used, the referral source, the presenting problem and the treatments or services offered. The timing of first onset of psychiatric symptoms was estimated through clinical interview based on patient self-recognition or observations by others. Additional questions were included to assess patient perceptions of the causes of their problems, including: physical causes (e.g. physical illness, somatic explanation); environmental problems (e.g. nothing to do, unemployment, interpersonal conflict); problems related to habits (e.g. lifestyle problems); psychological problems (e.g. stress, anxiety, depression); psychiatric problems (a specific diagnosis); supernatural problems; or symptoms as a result of a curse or punishment [34]; the nature and extent of social support networks [35]; and the self-rated level of acculturation using the method developed by Ranieri et al. [36]
File audits
A file audit of clinical records yielded general demographic and clinical information such as date of first presentation, descriptions of presenting problems, the degree of clinical severity, primary and secondary diagnoses, treatments received and/or referral decisions.
Health of the Nations Outcome Scales (HoNOS)
The HoNOS consists of 12 items that rate the degree of impairment in behavioural, emotional and social domains among people with a mental illness [37]. The 12 scales yield scores of 0–4, producing a maximum total score of 48. The HoNOS is completed by a trained mental health care practitioner, with ratings being made on the basis of all available information from routine clinical assessment [37, 38].
Procedure
Interviews were arranged by the assessing mental health worker for a location suitable to the patient. Verbal informed consent was obtained by the case worker and subsequently by the research assistant. For patients from ethnic minorities, a choice of language (English, ethnic language) was offered, and when appropriate, a trained mental health bilingual worker undertook the interview. The inpatient file audits were completed after discharge. Ethics approval for the project was obtained from the Western Sydney Area Health Service and the South Western Sydney Area Health Service.
Analyses
Time taken to reach services showed a skewed distribution so that median time in months was estimated. Differences in time were calculated using the Mann–Whitney test. Associations between time and other quantitative variables were examined using Spearman's rho correlation. Means, standard deviations and parametric statistical tests were applied to other variables such as the number of professionals consulted and the HoNOS scores, where the distribution was approximately bivariate normal.
Results
Pathways to care
Figure 1 depicts the various help-seeking pathways leading to first contact with mental health services. The mean number of professionals consulted prior to the index contact was three (SD = 1.3) with 87% making at least one and 60% making at least two consultations regarding their mental health concerns before reaching specialist mental health services. General practitioners (GPs) played a pivotal role in the help-seeking consultation pathways with 45% of patients presenting initially to a GP and 53% consulting with one at some time about their mental health problems. Following GPs, the order of frequency of first presentations were: direct to specialist mental health services (13%), hospital emergency departments (12%), police (11%) and allied health professionals (10%). Only 5% of participants first consulted a traditional healer, alternative medicine practitioner or religious leader, with 15% first consulting a non-health professional, such as a teacher or a welfare worker.
Pathways to specialist mental health care (n =146). GP, general practitioner.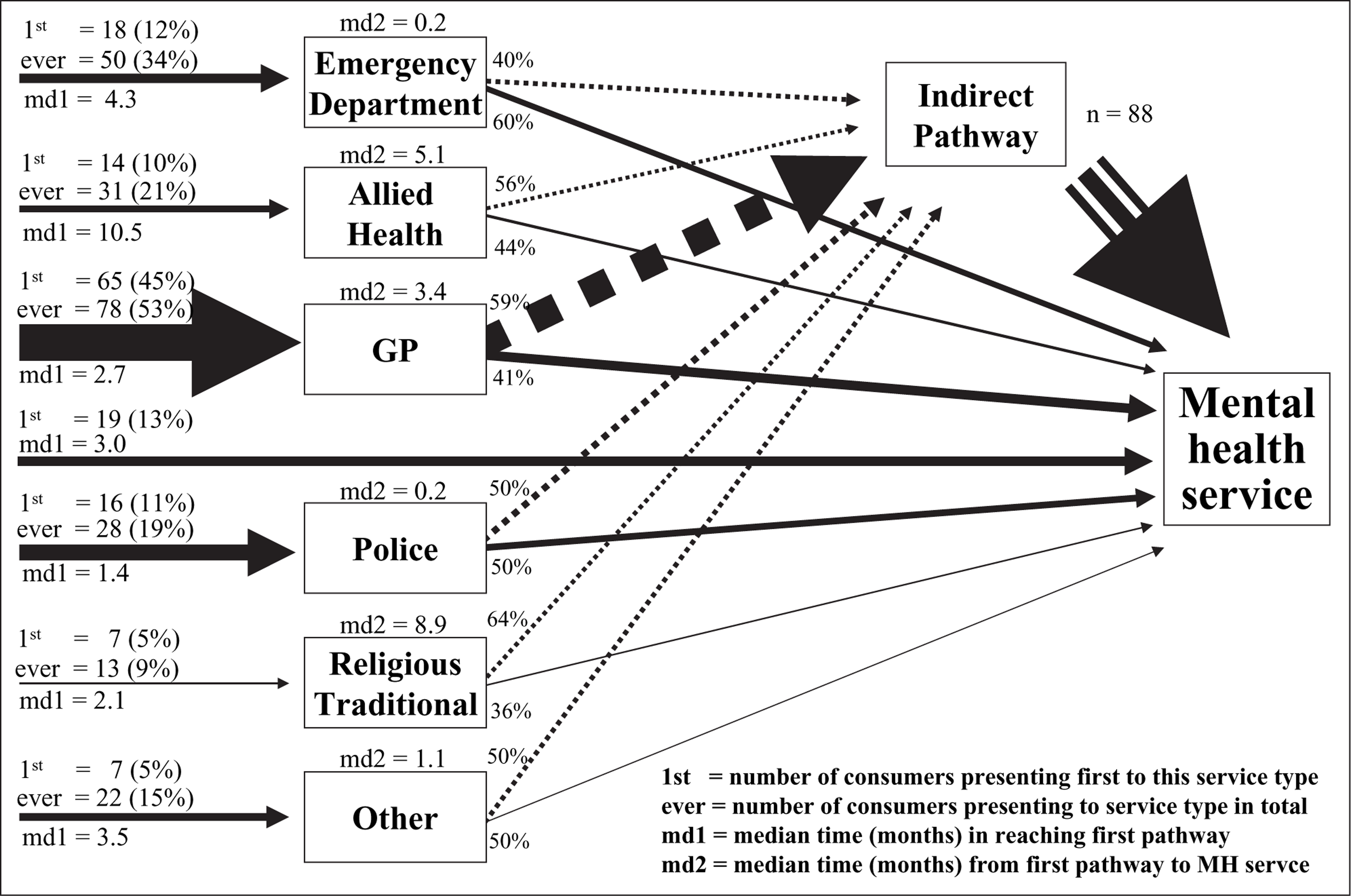
Time taken to reach mental health services
The median time taken to reach specialist mental health services was 6.3 months (range 1 week to 24 years). The median time to initial contact with the first generic professional was 2.9 months (interquartile range 1 week to 9 years). Over 25% of the sample reached public mental health care in less than 2 months, but 25% took over 2 years to reach care. The professional category of contact influenced the time taken to reach mental health care. The median time to reaching specialist mental health services after police involvement or after presenting to an emergency department was approximately 1 week, which was significantly lower than the median time taken after consulting with a GP (3.4 months, p < 0.001), allied health professional (5.1 months, p < 0.01) or a traditional healer, alternative medicine practitioner or religious leader (8.9 months, p < 0.01).
Gender, age and educational level did not affect time taken to reach mental health care. Patients living with both a partner and children had a longer help-seeking pathway (median = 9 months) than those in other living arrangements (median = 6 months, p = 0.32).
Influence of symptom severity and diagnosis on pathways to care
Table 1 presents the HoNOS mean total and subscale scores obtained for the 146 first-contact patients. The HoNOS total and subscales scores did not influence the median time taken to reach mental health services (r = −0.014) or type of professional consultations made prior to contact. Higher HoNOS total scores was associated with a greater number of professional consultations (r = 0.20) particularly for those patients with elevated impairment (r = 0.216) or symptom severity (r = 0.225) subscale scores.
Mean (SD) HoNOS total and subscale scores for the 146 first-contact mental health patients
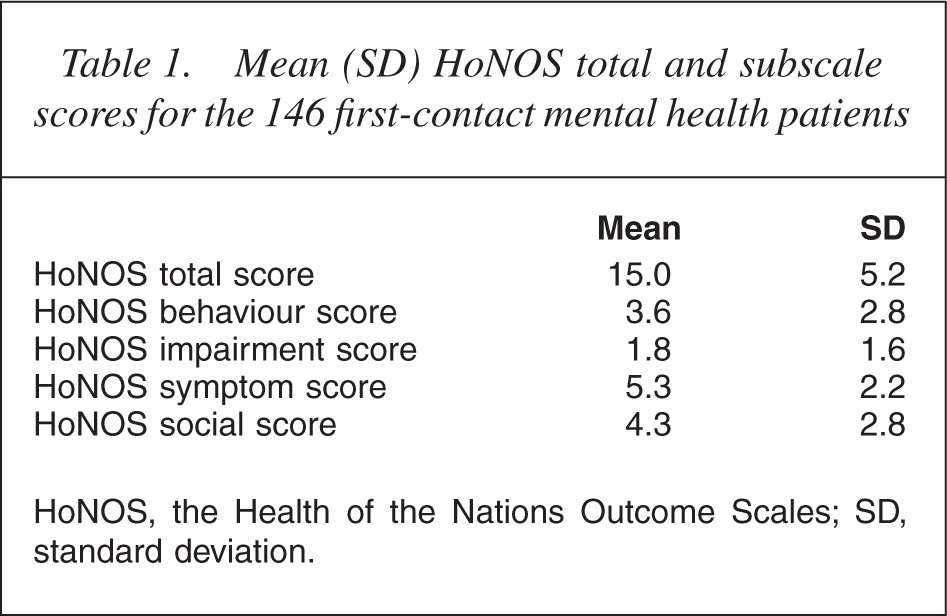
HoNOS, the Health of the Nations Outcome Scales; SD, standard deviation.
Patients with psychotic (mean = 15.4, SD = 5.0, n = 75) and nonpsychotic disorders (mean = 14.5, SD = 5.4, n = 71) did not differ on HoNOS scores (p < 0.05). Patients with a psychotic disorder were more likely to present directly to public mental health services (20% vs 6%, p < 0.01) and to have contact with the police (29% vs 8%, p < 0.001). Patients with a non-psychotic disorder were more likely to consult a GP (62% vs 45%, p = 0.04), allied health professional (30% vs 13%, p = 0.016) or a non-health professional such as a teacher or welfare worker (21% vs 9%, p = 0.046).
A shorter median time taken to reach mental health services was found for patients with a psychotic disorder (4.5 months vs 9.2 months, p = 0.03). This was not due to a difference in the time taken to reach the first professional carer but rather to the time that elapsed thereafter (psychotic median delay after first consultation = 2 weeks; nonpsychotic median delay = 3 months; p = 0.002).
Influence of facility type on pathways to care
No differences were evident in time taken to reach inpatient or community care. Sixty-six per cent (n = 50) of patients with a psychotic disorder had their first mental health contact at a hospital inpatient setting compared with 46% (n = 32) of patients with a non-psychotic illness (p = 0.011). Hospital presentations had higher HoNOS total scores (mean = 16.3, SD = 5.5) than those treated in the community (mean = 13.1, SD = 4.2) (p < 0.001). The consultation pathways displayed by those admitted to an inpatient facility involved more contact with emergency services (60% vs 14%, p < 0.001) and contact with the police (27% vs 9%, p = 0.009). In contrast, those treated in a community setting were more likely to have consulted a GP (64% vs 48%, 2= 6.8, df = 1, p = 0.009).
Influence of explanatory models on help-seeking patterns
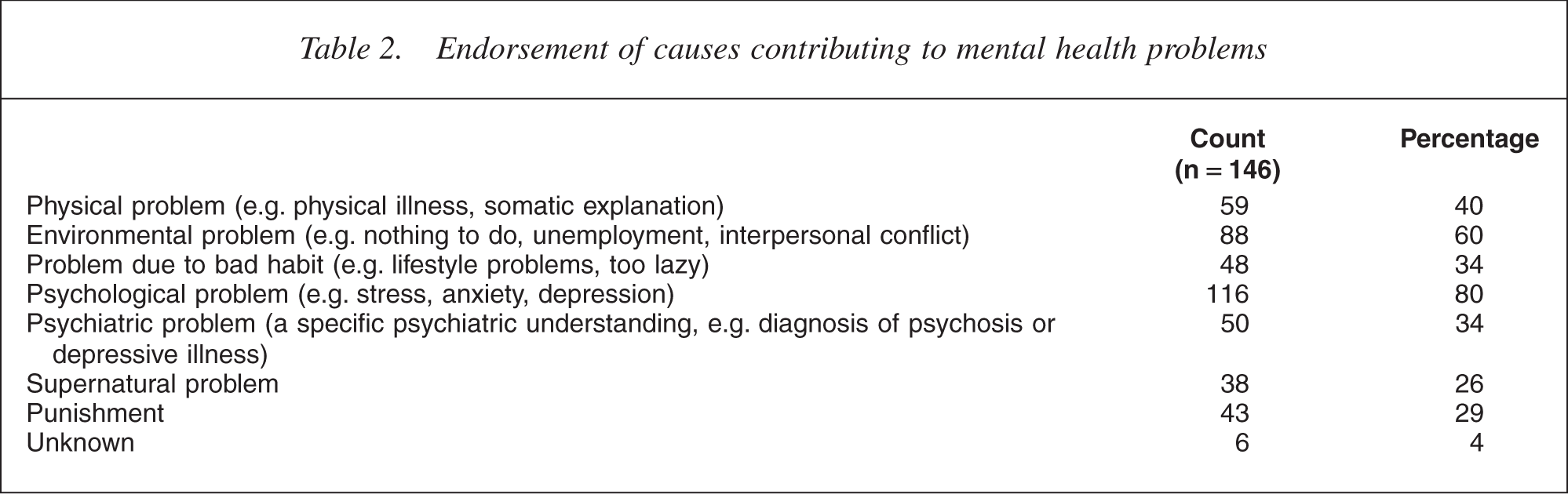
Patients endorsing a supernatural explanation (Table 2) were more likely to consult with a religious leader, traditional healer or alternative medicine practitioner (p = 0.01), to have police involvement (p = 0.006) and to visit an emergency department (p = 0.01). They also had higher HoNOS total scores (supernatural endorsed, mean HoNOS = 16.7, SD = 6.2; remainder = 14.4, SD = 4.7; p = 0.018) and were more likely to be diagnosed with a psychotic illness (p < 0.001). Patients who believed that their problems were due to bad habits were less likely to consult a GP (p = 0.04) or visit an emergency department (p = 0.04).
Endorsement of causes contributing to mental health problems
Influence of social support on help-seeking patterns
Three indices of social support were extracted from the semistructured interview: (i) total number of support people; (ii) number of support people in weekly contact with the patient; and (iii) total number of support people who were identified as confidantes. The average number of support people identified was five (range 0–14). The average number of people in weekly contact was 3.8 (range 0–11), with an average of 3.4 people (range 0–12) regarded as confidantes. There was no association between any index of social support and the number of professional consultations or the median time taken to reach mental health services. Number of support people in weekly contact (p < 0.01) and number of confidantes (p < 0.005) were each associated with lower HoNOS total scores. Patients with a greater number of support people (p < 0.05) or support people in weekly contact (p < 0.05) were more likely to consult an allied health professional. Patients with a lower number of support people (p < 0.05) or a lower number of confidantes (p < 0.01) were more likely to have contact with emergency departments.
Ethnicity, English flency and acculturation
There was no observed difference between the number of prior consultations or the time taken to reach mental health care across Asian, Arabic-speaking and Australian-born groups. The three groups did not differ in the proportion of those with a psychotic illness. Patients from an Arabic background had higher HoNOS total scores (mean = 16.8, SD = 5.1) than Australian-born patients (mean = 14.0, SD = 5) with those of Asian background occupying an intermediate position (mean = 15.8, SD = 5) (p = 0.038).
The three groups displayed a number of differences in the pathways they took to reach specialist services. The Arabic-speaking were more likely to consult a GP (76%) than either the Australian-born (47%, p = 0.01) or Asian (51%, p = 0.04) groups. Asian patients were less likely to consult an allied health professional (10%) than the Australian-born (29%, p = 0.02). The three groups did not differ in their endorsement of explanatory models.
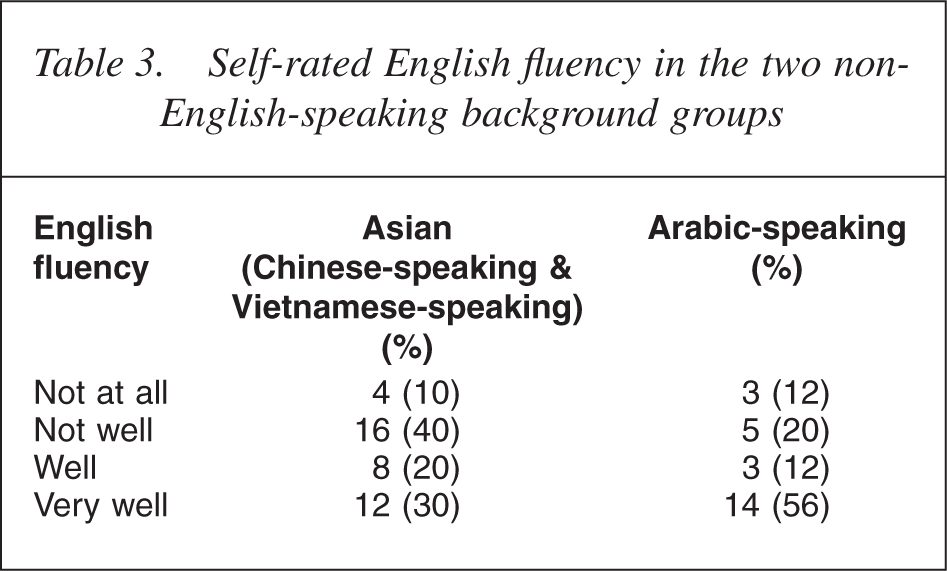
English flency was not associated with symptom severity as assessed by the HoNOS (t = 0.45, df = 62, p < 0.05) nor with likelihood of a psychotic illness (χ2= 1.1, df = 1, p < 0.05). There was no difference in the total number of professional consultations by level of English flency (t = 0.4, df = 60, p < 0.05), but poor English flency was associated with lower likelihood of consulting an allied health professional (χ2= 6.5, df = 1, p = 0.01). Patients with poorer English flency had a shorter median time (3.5 months) for reaching mental health services than patients with better English flency (Table 3).
Self-rated English flency in the two non-English-speaking background groups
Acculturation scores were similar among Arabic and Asian groups (χ2= 1.4, df = 1, p < 0.05). There was a strong correlation between selfrated English flency and level of acculturation (rho = 0.65). Acculturation scores were not associated with total number of professional consultations, time in reaching mental health care, diagnosis, symptom severity or consulting pathways.
Discussion
As in previous research [7, 12, 21, 22, 30], the GP emerged as the most common point of contact on the pathway to specialist mental health care. At the same time, participants exhibited a wide range of consulting pathways, with 60% having contact with two or more professionals. Lincoln et al. [31] and Hirst et al. [25] reported a similar diversity in the pathways pursued by patients making their first contact with mental health services. In the present study, the median time taken to reach mental health services was 6.3 months. However, there was a wide degree of variation across the sample with over 25% of respondents reaching care in under 2 months and a similar proportion taking over 2 years to reach care.
Having a psychotic disorder was associated with a shorter delay in reaching care, particularly once an initial professional consultation had occurred. The observed median time of 4.5 months was similar to the 4 months reported by Lincoln et al. [31] among a sample of 62 young people with first onset psychosis. In the multisite study of Gater et al. [7], psychotic disorder also predicted shorter time to reaching mental care at a number of sites. The Health of the Nations Outcome Scales scores were similar across the psychotic and non-psychotic groups and severity of symptoms did not predict time to reaching care or the number of professional consultations made. These results confirm the observation of Lincoln et al. [31] that psychotic symptoms, particularly of a florid nature, may attract intervention because of the bizarre nature of the condition rather than because of the severity of the illness. More of the patients with a psychotic condition were in contact with police, a pathway that was associated with a shorter pathway to reaching mental health care. As would be anticipated, admitted patients had greater symptom severity and this appeared to be the only robust predictor of whether community or hospital care was offered in the first instance.
Previous studies have underlined the importance of social networks on the pathways taken to reach care [30, 39]. Furthermore, Pescosolido et al. [15] found that larger social and kin networks were associated with greater coercion from family and friends to seek mental health care. The present study did not find that social supports influenced length of time to receiving mental health treatment. Social support increased the likelihood of more allied health consultations, suggesting that having confidantes encourages sufferers to seek professional psychological support. The absence of such support was associated with an increased reliance on hospital emergency services.
Ethnicity, English language proficiency and acculturation were not associated with longer delays in reaching care or in the number of professionals consulted. These findings are at variance with previous research that tended to show that ethnicity influenced the duration of help-seeking and the pathways taken to reach care. Early research by Lin et al. [11, 40, 41] reported that Chinese immigrants were more likely to be supported by families who are reluctant to seek psychiatric referral. However, a number of recent studies have questioned such conclusions. For example, Okazaki [42] reported a substantially shorter treatment delay than Lin et al. [11] in a sample of 62 Asian-Americans presenting for mental health care. Moodley and Perkins [27] did not find any difference in the routes to psychiatric admission in a consecutive series of Afro-Caribbean and White patients in an Inner London Borough. Cole et al. [30] found that social support variables were more important than ethnicity in determining pathways to care among patients presenting with first onset psychosis to a service in the UK. One possible explanation for this apparent variation in findings may relate to improvements in service delivery to minority populations in Australia, with significant resources in recent times allocated to improving the cultural sensitivity and accessibility of mental health services.
In the present study, ethnicity was related to the range of professionals consulted. Arabic-speaking patients were more likely to consult with GPs and Asian-born patients were less likely to have contact with allied health professionals than the Australian-born. These findings suggest a more restricted range of professionals being consulted by immigrant patients.
Explanatory models adopted by patients appeared to influence help-seeking pathways, in that those endorsing supernatural explanations had higher rates of psychotic illness and hence reach public health services. Interestingly, this phenomenon was not related to ethnicity.
In drawing inferences from the present data, the limitations of the study need to be acknowledged. The data were collected retrospectively and relied largely on respondent recall. Where possible, this information was supplemented by data from patient files. Future research would benefit from corroborative interviews with key family members in order to validate the data collected. Another limitation of the study was the refusal and noncontact rate with only 63% of those presenting to the service in the study catchment area participating because of a particularly high non-contact rate (22%). While this may reflect the unstable nature of the population, it is possible the patients who were lost to follow-up had different pathways to care from those who were interviewed. Future study designs might obviate this problem by ensuring that research interviews occur in close proximity or as part of the first clinical assessment, although the level of disturbance of the patient may limit the capacity to achieve this in all cases. An added limitation was the modest sample size which created a limitation in statistical power [43]. Questions have been raised regarding the validity and interrater reliability of the HoNOS in some settings [44, 45], but it was noteworthy that the HoNOS total score was similar to that found among a much larger population of newly admitted patients in Australia [46]. In addition, in order to achieve consistency in ratings, project staff were provided with training in the use of the HoNOS with regular meetings to ensure consistency.
Conclusions
The main finding of the study is that GPs continue to play a central role in the pathways to mental health care. Supporting the capacity of GPs to make informed judgements about timely referral therefore would seem to be an important ongoing priority. As expected, psychotic patients tend to be referred early, they are more likely to be admitted and pathways more commonly include the police and emergency departments. Those with nonpsychotic disorders take longer to reach specialist mental health care and are most likely to be treated in the community. Their HoNOS scores suggest the possibility that those with lower levels of symptoms are treated by GPs or other allied health professionals without the need for referral. The data on ethnicity suggest that there may have been significant changes in the patterns of referral in Australia with immigrants reaching public mental health services more rapidly than suggested by earlier research [47]. Nevertheless, that conclusion can only be tentative given the absence of population-wide data on the prevalence of various categories of mental disorder according to ethnicity. The available studies suggest that there may be variation in need according to ethnic background [48, 49]. Nevertheless, the present study does indicate the need for attention to improving access to allied health personnel by increasing the numbers of same-language professionals and ensuring accessibility and affordability.
Footnotes
Acknowledgements
The study was supported by a Research and Development Grant (Commonwealth Department of Health and Human Services) and a Health Research Foundation Sydney South West and Ingham Institute Grant. Thanks to Sung Dang, Nancy Ibrahim, Beste Jamali, Peggy Lee, Peter Quoc-Vinh Lee, Ka Sim Leung, Kim Low, Lauren Munroe, Jacqui Taylor, Deepali Trackroo, Ranya Yacou Erdal Vurel and Maureen Fitzgerald for their assistance in completion of this research project.