
Abstract
Problem of biopsychosocial case complexity in general health care
Psychiatric and psychosocial comorbidities are increasingly prevalent in general health care because of increase in number of the elderly and number of patients with chronic diseases [1]. Psychosocial comorbidities influence the outcome of various somatic diseases [2] and are related to excess health-care utilization [3], poor quality of life [4], non-survival [5] and suboptimal compliance with medical treatment, which represents a major obstacle to effective medical care [6]. However, the biopsychosocial model of disease [7], in which an assessment of biopsychosocial care needs is made, has not been implemented in standard general health care, resulting in undertreatment of psychiatric and psychosocial comorbidities [8],[9].
The problem seems to lie in the lack of operationalization of biopsychosocial case complexity. Although several attempts have been made to operationalize the biopsychosocial model and to develop instruments to assess case complexity, no methods applicable to patients in general health care have been widely accepted and implemented [10],[11]. The issue of how to approach biopsychosocial complexity thus remains an important challenge. In this paper, we will describe the INTERMED, an instrument to assess biopsychosocial case complexity in general health care [12] and provide an overview of its psychometric evaluation.
Operationalization of biopsychosocial case complexity
In order to develop both a scientifically sound and clinically meaningful tool for the assessment of biopsychosocial case complexity, data need to be collected and evaluated in a reproducible and valid way. Therefore, a psychometric approach was chosen in the operationalization of case complexity: an initial face-valid item pool was reduced, and validated by means of correlations with existing instruments [13],[14]. Instruments developed from psychometric theory tend to be reliable and valid, but are often long, complicated and sometimes even redundant. This approach was thought therefore to be insufficient for general health care and was complemented by the clinimetric method [15]. This approach favours simple and readily interpretable scoring, heterogeneity of variables, easy use of the instrument, face-validity and absence of subjectively judged items. Although the clinimetric approach tends to produce relevant and concise methods, thesemay sometimes be too simple and lack precision. As both approaches have their advantages and limitations, a combination of psychometrics and clinimetrics was used to develop the INTERMED, which had to have facevalidity, and be brief and easy to use, generic and flexible, reliable and valid. Additional features required that were intermediate between the psychometric and clinimetric approaches were those of the uni-dimensionality of the method and the inclusion of subjective data. The method needed to lead to a total score (rather than an interpretation of individual items), since biopsychosocial complexity is considered to be an underlying construct influencing all variables. However, the level of uni-dimensionality was not considered as crucial as in the psychometric approach. Total exclusion of subjective (patient) data – as suggested in the clinimetric approach – was not considered adequate, since complaints perceived by the patient are relevant for the assessment of case complexity.
INTERMED: a method to assess biopsychosocial case complexity
Based on earlier attempts to operationalize the biopsychosocial model of disease [10], we developed a grid, describing the biological, psychological, social and health care-related characteristics of the patient's history, and their current state and prognoses. This resulted in 12 cells in which information is organized (Table 1). For each cell of the ‘history’ and ‘current state’, two pertinent variables were selected, known from clinical expertise and/or scientific evidence to be important in directing patient care, and one pertinent variable for each cell of the ‘prognoses’. The selection of the 20 variables was discussed and ascertained by a panel of researchers and clinicians from various disciplines, that is, consultation–liaison psychiatry, internal medicine, rheumatology, psychology and geriatrics, in order to obtain sufficient face-validity.
Variables of the INTERMED scoring grid
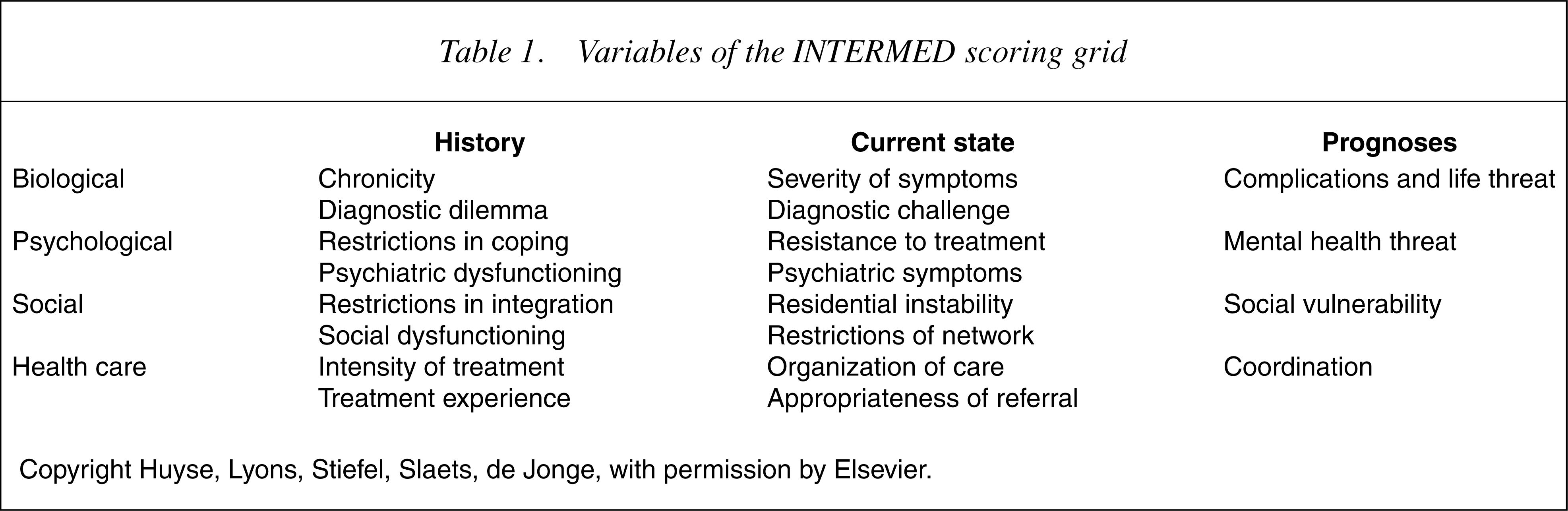
Copyright Huyse, Lyons, Stiefel, Slaets, de Jonge, with permission by Elsevier.
Psychometric evaluation of the INTERMED
The psychometric evaluation of the INTERMED was focused on its reliability and its capacity to detect patients in need of multidisciplinary treatment.
Reliability of the INTERMED
Classical test theory identifies three basic types of reliability: internal consistency, inter-rater and test–retest reliability [14]. Following the first inter-rater reliability study with the INTERMED [12], a final versionwas developed, which was then tested in a sample of patients with varying somatic illnesses. Patients were double scored by two raters, a psychologist and a psychiatric nurse [16], based on a review of the medical chart and a patient interview conducted by one in the presence of the other. The two raters showed high agreement, as indicated by a kappa of 0.85 indicative of very good agreement [17]. Temporal stability of the INTERMED was assessed in ambulatory patients with multiple sclerosis, with 1 year between the two assessments [18]. The correlation between the two assessments was moderate to good, indicated by a kappa of 0.60. Data from several of the INTERMED studies in different somatic patient populations were pooled to evaluate internal consistency [19]. In the total sample (n = 1104), Cronbach's alpha was 0.87 (95% confidence interval (CI): 0.86–0.89), while for the individual samples, alpha's ranged from 0.78 to 0.94. The findings give sufficient support for the reliability of the INTERMED and the use of the total score to describe biopsychosocial case complexity.
Validity of the INTERMED
Validity of the INTERMED could be addressed only in an indirect way, since a gold standard of case complexity is not available. It was therefore studied by selecting relevant outcome variables in several specific patient populations. In a sample of patients admitted to a general medical ward, we found that patients classified by the INTERMED as having a high degree of case complexity had a doubled length of hospital stay, and increased use of medications, nurse interventions and specialist consultations [20]. The findings were replicated later [21]; in addition, poorer quality of life at discharge was documented for the complex patients. In a sample of patients with diabetes, we found that the INTERMED score was related to HbA1c values, assessed 6 months earlier, and 3 and 9 months later [22]. In a sample of low back pain patients who participated in a 3-week functional rehabilitation program or applied for disability compensation, we found that INTERMED scores were significantly higher in those applying for disability compensation [23]. In a sample of patients under dialysis, we found that INTERMED scores were associated with low quality of life at 1-year follow-up [24], which in turn was unrelated to baseline parameters of the severity of illness. In multiple sclerosis outpatients, INTERMED scores were associated with measures of disability and with the number of disciplines proposed in the multidisciplinary treatment plan [25]. These data confirm the ability of the INTERMED to detect patients at risk and to predict clinical outcomes in several patient samples.
Re-analysis of data
In order to compare the above-mentioned studies [20], [22–25], we conducted a re-analysis of the data based on the INTERMED cut-off point of 20/21 [21], which has been developed as a criterion for the detection of complex cases. In order to enhance the comparability of the associations found across the studies (despite the difference in nature of the outcome data), for each of the samples the outcome measure was dichotomized, in a way that about 50% of patients had a poor outcome. Then, we calculated the capacity of the INTERMED to detect patients with a relatively poor outcome, in terms of sensitivity, specificity and odds ratio for a poor outcome in patients with an INTERMED score more than 20. For internal medicine and for dialysis patients, we used a 36-item short-form (SF-36) total score (respectively at discharge and at 12-month follow-up), for diabetes patients, average HbA1c during 9 months follow-up was used, for low back pain patients, their application for disability compensation was counted as a poor outcome, and for multiple sclerosis patients, poor functional status defined by an Expanded Disability Status Scale (EDSS) score >4 was used as an outcome. In Table 2 and Figure 1, it is shown that INTERMED scores above the cut-off score are associated with poor outcomes in all samples, with the exception of the diabetes sample where only a non-significant trend is observed.
ROC-curves for poor outcomes in each of the five samples.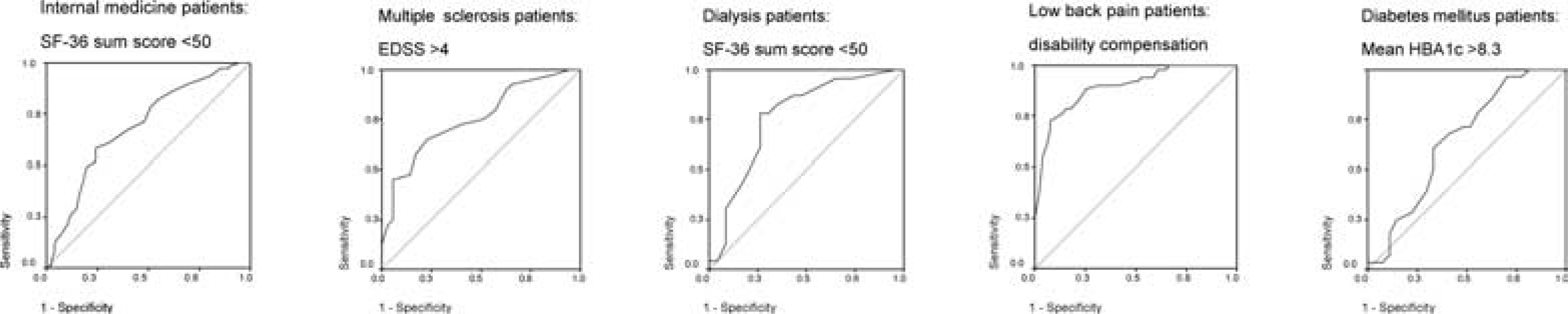
Relationship of high INTERMED scores with poor outcomes
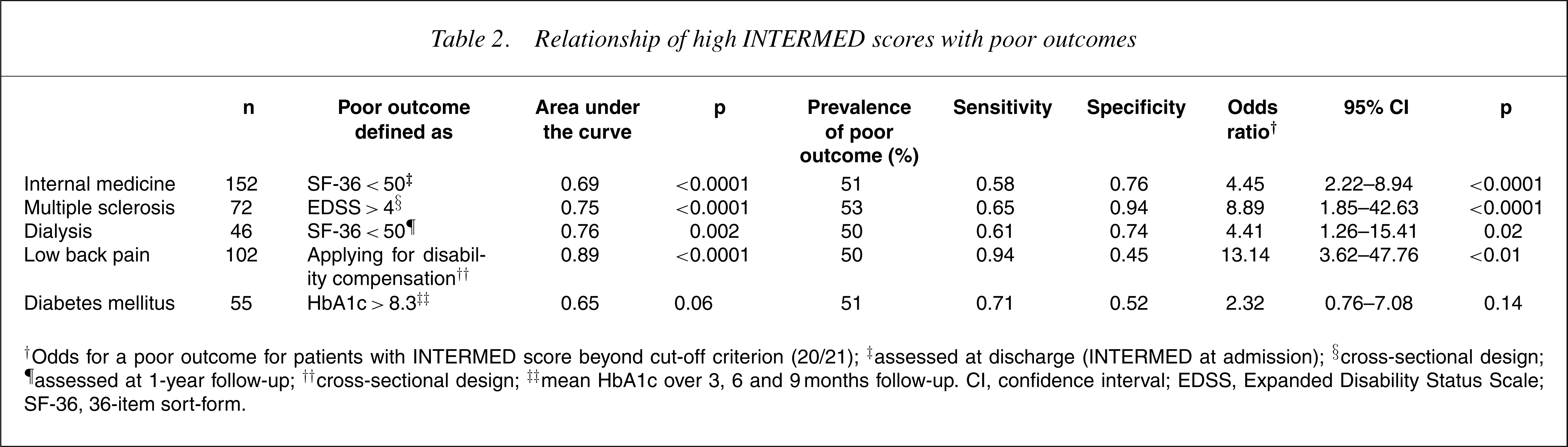
†Odds for a poor outcome for patients with INTERMED score beyond cut-off criterion (20/21); ‡assessed at discharge (INTERMED at admission); §cross-sectional design; ¶assessed at 1-year follow-up; ††cross-sectional design; ‡‡mean HbA1c over 3, 6 and 9 months follow-up. CI, confidence interval; EDSS, Expanded Disability Status Scale; SF-36, 36-item sort-form.
INTERMED: the biopsychosocial model of disease and the challenge of complexity
Studies conducted during the last 10 years showthat the INTERMED has face-validity, is brief and easy to use, and is reliable and valid. Elsewhere, it has been shown that interdisciplinary rounds could reduce length of hospital stay of general internal medicine patients [26], but application of this time-consuming type of care to all newly admitted patients does not seem feasible. Instead, we proposed to provide this kind of care to only a subset of complex patients detected by means of the INTERMED. The INTERMED has been implemented in the general Internal Medicine Department of the University Hospital Groningen, the Netherlands. All patients admitted to this ward are screened with the INTERMED and those with a score above the cut-off point are discussed in a multidisciplinary meeting. Meanwhile, in a controlled study we have shown that it is possible to improve quality of life at discharge by this way of providing care compared to care as usual [27]. Ongoing randomized controlled trials with the INTERMED in other patient samples will evaluate whether integrated biopsychosocial care for complex patients is more effective than care as usual with regard to medical outcomes, subjective benefits and health-care utilization.
Conclusion
The INTERMED project is relevant to various agents involved in the care process. It provides a basis for effective multidisciplinary treatment of patients with a high case complexity. The INTERMED project will induce a paradigm shift from a specialty-oriented to a patientcentred model of interdisciplinary care, which will foster comprehensive assessment and treatment of the complex patient.