
Abstract
Keywords
Electroconvulsive therapy (ECT) is an effective treatment of depression and especially effective for severe depression, with success rates of 80% or more [1, 2]. Many patients who have not responded to antidepressants improve with ECT. Because of adverse publicity, much of which is ill-informed and unjustified, there has been resistance to the use of ECT. This may delay or deny some patients getting effective treatment, prolong theirmorbidity and increase the risk of death from untreated illness.
A common patient concern is of memory loss. Electroconvulsive therapy can cause memory impairment (especially in the short term), post-ECT confusion, disorientation and rarely delirium. These cognitive adverse effects may be minimized by high-dose right unilateral ECT, with a brief-pulse electrical stimulus which causes less memory impairment than bilateral ECT [3, 4].
Although there are data suggesting that unilateral and bilateral ECT have similar effectiveness, some researchers, for example, Lambourn and Gill [5] found that treatment with unilateral ECT not much different from simulated ECT, when using low-dose stimuli, not much above seizure threshold (minimum stimulus dose at which a bilateral grand mal seizure is elicited). Lowdose unilateral ECT was also found to be ineffective in a study by Sackeim et al. [6]. Inadequate dosing is associated with increased cognitive adverse events, especially if there is prolonged ictal activity (such as<120 s), which is usually lowvoltage and without motormovements. Highdose unilateral ECT was nearly as effective as bilateral ECT and significantly more effective than low-dose unilateral ECT [4].
No correlation has been found between seizure threshold and effective treatment [7]. It is the degree to which the stimulus dose exceeds seizure threshold for that patient at that time rather than the energy of the stimulus that matters [8].
Sackeim et al.'s [4] findings have led some psychiatrists to believe that high-dose right unilateral ECT is the best treatment for severe depression using suprathreshold stimulus doses, but not so high as to increase cognitive adverse effects to the degree seen with bilateral ECT. Cognitive effects are greater at higher unilateral doses than at lower unilateral doses [4]. Weiner suggested that an ideal treatment stimulus dose range would be between 2.25 and 4.5 times seizure threshold [9]. An Australian expert group recommended initial treatment at 3 times seizure threshold [10].
Because seizure threshold typically doubles over a course of treatment, so that stimuli remain well above seizure threshold the stimulus dosemust be increased during the course. It is not generally practical to dose titrate before every treatment. Increase the dose over treatment in response to changes in electroencephalogram (EEG) monitored outcomes and clinical response [10].
Treating staff should have the training and expertise to interpret EEG results with ECT and be able to adjust the dose appropriately. A fixed dose strategy may be preferable to the risk of ineffective doses with no benefit and increased cognitive impairment, if staff are untrained and without this expertise.
Unilateral ECT administered at stimulus doses of up to 6 times seizure threshold and retained or slightly increased over the course of treatment may match the efficacy of bilateral ECT [11]. The dose of 6 or more times threshold early in treatment can increase cognitive adverse effects, though by the end of the course this dose will be only approximately 3 times final threshold.
Titration remains controversial. Abrams [7] suggested that best results are consistently obtained with age-based or fixed high-dose methods. Unfortunately, the data are not definitive on this matter. According to Sackeim et al. [11], adequate treatment stimuli to give effective unilateral ECT causes less retrograde amnesia than bilateral treatment.
It is still disputed whether excessive suprathreshold treatment results in more cognitive adverse effects than such adequate treatment. Sackeim et al.'s study suggested that higher doses were associated with more cognitive effects [4]. In contrast, Pettinati et al.'s report [12] suggested no dose effect. However, they only described anterograde non-verbal memory, and neither the common patient concern of retrograde memory nor autobiographical memory which is particularly affected by ECT [13, 14]. Another study comparing patient reports of titration-based and non-titration-based treatment resulted in a higher ‘cognitive deficit index’ in the non-titrated group [15].
Responses to a paper [7] suggesting titration unnecessary were varied, with one author [16] suggesting bilateral treatment has superior efficacy and unilateral treatment has failed. Two other responses [17, 18] advocated titration, consistent with American Psychiatric Association recommendations on ECT [19].
If one accepts that right unilateral ECT should be administered at adequate but not excessive suprathreshold stimulus doses, it is important to accurately determine the seizure threshold. The treatment dose should be effective while minimizing cognitive adverse effects. There is great interindividual variability in seizure threshold [20] and variability with stimulus characteristics, so it is important to adopt a strategy to accurately determine the initial treatment stimulus dose.
An age-based estimation is recommended by the manufacturer of the Thymatron [21], while the manufacturer of the MECTA machine recommend stimulus dose titration, although they also refer to an older sex–age–electrode placement algorithm and age-based estimation of seizure threshold [22].
Age estimations assume there is a clinically useful correlation between seizure threshold and age [23, 24]. Estimates of stimulus dose use the patient's age in years expressed as a percentage of 504 millicoulombs (mC).
With stimulus dose titration, the threshold dose is based on actual seizure threshold determination which may be the best method. Multiples of this threshold stimulus are then used as the initial treatment stimulus [25].
The aim of this study was to compare initial seizure threshold determined by stimulus dose titration in patients with major depressive disorder who were to be treated with high-dose right unilateral ECT with an empirical estimations based on the patient's age and half age. This study also aimed to assess the relationship between seizure threshold and age.
Method
A consecutive group of psychiatric patients treated for major depressive disorder at two of the largest private psychiatric hospitals in Melbourne were assessed. These hospitals together treat over 300 patients per year with ECT. Patients were referred to the relevant ECT service by their treating psychiatrists, who remained in charge of their overall treatment. The treating psychiatrists were requested by the ECT service to reduce or stop concomitant psychotropic drug(s), with specific advice to cease any drug(s) that could adversely affect ECT, such as benzodiazepines and anticonvulsants. Other drugs were generally unchanged during the course of treatment. Although most of the treating psychiatrists ceased drug(s) with anticonvulsant properties, some only reduced the dose. Thus, some of the patients were on drugs that may have affected their seizure threshold. This was not seen as a major drawback, as the patients were representative of those having ECT in the general community.
All patients had their seizure threshold determined using the stimulus dose titration technique described by Sackeim et al. [4]. Patients were fasted for at least 6 hours before ECT and pre-oxygenated with oxygen 100%. Patients were given anaesthetic (either methohexitone or thiopentone on the attending anaesthetist's judgement) and muscle relaxant (suxamethonium), with the ipsilateral calf isolated with a blood pressure cuff inflated above systolic blood pressure before administration of the muscle relaxant. None of the patients were administered anticholinergic agents, for example, atropine or glycopyrollate, before or during ECT.
The psychiatrists who participated in this study had all completed a training course and administered ECT on a regular basis. They all used the same stimulus dose titration technique, similar dose adjustments in the course of treatment and the Thymatron DGx ECT machine.
Electroconvulsive therapy was administered using a first-titration stimulus dose of 25mC for females and 50mC for males. If no seizure occurred, the stimulus dose was then increased by 25 mC. Seizure threshold was the stimulus dose at which there was definite evidence on the EEG of generalized bilateral seizure activity, with associated motor activity in the isolated ipsilateral limb. None of the patients were administered more than three stimulus doses to determine seizure threshold.
Results
Two hundred and three consecutive psychiatric patients referred for high-dose right unilateral ECT were assessed. There were 149 females who had their seizure threshold determined, with an average age of 52.3 years, standard deviation (SD) 18.2 years and an average seizure threshold of 50mC (SD=20.2). There were 54 males with an average age of 49.8 years (SD=18.2 years) and an average seizure threshold of 60.7mC (SD=19.9mC). There were no significant complications.
Males had a significantly greater average seizure threshold than females (t-test: p<0.000).
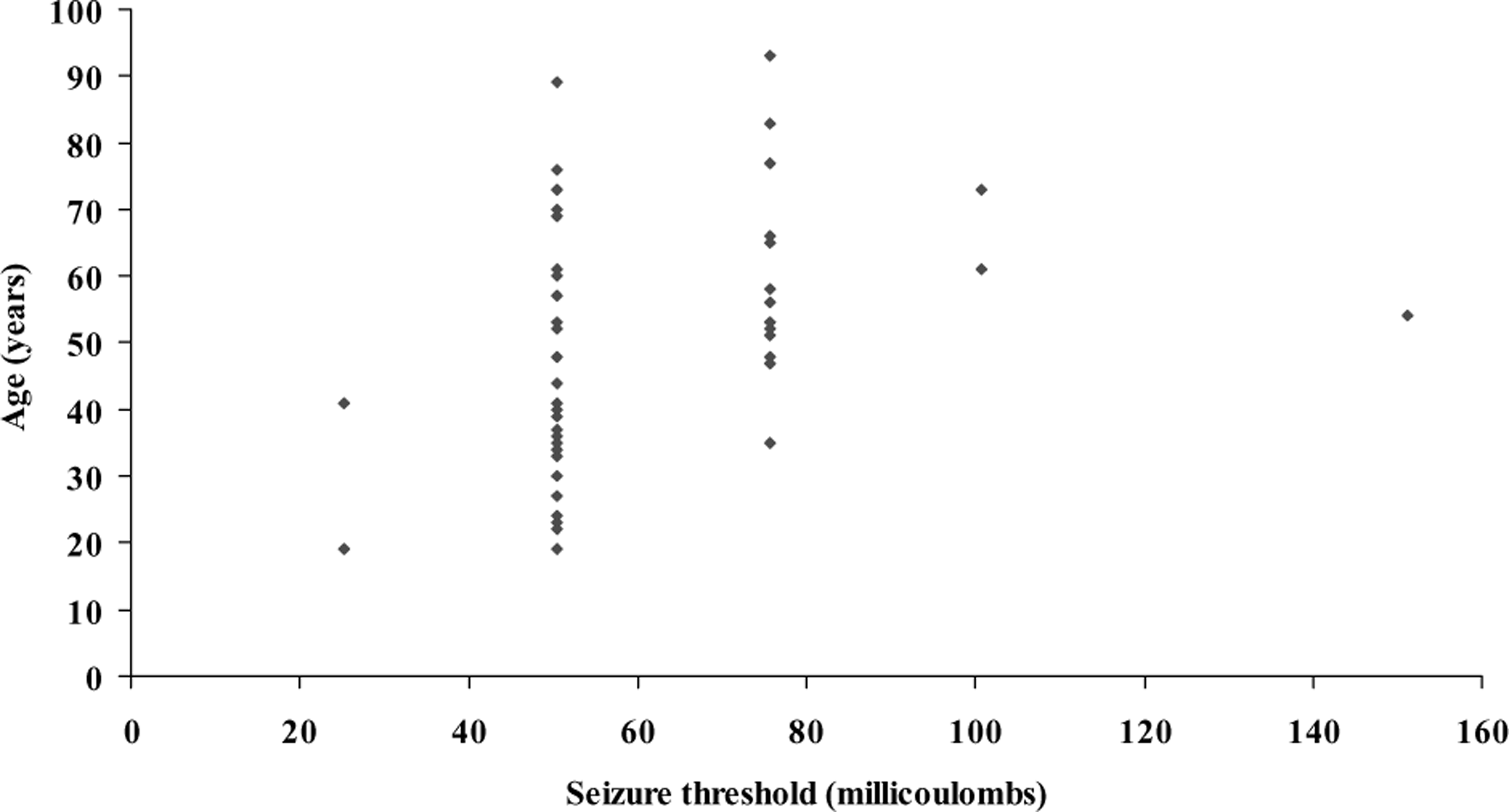
Using the Pearson two-tailed test of correlation, there was a highly significant correlation between seizure threshold and age: r=0.386 (p<0.004) for males and r=0.299 (p<0.000) for females. Correlations between age and threshold dose for men under 60 years were r=0.482 (p=0.002) and 60 years of age or over were r=0.003 (p=0.99). For women under 60 years, r=0.297 (p=0.003) and 60 years and over, r=0.288 (p=0.039). However, as Figs 1 and 2 show there was a wide dispersion of seizure threshold at each age and the wide dispersion was as apparent at older ages as at younger ages.
Seizure threshold versus age in females (n=149): r=0.299 (p<0.000). Seizure threshold versus age in males (n=54): r=0.386 (p<0.004).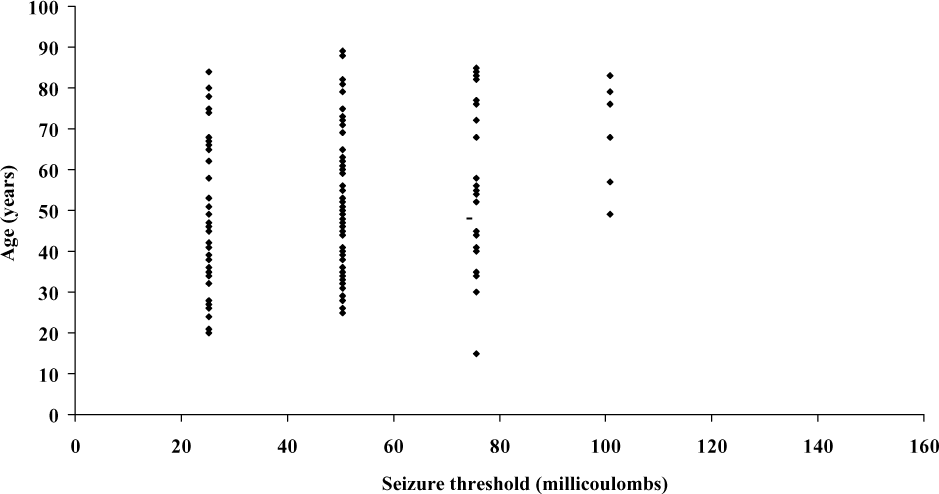
If age had been used to estimate the seizure threshold, the subsequent treatment stimulus dose for 54% of females and 31% of males would have been 5 ormore times seizure threshold and 30% of females and 8% of males would have been 7 or more times the seizure threshold. Two per cent of females and 7% of males would have been undertreated or untreated as they would have received treatment stimulus doses below 2.25 times seizure threshold – too low a dose to be effective.
If a half age strategy was adopted, then 87% of men and 55% of women would have been underdosed. Considering those over 60 years of age, 60% of men would have been underdosed, though half-aged dosing for older women would have probably been effective as it was approximately 3–4 times threshold.
Discussion
In Australia, present recommendations are for highdose right unilateral ECT, with the initial treatment stimulus dose being typically 3 times the seizure threshold [26], with progressive increases over the course of treatment [11]. This approach is believed to be effective while minimizing cognitive adverse effects. The trend is to not use very high-dose or fixed high-dose unilateral ECT (say at 6 times seizure threshold) as the advantages, if any, in efficacy are potentially offset by increased cognitive adverse effects. There is contention about the best way of determining seizure threshold [9, 27]. Fink's opinion [27] is that age-based estimations are appropriate, with treatment stimulus dose based on the patient's age in years as a percentage of 504 mC, while Weiner [9] has advocated individual stimulus dose titration.
The most accurate way of determining seizure threshold is with stimulus dose titration. This involves administering several subthreshold stimuli at the same session to determine and then give the dose for the first treatment. This means the anaesthetic and muscle relaxant doses need to be increased, the patient is unconscious for longer than without titration and there is potentially an increased risk of complications.
There may also be a risk of bradycardia and arrhythmias with subthreshold stimulus doses during stimulus dose titration [28]. Despite these potential disadvantages, the authors did not find any significant complications in the patients studied. Muscle aches and headaches were reportedmore frequently with stimulus dose titration than with subsequent treatments. This may be because of the higher dose of muscle relaxant used during stimulus dose titration, but these symptoms were mild, transient and responded to simple analgesics.
The age-based estimation suggested by Fink [27] avoids stimulus dose titration. His opinion is that this approach is reasonably reliable for most patients, though he noted that for the elderly, higher stimulus doses were required and for the young, age-based estimation may deliver an unnecessarily high stimulus dose.
If the patient's age had been used to decide the treatment stimulus dose, many patients would have fallen outside the 2.25–4.5 times the seizure threshold [9] range, that is, their initial treatment stimulus dose would have been either too low or too high.
Our findings show that an age-based estimation of seizure threshold is likely to provide suboptimal results for more than half the adult patients. Despite the previous suggestions that stimulus dose titration is impractical under routine clinical conditions [29], we found it to be practical and avoids guessing, given the wide interindividual variation in seizure threshold.
In this study there were a few patients in all age groups of men and women who were on low doses of psychotropic medications which had anticonvulsant effects. There was no obvious excess use in any one group. If this use had any effect, it would have been to slightly increase treatment threshold. This would not have materially altered the substantial number of patients whose dose would be suboptimal using age-based estimates. This use of psychotropics had the benefit that it did represent the common clinical context for ECT. Nevertheless, that use is a potential limitation with this study.
Age-based estimations would have resulted in excessive doses for 24% of patients and suboptimal initial treatment doses for 7% using full age and 64% using half age strategies. As a result we recommend dose titration at the start of a course of ECT. During treatment, because of limitations with other EEG-based surrogate markers for clinical effectiveness, we suggest re-titration if dose adjustments result in doses that seem too high or the clinical outcome is poor. Re-titration usually confirms the treatment dose, but if adjustments are needed, it is more common that the titrated threshold is lower than anticipated.
These data reinforce that statistical significance with these correlations does not necessarily mean clinical relevance. Interindividual differences warrant individual stimulus dose assessment to optimize treatment.
Conclusions
These data suggest that fixed high-dose treatment is likely to lead to excessive initial treatment stimulus doses that defeat the cognitive sparing purpose of using unilateral ECT. An empirical age-based estimation of seizure threshold will result in suboptimal initial treatment for more than 50% of patients. These data suggest that it is important to determine seizure threshold with stimulus dose titration, so that the optimal initial treatment stimulus dose can be administered for each patient.
Footnotes
Acknowledgements
The authors acknowledge the assistance of D. Thompson for data collection, T. Layton for data analysis and B. Khariwala for editorial assistance.