
Abstract
In Germany, as in many countries, the integration of psychiatric services and departments into general hospitals has paved the way for psychiatry to be taken note of as a medical discipline by medical–surgical physicians and patients alike. This integration is the cornerstone of consultation–liaison (C-L) psychiatry, which specializes in physical/psychiatric comorbidity and somatization [1]. Although in all other countries there is only one medical specialty providing services in this field, in Germany since 1992 there are two; one called ‘psychiatry and psychotherapy’, the other ‘psychosomatics and psychotherapeutic medicine’. This paper tries to explain this German peculiarity (Sonderweg). It starts with a description of the reshaping of the German system of psychiatric services in the wake of the social psychiatric movement with its goal of deinstitutionalization of long-term psychiatric inpatients, the dissolution of large state psychiatric hospitals and the integration of psychiatry in general hospitals. It then elucidates the beginnings of C-L psychiatry in Germany, outlines differences and similarities of C-L psychiatry and C-L psychosomatics, and reflects on lessons to be learned from this unique set of developments.
‘Psychiatrie-enquête’ and the implementation of psychiatric departments in general hospitals in Germany
It is beyond the scope of this article to give a summary of the history of psychiatry in Germany. For the development of C-L psychiatry, it is important to note that during the second half of the nineteenth century, when the shaping of the system of psychiatric service in Germany began, the most important discussions took place between psychiatrists who worked in university hospitals, who wanted to foster psychiatric research within the scope of academic medicine, and alienists, who ran large state mental hospitals, doing the bulk of work in treating especially the poor mentally ill. Incorporation of psychiatry into non-university general hospitals hardly occurred (for further reading see [2], [3]).
Unlike in the US, where psychiatric departments in general hospitals were already common in the 1920s, in Germany the establishment of such departments in general hospitals was an iron too hot to handle until the 1960s. In 1970, there were just some 21 departments of this kind. The situation at the large state mental hospitals was unsatisfactory, but started to change when, at the initiative of the federal government, an expert commission was created to inquire into the care of psychiatric patients in the Federal Republic of Germany and make suggestions for improvement (this inquiry is one of the cornerstones of modern psychiatry in Germany and is widely known under the name of ‘psychiatrie-enquête’) [4]. It criticized the remote location of psychiatric hospitals, which interfered with the collaboration with other medical disciplines. Because approximately one-third of psychiatric inpatients suffer from additional somatic illnesses, this was tantamount to a loss of quality of care. As a solution to the problem, the expert commission recommended the urgent establishment of psychiatric departments in general hospitals [5]. In this context, the implementation of permanent C-L services was demanded explicitly for every large hospitals in which patients were treated after a suicide attempt [5]. Importantly, the provision for expansion of ‘psychiatric and psychotherapeutic primary prevention for risk groups and for psycho-social stress situations in the area of somatic medicine’ was also recommended:
Within this realm belong the care of hospitalized children and adults, accident victims as well as the incapacitated or chronically ill. Large psychological problems also occur in the context of dialysis, the treatment with cardiac pacemakers, transplantation surgery and the aseptic isolation in the care of extensive burns. The increase in technology in medicine as is practiced in intensive care units, the dependence of many patients on complicated, frequently poorly understood instruments, their forced isolation and immobility represent a significant psychic stress situation and make preventive care necessary which would be best handled by psychiatric-psychotherapeutic or psychosomatic departments at general hospitals. [5, p.392]
In a status report, 5 years after the Psychiatry-Enquête, Häfner [6] stressed that:
the psychiatric department in a general hospital is not only a prerequisite for the elimination of the separation of inpatient psychiatric care. It also provides the mentally ill with simultaneous somatic illness a collaborative treatment through other medical disciplines and the somatically ill a psychiatric therapy of high standards. (p.17)
To document the development that was initiated by the psychiatrie-enquête and in order to check on the transformation as well as to take into account newer developments, a model psychiatric program was initiated by the German government in 1979. In its final report the expert commission focused again on the care of mentally ill in the general hospitals:
Through the community-centered location and also physical integration into the general hospital, the hurdle of admission is much lower than with regard to specialized psychiatric hospitals.… This is of significant importance because many patients after suicide attempts, alcohol- and drug-dependent individuals as well as old people with psychic disorders are treated in medical-surgical departments in general hospitals. [7, pp.280–281]
In view of the high prevalence of mental disorders in medical–surgical units, the expert commission did not intend to establish separate psychosomatic/psychotherapeutic inpatient units at general hospitals, but suggested another mode of cooperation:
Differing models are in existence: (1) the consultation model, (2) the liaison model and (3) theworkgroup model (extended model of the liaison service that provides continuity).… the expert commission recommends the establishment of liaison services at general hospitals staffed by specialists. Under this term one understands physicians with specific areas of continuous education in psychotherapy or psychoanalysis who have qualified knowledge of the respective medical discipline to be served. [7, pp.554f]
Liaison models with part-time employment of medical psychotherapists or psychiatrists who otherwise work out of their own ambulatory office were considered especially worthwhile under the aspect of continuity of care.
History of consultation–liaison psychiatry in Germany: beginnings
The first comprehensive report on the problems of integrated psychiatric services in a general hospital in the Federal Republic of Germany was presented by Radebold [8] from Berlin in 1971, and is reminiscent of the work of Henry [9] in the US in 1929. It describes the path from initial opposition to a growing acceptance of psychiatrists by the staff of medical and surgical units (known in Germany as departments, and henceforth referred to as such), important factors being elements of liaison activity such as joint visits at the bedside. A first systematic overview of ‘practical’ consultation psychiatry was published in the second edition of the German handbook of ‘Contemporary Psychiatry’ in 1975 by Bönisch and Meyer [10] under the title ‘Extreme situations of medical treatment’. It announced the expectation of an increasing importance of psychiatric liaison activity in a general hospital, in view of the developments of modern technological medicine. Wherever, rarely enough in those days, psychiatric units were installed in general hospitals, somatic disciplines frequently used the opportunity to call a psychiatrist as a consultant. Within 6 years of its creation in 1970, the C-L psychiatry service at Steglitz University Hospital in Berlin encompassed a volume of 1571 initial consultations and 2687 repeat consultations for 1300 somatic beds [11].
In the wake of the psychiatrie-enquête
A survey of psychiatric units in general hospitals at the beginning of the 1980s showed the considerable extent of C-L psychiatric activities: for a typical psychiatric department with approximately 70 beds in a medium-sized hospital, one could assume approximately 600 consultations per year. In a large medical centre, the frequency of consultations was found to be up to 4000 per year [12]. But scientific contributions to C-L psychiatric themes remained rare until the end of the 1980s [13], [14]. They were confined mostly to the clinical aspects of singular disease entities, where the necessity of interdisciplinary studies with respect to the prevalent psychopathological syndromes and psychological problems was proposed, especially in the areas of oncology, haemodialysis and heart surgery [see 15]. Occasionally, an orientation toward the North American model of C-L psychiatry was suggested [15].
Contributions on the organization and functioning of C-L psychiatry services remained rare [13]. There were occasional descriptions of the functioning of single C-L psychiatric services and aspects of C-L service delivery in the context of models of inpatient crisis intervention in general hospitals. A remarkable exception was the aftercare of suicidal patients: a series of publications showed urgently the necessity of continuous aftercare of patients following suicide attempts, according to a model of C-L psychiatric liaison services working with inpatients as well as outpatients [16].
Recent developments
Since the beginning of the 1990s, the interest in C-L psychiatric questions in German psychiatry has increased. A series of reports about the activities of psychiatric C-L services in Germany was published
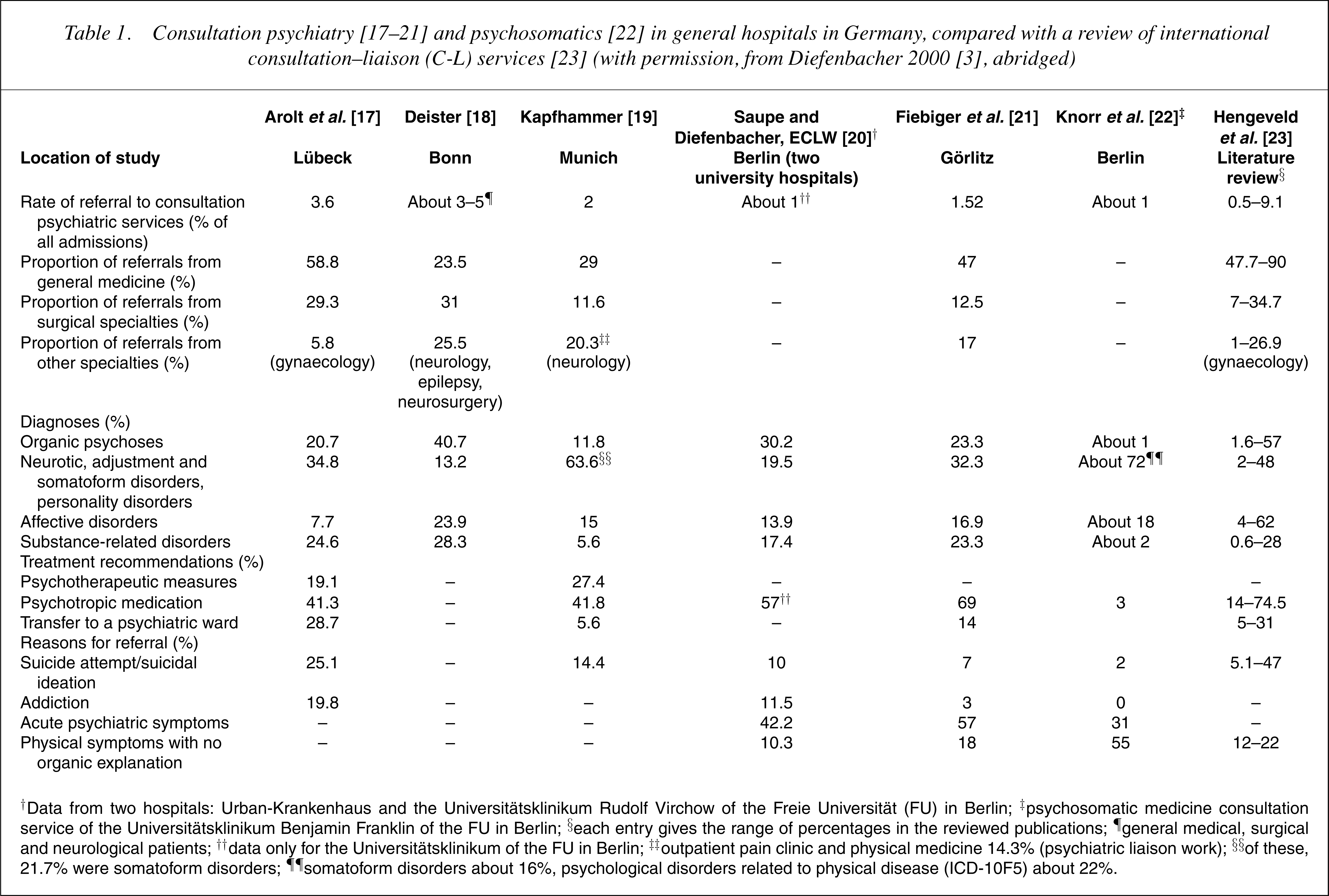
†Data from two hospitals: Urban-Krankenhaus and the Universitätsklinikum Rudolf Virchow of the Freie Universität (FU) in Berlin; ‡psychosomatic medicine consultation service of the Universitätsklinikum Benjamin Franklin of the FU in Berlin; §each entry gives the range of percentages in the reviewed publications; ¶general medical, surgical and neurological patients; ††data only for the Universitätsklinikum of the FU in Berlin; ‡outpatient pain clinic and physical medicine 14.3% (psychiatric liaison work); §§of these, 21.7% were somatoform disorders; ¶¶somatoform disorders about 16%, psychological disorders related to physical disease (ICD-10F5) about 22%.
In 17–21] and one psychosomatic [22] C-L services are compared with the scope of international C-L service delivery as outlined by a literature review [23]. It shows that German psychiatric C-L service delivery is in accordance with international C-L service delivery, whereas the German psychosomatic C-L service does see virtually no patients after suicide attempts, nor patients with organic mental syndromes or substance abuse (cf. also Table 4).
In general there was an increase in research reports on aspects of the care of special patient groups in the general hospital with increased mental comorbidity, for example, alcohol-dependent and geriatric [24], geriatric [25], alcohol-dependent [26], [27], neurological–epileptological [28], pain [29] and oncological patients. For the care of the latter groups, significant contributions also came from medical psychological services [30].
As the number of psychiatric units or departments in general hospitals doubled from 61 in 1979 to 125 in 1995, C-L psychiatric services increasingly lived up to the function of making the field of psychiatry, with its diagnostic and therapeutic possibilities, transparent for the somatic disciplines. They also strove to reduce prejudice against the mentally ill and the (pessimistic) ignorance about psychiatric treatment success, that is, they tried to overcome the stigmatization of psychologically ill patients. The workgroup of the directors of psychiatric departments at general hospitals (http://www.ackpa.de) has established a solid position for the theme of C-L psychiatry in the context of its annual meetings. Since 1992, at the scientific meetings of the German Society for Psychiatry, Psychotherapy and Neurology (Deutsche Gesellschaft für Psychiatrie, Psychotherapie und Nervenheilkunde [DGPPN], http://www.dgppn.de), a C-L psychiatry symposium has been held regularly. Consultation–liaison psychiatry and psychotherapy are receiving increasing attention in psychiatric textbooks [31], [32]. Concise guides on ‘Practical Consultation Psychiatry and Psychotherapy’ have been published [33], [34], as well as a comprehensive textbook [35]. With increasing tendency, C-L psychiatry is being conceptualized as part of a community psychiatric care system and emphasis is being placed on the filter function of the general hospital and implicit role of psychiatric consultation services in the diagnosis of heretofore unrecognized treatable mental disorders [36], [37]. Also, reports on C-L psychiatry activities performed by departments of child and adolescent psychiatry, which is a separate medical specialty in Germany, have been published [38]. In a memorandum, the German Society for Psychiatry, Psychotherapy and Neurology (http://www.dgppn.de) emphasized the importance of psychiatric–psychosomatic C-L services for the general hospital [39].
Psychiatry and psychotherapy and psychosomatic and psychotherapeutic medicine: a German conundrum
With regard to psychiatry and psychosomatics there are several peculiarities in Germany.
First, while it is generally known that there is no international agreement on how to define the concept of psychosomatic medicine; in Germany, there are at least three different definitions in use, as Malt [40] has summarized recently: psychosomatic medicine defined as ‘biopsychosocial or holistic medicine’, as ‘psychological conflicts causing physical dysfunction and disease’, or simply defined as ‘psychotherapy’. According to Malt [40], the latter definition is the most confusing from an international viewpoint as many German textbooks of ‘Psychosomatic Medicine’ are nothing but regular psychiatric textbooks of non-psychotic (‘neurotic’) disorders with a strong emphasis on psychological and psychotherapeutic issues. Thus, a psychiatrist who works only with patients with neurotic disorders in private practice may call himself or herself a psychosomaticist, especially if he or she hardly ever uses medication even if mostly treating patients with anxiety or depressive disorders, and even if not treating patients with unexplained physical symptoms at all.
Second, it seems not at all understood abroad that psychiatry and psychotherapy and ‘psychotherapeutic medicine’ became two separate medical specialties in Germany only in 1992. In that year, following a decision by the German council of physicians (Deutsche Ärztetag), another distinct medical specialty was created in addition to that of psychiatry for the care of patients with psychiatric disorders; the former is called ‘physician for psychiatry and psychotherapy’ (Facharzt für Psychiatrie und Psychotherapie), and the latter ‘physician for psychotherapeutic medicine’ (Facharzt für psychotherapeutische Medizin), also sometimes called ‘psychosomaticist’ as the specialty is called psychosomatics and psychotherapeutic medicine.
Physicians according to specialities (as of 31 December 2002)
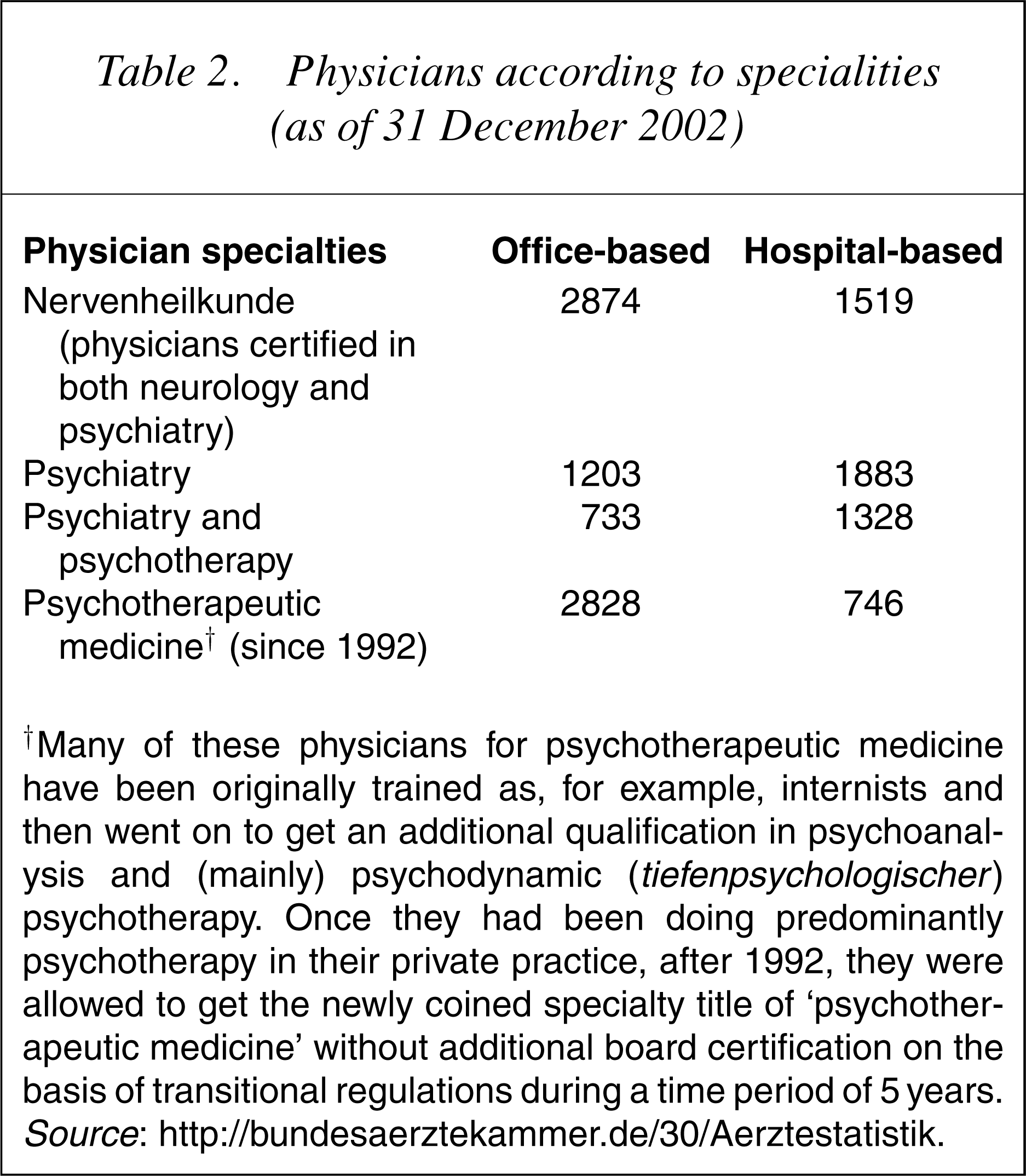
†Many of these physicians for psychotherapeutic medicine have been originally trained as, for example, internists and then went on to get an additional qualification in psychoanalysis and (mainly) psychodynamic (tiefenpsychologischer) psychotherapy. Once they had been doing predominantly psychotherapy in their private practice, after 1992, they were allowed to get the newly coined specialty title of ‘psychotherapeutic medicine’ without additional board certification on the basis of transitional regulations during a time period of 5 years. Source: http://bundesaerztekammer.de/30/Aerztestatistik.
About 15 years ago, because of the growing complexity of both psychiatry and neurology, several transitional ruleswere put forth and the German Medical Board (Bundes ärztekammer) separated that joint specialty into two separate ones, neurology and psychiatry. Psychiatrists now have to specialize in a specific psychotherapeutic technique, either behaviour therapy or psychodynamically oriented psychotherapy; hence their designation is physician for psychiatry and psychotherapy. During a limited time period after its inauguration in 1992, the newly coined title of physician for psychotherapeutic medicine was conferred to those physicians (psychiatrists, family practitioners, internists or gynaecologists, to name but a few) who had gained the added qualification of psychotherapy and/or psychoanalysis, and had worked for a certain period of time with psychotherapeutic techniques. In 2003, the German Medical Council decided to rename this specialty as ‘physician for psychosomatic medicine and psychotherapy’. 75].
The training in each medical specialty takes 5 years, with a compulsory year of neurology for psychiatry and psychotherapy, and a compulsory year of both internal medicine and psychiatry and psychotherapy for ‘psychosomatic medicine and psychotherapy’. In 2000, residents in training for psychiatry and psychotherapy (n=3796) by far outnumbered those for psychotherapeutic medicine (n=153) [42]. There is an overlap of a 90% between specialties; and this has led to the criticism that the two-stranded system is confusing to both patients and fellow physicians [42], [43].
Consultation–liaison psychiatry and consultation–liaison psychosomatics in Germany: separate but equal?
Outside Germany for many years there has been the erroneous assumption that German psychosomaticists are responsible for C-L psychiatry service delivery in general hospitals. In fact, this was never the case, and for a long time those psychosomatic specialists who were active in C-L psychiatrywork even expressed their disappointment that the psychosomatic consultation service… has to be regarded in several ways as the neglected child of psychosomatic medicine. Therefore many colleagues are glad when they can delegate this work which often appears senseless, frustrating, and does not seem to lead to much feedback. [44]
Wirsching and Herzog [45] emphasized that ‘so far the rather problematic perhaps even neglected area of cooperation of psychosomatic medicine with general clinical medicine in so-called C-L services (experienced) an unexpected boost only at the end of the 1980s’. Herzog et al. [46] published recently guidelines for ‘C-L psychosomatics and psychotherapy’.
Discussions between C-L psychiatrists and their psychosomatic counterparts in Germany remained rare during that period. Individual psychiatrists tried to define their relationship with psychosomatic medicine, for example, Blankenburg [14] who would have preferred to ‘see psychiatry as a subdiscipline in a larger psychosomatic field’, or Böhnisch and Meyer [47] who reported, under the title ‘Psychosomatic medicine in clinical medicine’, on psychiatric–psychotherapeutic experiences with severe somatic diseases. But this did not initiate deeper cooperation.
Both specialties care for psychiatrically ill patients. Because of their numerical superiority, psychiatrists deliver most of the C-L services in general hospitals, covering the whole gamut of the diagnostic spectrum [76]. Psychosomaticists focus more on referrals for unexplained physical symptoms, but not exclusively. However, for this group of patients, as well as for patients suffering from depression, there is a large overlap with psychiatric CL services [48]. There are no algorithms for differential referrals, with an ensuing uncertainty whether, for example, patients with depression receive comprehensive treatment combining psychotherapy and antidepressant medication, as pertinent for psychiatric C-L services, or psychotherapy alone, as is so for psychosomaticists [22], [49]. Comparative studies of the outcomes of either service delivery for special diagnostic categories would be interesting but, to the best of this author's knowledge, have not been carried out. It is estimated that 95% of existing general hospital C-L services are provided by psychiatry and 20% by psychosomaticists, obviously with some overlap [50]. Of note, while many university hospitals have both psychiatric as well as psychosomatic departments, this does not hold true for non-university general hospitals where there are many more psychiatric than psychosomatic departments. The last survey (carried out by the end of the 1980s) found 11 psychosomatic and 78 psychiatric departments [51]. Because of the establishment of the two separate physician specialties in 1992, there has been a slight increase in psychosomatic departments in general hospitals in some of the German states, but plans to increase their number in addition to psychiatric departments remain controversial.
State of consultation–liaison (C-L) service delivery in 1988–1989 in West Germany (according to Herzo and Hartmann, 1990 [51], modified)
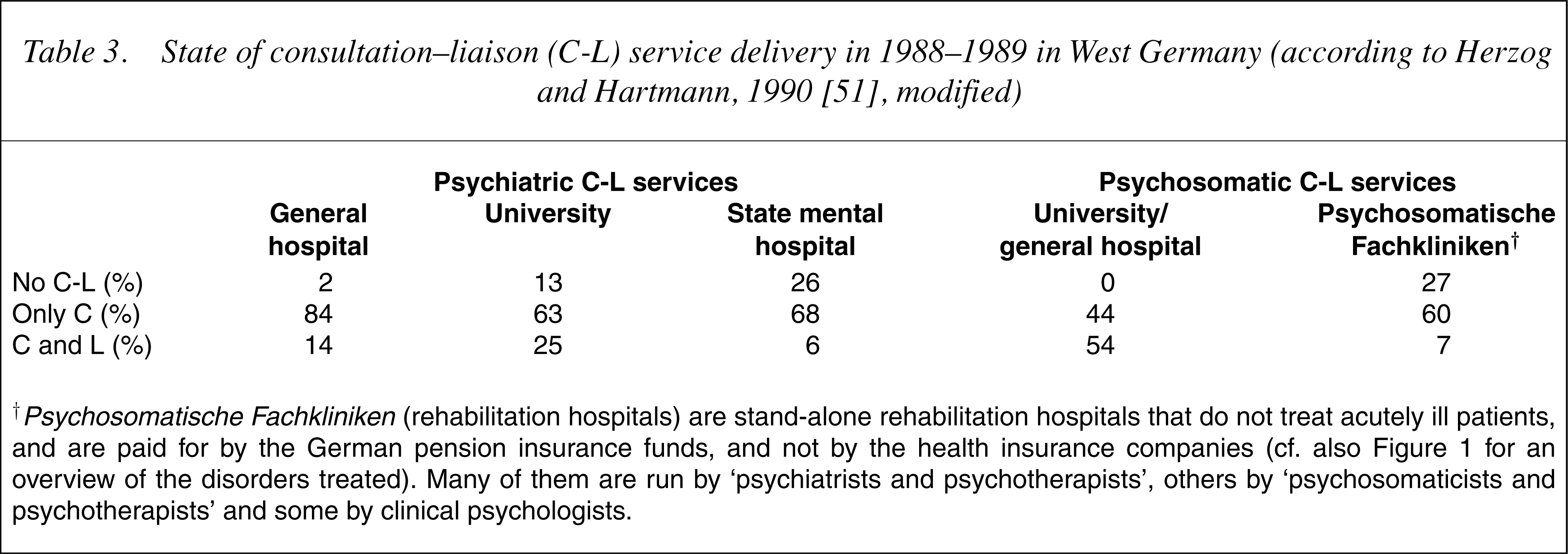
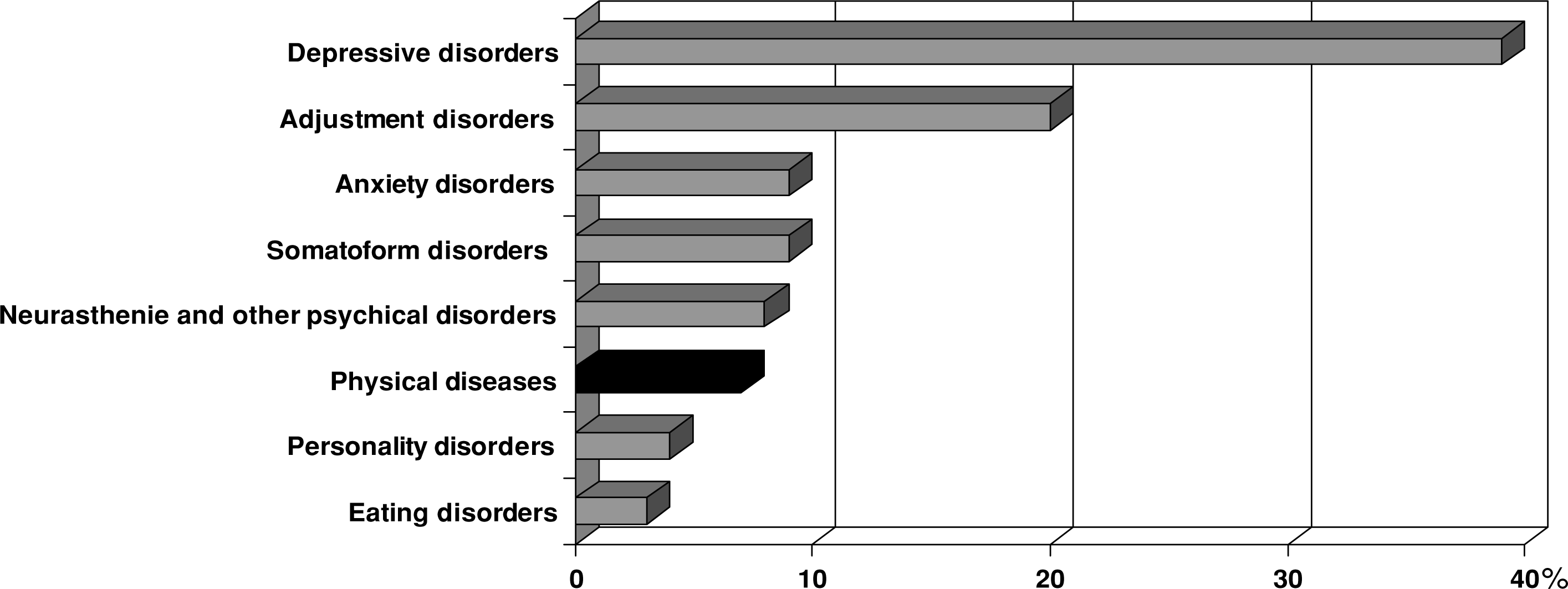
†Psychosomatische Fachkliniken (rehabilitation hospitals) are stand-alone rehabilitation hospitals that do not treat acutely ill patients, and are paid for by the German pension insurance funds, and not by the health insurance companies (cf. also Figure 1 for an overview of the disorders treated). Many of them are run by ‘psychiatrists and psychotherapists’, others by ‘psychosomaticists and psychotherapists’ and some by clinical psychologists.
Comparison of psychiatric and psychosomatic consultation–liaison (C-L) services in Germany
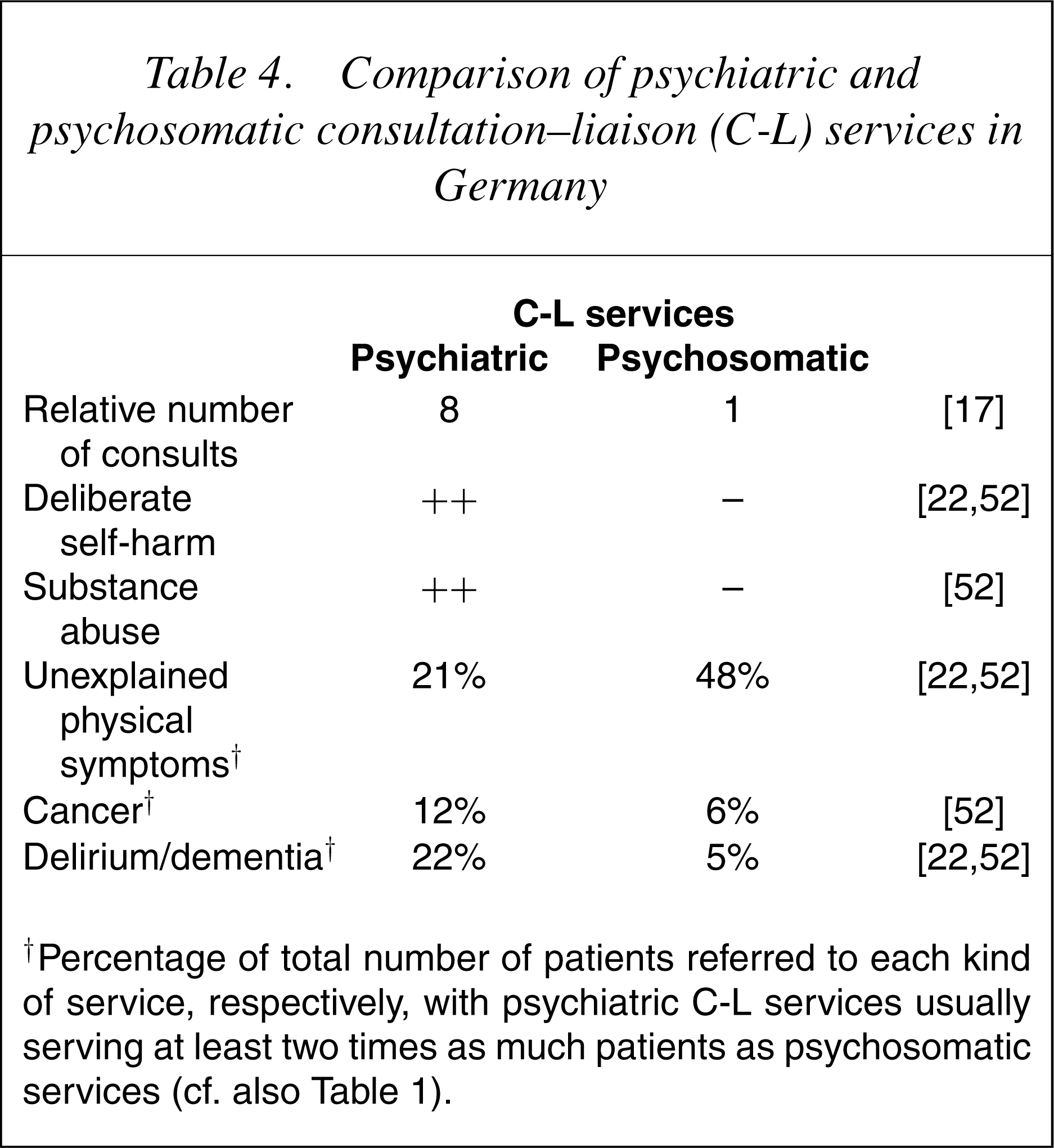
†Percentage of total number of patients referred to each kind of service, respectively, with psychiatric C-L services usually serving at least two times as much patients as psychosomatic services (cf. also Table 1).
In the ECLW study, a cluster analysis of variations in the characteristics of patients referred to 56 C-L services in 11 European countries yielded two types of service delivery: one ‘psychosomatic’ and one ‘psychiatric’ [52]. Although the German psychiatric C-L services fit well into the European ‘C-L psychiatric cluster’, genuine psychosomatic service delivery remained a peculiarity of the German psychosomatic C-L services, with such services seeing virtually no deliberate self-harm patients, only a small percentage of substance abuse patients and a very low percentage of patients with organic mental syndromes. Their main focus was dealing with unexplained physical complaints which, on the other hand, was also an important function of German psychiatric C-L services [17], [19] (cf. 22], [49].
Although one might assume that the coexistence of both service types at a number of hospitals in Germany should have paved the way for comparative outcome studies of different approaches in a natural setting, this unfortunately was not the case. There are no scientific studies on differential indications for referrals to either service [17]. Patterns of respective referrals develop in everyday clinical practice, according to the given quality of cooperation of both services. This means, on the other hand, that referring doctors do not usually have sound criteria on how to decide which way their referrals should go, with the consequence of getting double consultations, or switching C-L services according to whether one is satisfied with a given recommendation or not, which may lead to ensuing risk of conflicting treatment recommendations and the prolongation of length of stay [36].
With each other or against each other?
The existence of a two-stranded service delivery system for psychiatrically ill patients in Germany has led to an abundance of literature serving the interests of the members of each discipline. This might help in preventing psychotherapy from being overwhelmed by biology, as Malt has argued [40]. But unfortunately, the last few years have seen a rise of unfriendly spirits between the two disciplines. Thus, in a reaction to the memorandum of the German Association for Psychiatry, Psychotherapy and Neurology, which favours a reintegration of ‘Psychotherapeutic Medicine and Psychosomatics’ into Psychiatry and Psychotherapy, for example, as an added qualification within a common trunk of psychiatry, representatives of the German Society for Psychotherapeutic Medicine evoked the picture of a long-gone custodial psychiatry and argued that within the German tradition:
psychiatrists and psychotherapists are fundamentally different.… The latter being more sensible, receptive, compassionate, and oriented towards the individual, the former instead more norm oriented and prone to action. This contradiction cannot easily be solved by dual qualification. ([53], translated by the author)
In a recent press release commenting on the reorganization of psychosocial C-L service delivery in Berlin, where some psychosomatic services were integrated into psychiatric departments, a representative of the Association for Psychosomatics and Psychotherapeutic Medicine (Deutsche Gesellschaft für Psychotherapeutische Medizin [DGPM]) argued that ‘psychosomaticists hardly see any points of contact with psychiatry’, and that psychosomatic C-L service delivery fundamentally can only be performed by ‘physicians for psychosomatic medicine and psychotherapy’. They argued that it is irresponsible to permit these services to be delivered by psychiatry, which it denounced as plainly pillmongering and hardly talking to patients, in contrast with the talking cure-oriented psychosomaticists that strictly would refrain from substituting a therapeutic relationships by psychopharmacological drugs (statement made by a spokesperson of the DGPM, quoted according KV-Blatt [Journal of Berlin Physicians] Berlin, 06/2004, p.35; translated by the author).
With regard to the psychological care for oncology patients by C-L psychiatry and C-L psychosomatics (cf. Table 4), this debate between the two groups is being criticized by non-medical professionals:
Psychiatrists and psychosomaticists both regard themselves as competent, and prone to care for oncological patients.… We meet a phenomenon: territorial claims proposed, but not realized. This persevering claiming of competence, that stays unfulfilled, actually prevents daily care. [54]
Interestingly, at this point of discussion between psychiatry and psychotherapy and psychosomatic medicine and psychotherapy, the well-known entanglement of psychiatry in the ‘Third Reich’, with regard to, for example, euthanasia of mentally ill patients [55], [56], still plays a role in the self-understanding of psychotherapeutic medicine. After the defeat of the Nazis, important figures such as the psychosomaticist Alexander Mitscherlich went on to implement humanistic psychotherapeutic approaches in German university medicine outside psychiatry (for the difficulties of this process, cf. for example [57], [58]. Some representatives of German psychotherapeutic medicine strongly refer to that historical tradition as crucial for the definition of their subspecialty [48], [59]. It is beyond the scope of this article, to discuss this further. (With regard to the professionalization of psychotherapy during the Third Reich, for example, the important role of the psychotherapeutic ‘Göring Institute’, readers are referred to, for example [57], [58], [60], [61].)
A new player: medical psychological consultation–liaison service delivery
In the last few years, medical psychology has become more visible in Germany, promoting behavioural medicine approaches in the treatment of patients with physical and psychiatric comorbidity, or unexplained physical symptoms [62]. Their role is still small by comparison with that of other C-L services, and limited mainly to university-based institutions, but their voices will get stronger in the future [63], [64], as the results of medical behavioural interventions applied by medical psychological C-L services are promising [65]. Medical behavioural approaches in patients chronic pain and alcohol addiction are used with increasing frequency [26], [30].
Outlook
Diagnosis-related groups and consultation–liaison psychiatry
As of 2004, a diagnosis-related group (DRG) reimbursement system will be introduced in all medical– surgical departments in Germany. For the time being, psychiatric and psychosomatic departments will be DRGexempt [36]. Despite the urgent demands by several psychiatric associations, it has still not been made clear how psychiatric C-L services will be reimbursed under the DRG conditions [66]. Of note, a recent study performed by the ‘Deutsche Angestellten Krankenkasse’, Germany's second largest medical insurance organization, shows that 33% of their members receiving a main psychiatric diagnosis were admitted to the somatic wards of general hospitals, most of them (19%) to internal medical wards [37]. Not surprisingly, the three largest groups came from the ICD-10 F10 (alcohol-related), F0 (organic mental syndromes) and F4 (neurotic, adjustment and somatoform disorders) diagnostic categories. These authors suggest an increase in psychiatric–psychosomatic C-L service activities, with special emphasis on, and the introduction of, short-term crisis intervention techniques for alcohol-abuse patients on internal medicine wards. However, they are skeptical about whether the DRG system, as it stands, would offer any incentive to make these changes [37]. Nevertheless, the fact that one of the largest health-care insurance companies in Germany has discovered the probable benefits of C-L service delivery for the comorbid physical/psychiatric patient in the general hospital is promising.
Other venues of consultation–liaison service delivery
General hospitals in Germany without a psychiatric inpatient department are mostly served by ambulatory care office-based psychiatrists who usually do consultation work (and not a liaison approach) on a contract basis. As most office-based psychiatrists are still also trained in neurology, they usually perform both psychiatric and neurological consults, which is quite helpful, for example, in the treatment of pain patients [67]. This form of service delivery may gain further importance as, under a new legislation, small-scale projects subsidized by health-care insurance companies may help to implement C-L service delivery by office-based psychiatrists in hospitals without psychiatric departments. This should bridge the still existing gap between inpatient and outpatient care in Germany. Hospitals are not usually allowed to deliver outpatient treatments on an ongoing basis. Physicians working in private practice hardly ever are able to manage their patients through an inpatient treatment episode, that being performed independently by hospital doctors.
In 2004, the number of psychiatric departments in general hospitals has risen to approximately 170, and is accompanied by increasing efforts of the additional 150 stand-alone psychiatric facilities to establish closer collaboration with nearby general hospitals, for example, by establishing medical–psychiatric units (MPUs). Although this term is not common within German psychiatry, MPUs have long been a feature of German psychiatric inpatient care, especially for psychogeriatric wards, and also for younger patients with severe physical/psychiatric comorbidity [4], [68]. The advantages of MPUs in providing concurrent but not sequential care (as is the case with the classical consultation approach) are being discussed under the perspective of the upcoming DRG system [69].
German psychosomatic wards are mainly located in rehabilitation centres (so-called Psychosomatische Fachkliniken, cf. 40]. In fact, the so-called psychosomatic rehabilitation hospitals (i.e. Psychosomatische Fachkliniken) mainly treat patients with non-psychotic psychiatric disorders, for example, depression, and only a small proportion of patients with somatic disorders (cf. Fig. 1) [70]. Of note, a quarter of such Psychosomatische Fachkliniken did not perform consultations to general hospitals (cf. Table 3).
Nurses are very seldom part of C-L psychiatric services but their integration has been proposed, as has that of social workers and other health-care professionals, not the least due to budget constraints [71].
Education and training
At present, there is no compulsory rotation of psychiatric residents in C-L services, though in most general hospitals with psychiatric departments, psychiatric residents do some C-L work. Hence, a curriculum has been published as a tool for organizing seminars in C-L psychiatry. It gives suggestions as to how to organize practical C-L training of residents [72]. At the annual meeting of the DGPPN, a C-L training seminar has been mounted on a regular basis since 1996.
Because of the interesting prospect of integrating behavioural medical approaches into C-L psychiatry, and with the DRG system looming large, the C-L psychiatric task force of the German Association for Psychiatry, Psychotherapy and Neurology has been relaunched as the ‘Section of Behavioral Medicine and Consultation Psychiatry’ within the DGPPN (chaired by Manfred Fichter, email:
Conclusion
It is this author's opinion that it is difficult to say what lessons could be learned for other countries from this quite peculiar approach of the, in part, two-stranded C-L psychiatry service delivery in Germany, given the present level of evidence about the relative efficacy. However, the following points are offered to stimulate discussion:
This author's conclusion is that the German experience of two distinct service approaches in the C-L setting is confusing to both patients and physicians, and stigmatizing for patients with severe (psychotic) psychiatric disorders. It fosters a deeply engrained turf mentality, and, with regard to medical psychologists, is at present hardly able to deal with the advent of an interesting and important group of non-medical professionals in the field of care for patients with psychiatric and physical comorbidity. It cannot, due to its special history, and should not, for conceptual and pragmatic reasons, be emulated in other countries.
With regard to psychiatric–psychotherapeutic service delivery in Germany, this author's opinion is that the two-stranded system of psychiatry and psychotherapy and psychosomatic medicine and psychotherapy should be reintegrated under a single ‘umbrella specialty’, named, for example, ‘physician for psychological disorders’. Within this specialty, subspecialties should be developed such as ‘addictive disorders’, and, for example, ‘C-L psychiatry and psychotherapy’, which also could be named, as only recently decided in the US, psychosomatic medicine. Such proposals are being discussed within the DGPPN, but are strongly opposed by the organizations for psychosomatic medicine and psychotherapy.
With regard to the two-stranded C-L service delivery that exists in some general and university hospitals in Germany, they should be integrated into one C-L service that is multidisciplinary and should embrace a wide range of interventions including the range of psychotherapies known to be effective. The director of such integrated C-L services could be either ‘psychiatrist or psychotherapist’, or ‘psychosomaticist and psychotherapist’.
Most interesting to this author, however, would be the discussion as to whether the traditional system of physician specialties for psychological disorders, as it has developed during the past 100 years, will stand the test of time. Would it not be worthwhile in the field of treatment and care for psychiatrically ill patients to rethink and probably reshape professional boundaries with respect to non-medical psychotherapists, especially clinical psychologists?