
Abstract
Asylum seekers arriving in an unauthorized manner to industrialized countries are increasingly being subject to detention because of the recent tightening of the refugee policies in these countries [1, 2]. In Japan, detention may occur at the time of applying for refugee status or in the refugee determination process, that is, during the interview or domiciliary visit by the immigration authority to investigate the reason for their undocumented status. However, in practice, not all asylum seekers are detained. The criteria for detention are unclear and whether or not an asylum seeker is detained is unpredictable. Following the terrorist attacks in New York in September 2001, Afghan asylum seekers in Japan were increasingly detained (Lawyers League for Afghanistan Refugees, unpublished data, April 2002). Several industrialized countries also started to announce further restrictive immigration policies [3]. This insecure situation caused an unnecessary fear among these asylum seekers in Japan [4].
The detention of asylum seekers would most likely interrupt their recovery from psychological distress [5], while the recovery process may be speedier if the postmigration environment is safe, supportive and predictable [6]. Reports from Japan, Australia, the USA and some countries in the European Union [1, 2, 5,7–12] suggest that suicidal thoughts, and attempts and serious selfharm are recurrent among detained asylum seekers, yet adequate medical services are not always available to them. Limited access to educational or recreational opportunities has been reported in multiple settings and allegations of inhumane treatment at the hands of detention officers or inmates are commonplace.
The potentially traumatic circumstances surrounding detention might trigger psychological distress among detained asylum seekers [5,10–12]. Some of the detained Afghan asylum seekers in Japan repeatedly attempted suicide during detention [8]. However, the effects of detention on the mental health of asylum seekers has not been thoroughly investigated, primarily because of the difficulties in gaining access to asylum seekers, especially those detained. It is only recently that a longitudinal study among detained asylum seekers indicated that their psychological distress worsened with time in detention while it showed an improvement after release [13]. As this study did not include a comparison group of nondetained asylum seekers, it did not reveal the net impact of post-migration detention on mental health.
In the present study, we examined the adverse effects of post-migration detention on mental health by comparing asylum seekers who had once been detained (though released from detention at the time of this study) and those who have never been detained, focusing on Afghan asylum seekers in Japan.
Method
Participants and their security issues
Participants of this study were asylum seekers from Afghanistan who were in the process of applying for refugee protection in Japan. As of 2001, the official number of Afghan asylum seekers in Japan was 138 including 78 who newly applied for refugee status in that year, of whom three were recognized as refugees. Another 39 had their application for refugee status rejected [14]. A large majority of the Afghan asylum seekers were male.
These Afghan asylum seekers fled their country mainly for political persecution where Hazara and Tajik ethnicities were more suppressed under the Taliban regime. They mostly passed through Pakistan or Iran and arrived in Japan by air. They were accessible through a group of lawyers representing them in Tokyo and two non-governmental organizations (NGOs) in Tokyo and Osaka. These lawyers were independent of the government and voluntarily helping them.
We invited those who were aged at least 18 years old. Between November 2002 and March 2003, we contacted all 73 Afghan asylum seekers (71 men, 2 women) who were accessible through these groups; those who lived far from the aforementioned two cities, if any, were not included in this study. Of those contacted, 55 (53 men, 2 women) agreed to answer the questionnaire (response rate 75.3%), with 17 reporting their detention in Japan. When we contacted them, an average of 16 months had passed since the terrorist attack in New York, and for those who had been detained in Japan, about 10 months had passed since their release from detention.
We explained to them about the aim of our study and asked for their voluntary participation. We informed them orally in Japanese or English and also in writing (in Dari, their common language) whether or not the participants were literate that the authorities had nothing to do with this study, refusal to participate would not affect their refugee application, the questionnaire would be kept entirely anonymous and confidential, and they could skip any question of the questionnaire if they felt uncomfortable to respond. Of the 55 participants, 33 gave their written informed consent, while others gave only oral consent because they said that signing would remind them of the immigration authorities, or because they simply did not want to sign. We therefore did not seek for other forms of consent such as obtaining fingerprints and taping their oral consent. All the procedures of this study were approved by the Institutional Review Board of the University of Tokyo, Faculty of Medicine.
Measures and data collection
We measured the anxiety and depression levels using the Hopkins Symptoms Checklist-25 (HSCL-25) and studied posttraumatic stress disorder (PTSD) using the Harvard Trauma Questionnaire (HTQ). The HSCL-25 is a widely used screening instrument to measure anxiety and depression among refugee populations on account of its simplicity and non-provocative nature [15]. The HSCL-25 includes 10 symptoms of anxiety and 15 symptoms of depression. The HTQ was developed to assess PTSD in refugee populations and includes 16 symptoms as defined in the
Two Afghans independently translated the questionnaire from English to Dari, a common language among the participants. A third Afghan then compared these two sets of questionnaire in terms of readability of the Dari version and then back-translated them (from Dari to English). We checked the comparability of the original and the back-translated questionnaires. Internal consistency reliability (Cron-bach's alpha) of anxiety, depression and PTSD symptoms in the Dari version was 0.91, 0.87 and 0.91 respectively.
As the majority of the participants were illiterate in their own language as well as Japanese and English, the self-administered questionnaire was read out to the participants using an audiotape player. The participants could themselves tick the option of their choice to answer the questions. Data collection was conducted at the places of participants' convenience and preference, like the NGO's office or coffee shops. Three NGO caseworkers working for asylum seekers independently conducted the data collection from the participants. We employed them because they were considered more trusted by asylum seekers.
Analysis
Symptom scores of anxiety, depression and PTSD were obtained in terms of the sum of responses divided by the number of the items answered; therefore, the scores ranged from 1 to 4. As some participants skipped some of the symptoms in scoring, we analysed the data when they were both included and excluded, and compared the results. As the results did not largely differ, we have presented the results of the analyses that included all the participants. However, one participant did not answer any of the questions on PTSD. He was excluded from the analyses for PTSD. For two participants who did not report their date of their entry into Japan, the date of their refugee application was used to estimate the time they had spent in Japan. One participant for whom neither of these two dates was available was excluded from the analyses that took into consideration the time spent in Japan.
We did not use scale-cutoff points for the caseness of the mental disorders that have been determined in Indo-Chinese refugees [15, 16]. An algorithm method based on the DSM-IV criteria that was used in the case of Bosnian refugees [17, 18] was also not used. As these criteria for the caseness have not been established for Afghan refugees, we considered that using the raw score would be more appropriate.
Those who had once been detained in Japan and those who have never been detained (hereafter, detained and non-detained asylum seekers) were compared on their symptom scores, the number of trauma events experienced or witnessed, and demographic characteristics. This comparison was performed using a Student's
Results
Participants
The average age of the participants was 30.2 years (SD = 6.9) ranging from 19 to 50. Of the 55 participants (53 men, 2 women), 54 (98.2%) had Islamic background, and 43 (78.2%) belonged to the Hazara ethnicity. One participant had received no formal education and 17 (30.9%) had attended only primary school. Thirty-five (63.6%) participants were unmarried, 19 (34.5%) were living alone in Japan, and 17 (30.9%) had no confidant. Of 20 participants who were married, five were living with their spouse or other family members in Japan and the rest were separated. The participants spent a mean of 24.4 months (SD = 15.6) in Japan, and 18 (32.7%) participants had once been detained in Japan. For 17 of these participants the detention period had ranged from 4 months to 10 months (median 7 months). This information was missing for one participant. There were no statistically significant differences in these characteristics between detained and non-detained asylum seekers (Table 1).
Characteristics of 55 Afghan asylum seekers: 18 who had been detained in Japan and 37 non-detained
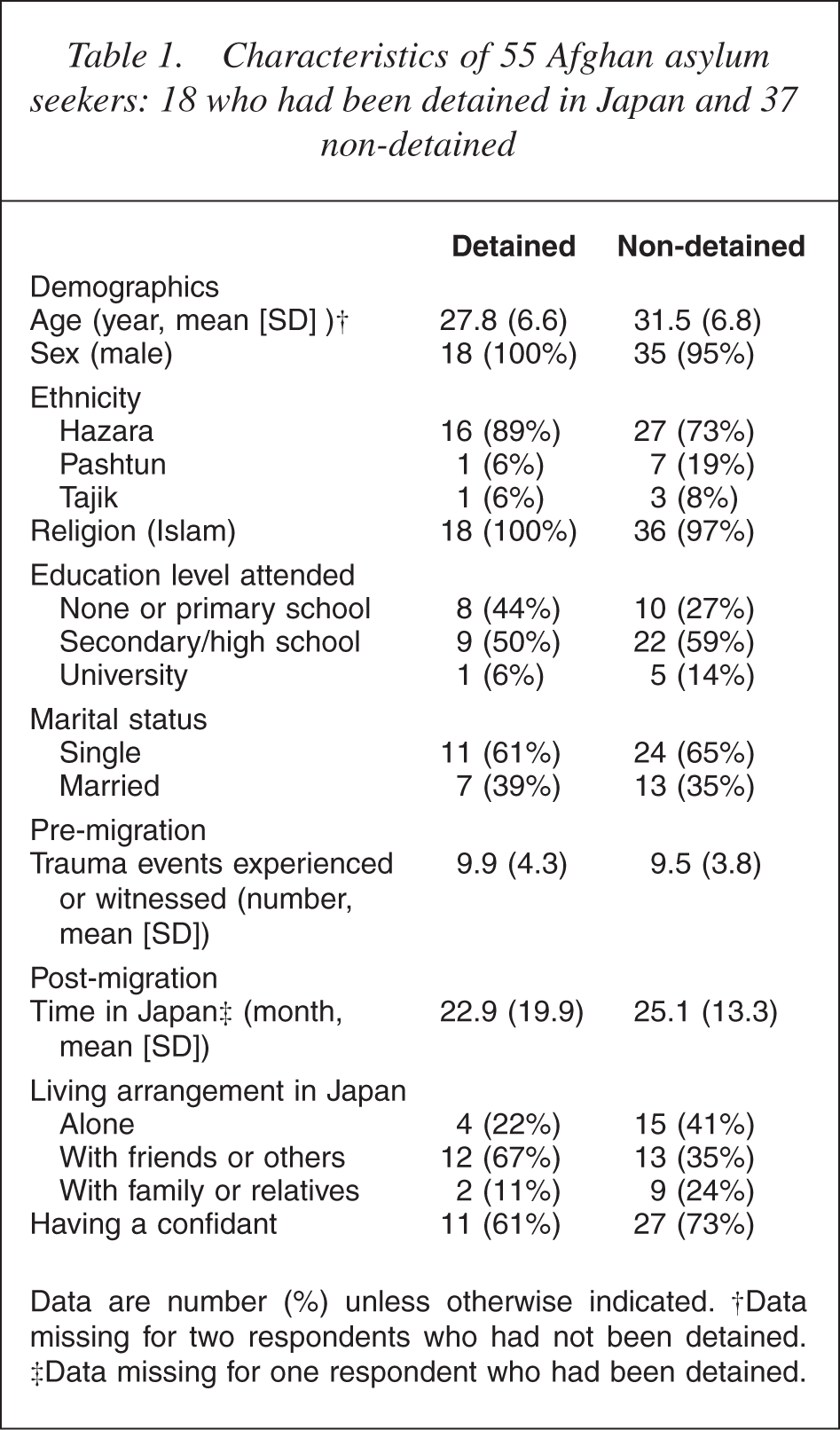
Data are number (%) unless otherwise indicated. †Data missing for two respondents who had not been detained. ‡Data missing for one respondent who had been detained.
Trauma exposure
The mean number of trauma events experienced or witnessed was 10 (SD 4.0). The most commonly experienced or witnessed trauma events were being close to death (81.8%), combat situation, forced separation from family members (80.0% each), forced isolation from others, murder of family or friends and torture (67.3% each). The number of trauma events experienced or witnessed was not significantly different between the detained and the non-detained asylum seekers (Table 1).
Post-migration detention and mental health
While there were no significant differences in terms of characteristics and trauma exposure between detained and non-detained asylum seekers, the former showed higher symptom scores (Table 2). They scored significantly higher on anxiety and PTSD with their scores being higher by 0.61 and 0.55 on a 4-point scale respectively. The difference in the mean symptom score on depression (0.34) was less than that for the scores on anxiety and PTSD.
Mean symptom score of mental disorders of detained and non-detained asylum seekers, and the mean difference (95% CI)
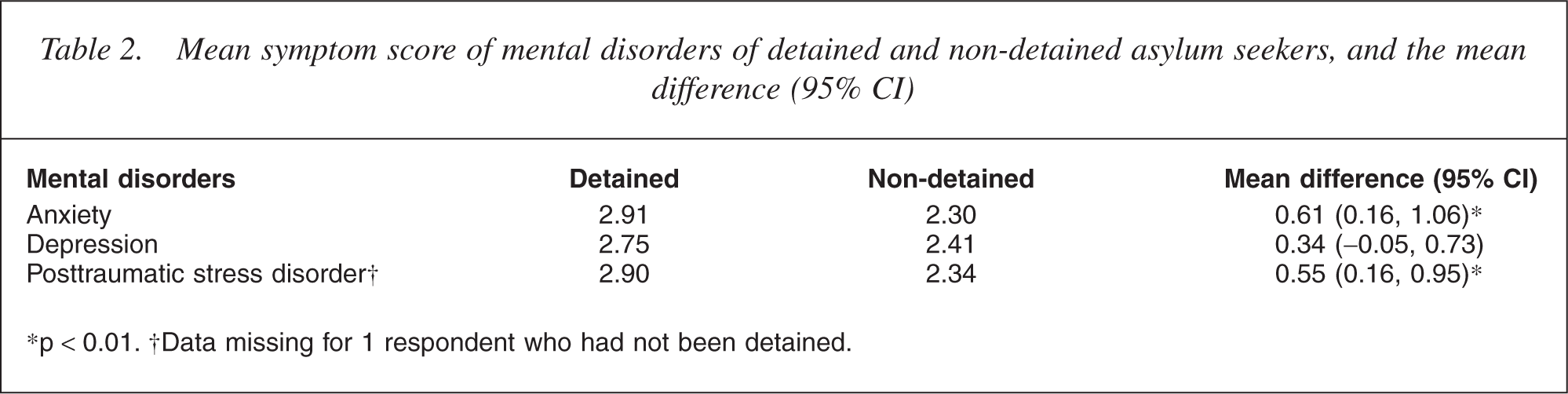
∗p <0.01. †Data missing for 1 respondent who had not been detained.
Relative effects of post-migration detention, trauma exposure and other factors on mental health
Post-migration detention was significantly related to higher symptom scores for all the mental disorders after adjusting for trauma exposure and other variables (Table 3). The estimated score increase attributable to post-migration detention was 0.68 on anxiety, 0.47 on PTSD and 0.43 on depression. Greater trauma exposure was also significantly related to higher symptom scores for all the mental disorders. Relative effects of the detention and trauma exposure were comparable. As for the relationship between mental health and demographic characteristics, only the effect of living alone remained significant and appeared almost equivalent to that of the detention and trauma exposure. The models explained nearly 30% of the variance in symptoms.
Relative effects of post-migration detention and other variables on mental disorders: standardized (Beta) and unstandardized (B) coefficients and its 95% CI from multiple linear regression models
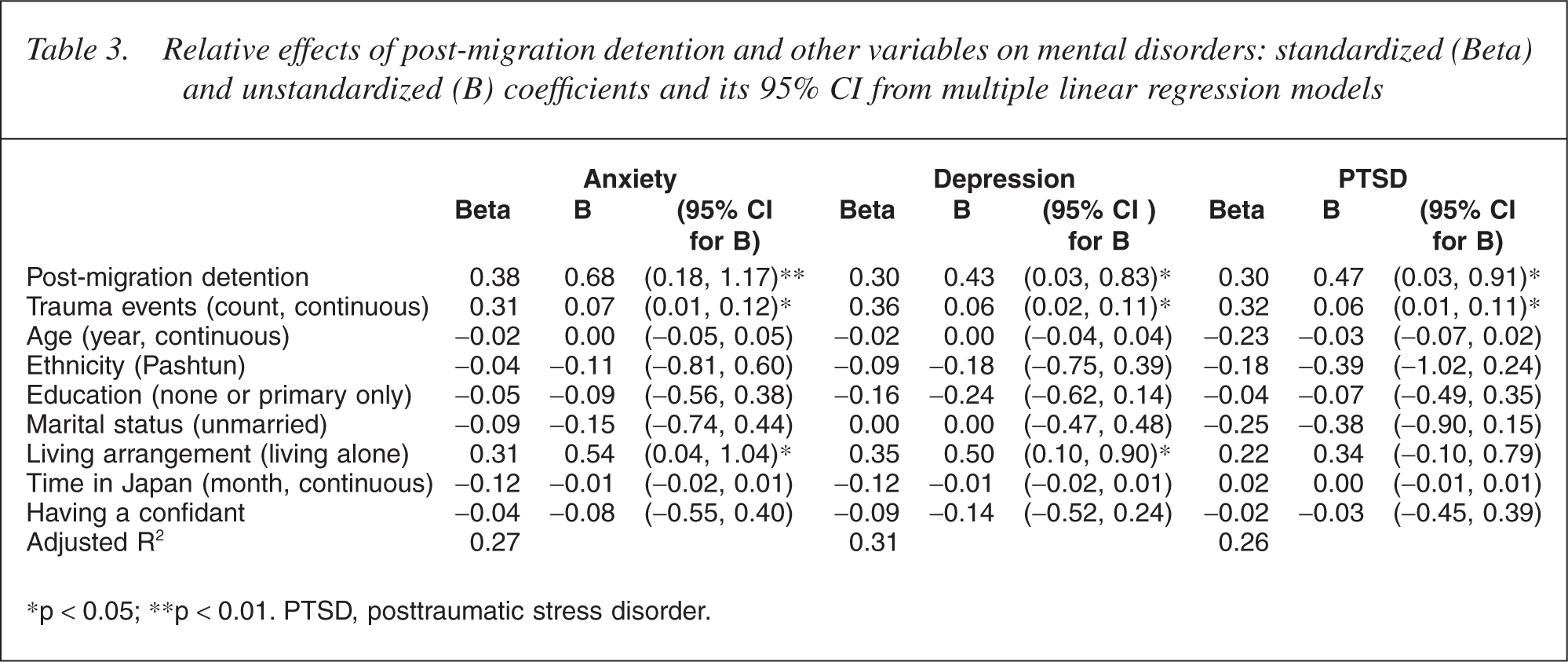
∗ p < 0.05; ∗∗p < 0.01. PTSD, posttraumatic stress disorder.
Discussion
We found that post-migration detention was associated with worsened mental health status among Afghan asylum seekers in Japan. In this study, we attributed this to post-migration detention in the following manner. First, comparing the detained and non-detained asylum seekers, we showed the net impact of the detention on their mental health. The cross-sectional nature of this study might have even underestimated the actual impact because the detained asylum seekers had already been released from detention when they were contacted, nearly 1 year after the release. Their psychological distress could have been alleviated by then [13].
Second, even in the cross-sectional study we considered it reasonable that a temporal relationship should exist between detention and mental health as there are no reasons to assume that those who were mentally ill tended to be detained. Our causal inferences are consistent with the previous longitudinal study that revealed the correlations between elevated symptoms and the length of the time spent in detention, and reduced symptoms among those who were released [13]. The relationship between the severity of psychological distress and the time spent in detention would support the temporal relationship existing between them; however, the crosssectional nature of this study did not permit us to examine this aspect.
Third, post-migration detention was found to be related to the mental health of the asylum seekers, after we controlled for the factors related to refugee mental health, particularly trauma exposure. We thus suspect that the post-migration detention of asylum seekers exacerbates their mental health.
Pre-migration trauma exposure was also related to worsened mental health. As a major determinant for refugee mental health, the trauma is primarily taken into account in refugee health care and research. Nonetheless, we found that the effects of the trauma and the detention on mental health were comparable in terms of the symptom scores. This finding has important clinical and policy implications in our efforts of protecting asylum seekers in post-migration.
We acknowledge the limitations of this study. First, we used the psychiatric scales that have not been clinically validated for the Afghan population. Cross-cultural differences could have created a systematic bias and the use of self-report measures could have inflated our estimates [20]. To avoid misclassifications, we did not define cases of mental disorders, using predetermined scale cut-off points of the symptom scores or an algorithm. Instead, we used the symptom score to investigate the effect of the detention. In this approach, the potential measurement errors mentioned above are less likely to distort our results. Moreover, it is noted that the scales had high levels of internal consistency in the Dari version and were used within a culturally homogeneous population.
We may have overestimated the effects of detention on mental health in case the detained asylum seekers exaggerated the state of their mental health. However, its extent is uncertain because such over-reporting could have occurred among any respondents who expected some gain by exaggerating their life experiences, regardless of their exposure to post-migration detention. We therefore assumed that the over-reporting did not necessarily occur in a systematic manner, while the scores could have been elevated owing to possible overreporting. To lessen this problem, we used the symptom scores in estimating the effect of the detention, as mentioned earlier.
The possibility of a recall bias exists; however, it is unlikely to have altered the results. Recall of core life experiences among the traumatized population is generally reliable [21], and their recall bias is attributable to both over- and under-reporting [22]. Finally, as only those respondents who were accessible were questioned, and one in four refused to participate, the generalizability of our findings to the entire population is limited. Asylum seekers who had no contacts with lawyers or any other supporters might have experienced more anguish postmigration. Besides, it is also noted that men were dominant in the study participants, further limiting the generalizability.
In conclusion, we found that the post-migration detention of Afghan asylum seekers in Japan was independently related to their worsened mental health. We suggest that the recent tightening of the immigration policies towards asylum seekers be reconsidered for the purpose of both health and human rights.
Footnotes
Acknowledgements
We thank all the participants of the study and acknowledge the generous cooperation of the Lawyers League for Afghanistan Refugees, the Japan Association for Refugees, the Catholic Osaka Archdiocese Social Action Centre, all of whom made the data collection possible. We also acknowledge the substantial contribution of the three anonymous Afghans who helped us develop the Dari version of the questionnaires.