
Abstract
Keywords
Studies of community samples consistently report higher rates of depression in women than in men [1–5]. The often uncritical reporting of this gender disparity has led to certain assumptions about the mental health of both men and women. Women assume, or are assumed to have, a certain pathology or vulnerability to depression [6–8] while men are assumed to be comparatively healthy or ‘silent’ in their experience of depression. There is a risk that we may be overpathologizing women and, at the same time, underestimating men's ‘unique pain’ of depression [9]. Factors attributed to lower rates of depression in men include their ‘failing’ to report [10], [11] or ‘forgetting’ their symptoms [12], or problem recognition being inhibited [13]. Men are thought to have difficulty in verbally expressing their emotions, or are described as inexpressive [14], hypoemotional [15] or unable to identify and describe their feelings (alexithymia: [16]). Conversely, features or behaviours associated with depression are more frequently displayed or reported by women. These include crying, emotionality, mood amplification (due to ruminating response), expressions of helplessness and passivity and increased food intake [17–20].
Men are, however, over-represented in risk-taking and antisocial behaviours such as aggression and violencerelated deaths, deliberate self-harm and suicide, sexual encounters, gambling, drink-driving, road rage and drug and alcohol abuse including binge drinking [21–32]. Of interest, in communities where alcohol and drug use and sociopathy are culturally prohibited [33] or where there is low use of alcohol and suicide as escape routes from depression [34], the disparity between men's and women's reporting of depressive symptoms narrows. Behaviours such as aggression and violence and drug and alcohol abuse, road rage and suicide (usually attributed to men), have been termed ‘depressive equivalents’ or ‘masked depression’ [35], [36], which suggests some association with ‘being depressed’ but not labelled as depressive symptoms. The ‘reporting of’ depressive symptoms by men may therefore not be the same as the ‘experience of’ depression in men. The link between what men ‘feel’ and what men ‘do’ when they are depressed seems not to have been explored.
‘Depression’ is used in both common language and the psychiatric literature, but not always with the same meaning [37]. The current classification systems (DSM-IV and ICD-10) have been more concerned with issues related to reliability and validity of diagnostic categories of depression than with the subjective meaning of depression. There is a need to return to the task of discriminating between the subjective experience of depression, the reporting of depressive symptoms and the meaning attached to the experience of depression. To enable a greater understanding of men's experience of depression, Cochran and Rabinowitz [35] suggested an appropriate strategy was to ‘simply ask men’ but few studies have done so. Where qualitative techniques have been used to explore men's views about mental health and physical health issues [39], [40] men's stoicism and reluctance in talking about health issues has been emphasized, pointing to challenges in detecting depression in men. This study sought to add ‘meaning’ to the gap between the ‘manifestation’ and ‘measurement’ of depression using men's own words.
Method
Sample
A convenience sample of teachers and students was recruited to discuss their experience of being ‘down in the dumps’ and how they managed the symptoms. The participants were drawn from four sites of a tertiary education institution (Institutes of Technical and Further Education) in the northern, southern, western areas of Sydney and the Illawarra region of New South Wales. Deans and head teachers of institutes sampled were provided with an overview of the study, assurance that participants' attendance was voluntary and withdrawal could occur any time. They were informed of the objective and process of the study and what participants' involvement would entail. A poster, which outlined the study, was given to teachers to display or to disseminate to generate interest in other teachers and students. Prospective participants were contacted by telephone and then with a follow-up letter confirming date, time and venue for the discussions. At the initial face-to-face meeting with participants, information about the study was repeated. They were also given the opportunity to ask questions, to clarify issues and to voice their views and concerns about aspects of the study. Onsite counsellors were advised that the study was going to take place should the need for counselling for participants arise. Compact disc music vouchers were offered in appreciation of participants' time and personal involvement in the study and they were offered a summary of the findings of the study. Approval to recruit the sample and to conduct the study was granted by the Ethics Secretariat, University of New South Wales (Approval No. 99099).
Data collection
Ten focus groups were conducted with men (four with teachers; six with students) and four focus groups were conducted with women (two with teachers; two with students). A schedule of open-ended questions was used to guide the group discussions and to generate qualitative data concerning the physical and emotional effects of being ‘down in the dumps’ (experienced and observed in others) and ways of managing the symptoms. ‘Down in the dumps’ is a descriptor used by DSM-IV criteria for depression [41]. Participants were also asked their observations of the effects of depression on the other gender. A selfreport questionnaire (completed before the group discussion) gathered sociodemographic information, including age, marital status and dependants, and behavioural variables including alcohol and cigarette use and self-rated health (out of 10). Two standard measures of mood (the positive and negative affect schedule [PANAS] [42]) and dispositional optimism (the life orientation test [LOT] [43]) were used to gauge the ‘non-clinical’ or ‘clinical’ status of the group.
All groups were led by the same facilitator (male counselling psychologist) to minimize variation in facilitator style. One of the authors (SB), a woman, acted as scribe for all 14 focus group discussions which were audiotaped. She also transcribed all of the men's group discussions verbatim and proceeded with the analysis. Once the men's data were analysed to the extent of distilling to the core category, she then transcribed all of the women's group discussions verbatim and analysed the data with reference to the men's data.
Data analysis
The men's qualitative data were analysed using a grounded theory approach [44], [45]. The analytic process is described in detail elsewhere [46]. In short, it is an inductive and iterative process of generating, examining and constantly comparing concepts and categories, for similarities and contrasts leading to ‘new’ discoveries and to explore underlying meanings attached to the phenomenon under study [47]. The iterative process continued until the categories were distilled into the core category that theorized men's experience of depression, grounded in the richness of the data. Verbatim quotes (in italics) from the language or words used by the participants, were retained in order to stay as close as possible to the meanings men attached to their experience of depression.
The women's data were analysed using content analysis [48] with reference to a priori categories generated from the men's data. The use of a priori categories generated from the grounded theory is considered an acceptable approach to content analysis [49]. Thus, the categories generated from the men's data provided a theoretical foundation about the experience of depression against which to analyse the women's data. The process of content analysis proceeded through four stages: the first stagewas to identify patterns within the women's data of women describing their experience of depression and their observations of men who were depressed. The second stage was to examine for consistency in the data. The third stage was to identify patterns, for example, of ‘avoidance’ in the women's data that would be similar to the men's category (generated from the grounded theory) of avoiding ‘it’. The fourth stage was to interpret the themes in a way that would contribute to the development of knowledge, specifically, men's experience of depression.
Results
Seventy-seven men participated in this study (teachers n=27; students n=50). The teachers' and students' average age was 48.4 years (SD=5.5) and 20.4 years (SD=3.8), respectively. The trade certificate courses included horticulture, aircraft, automotive, autobody, carpentry, building, electrical, mechanical engineering, industrial electronics, metal fabrication and welding. All men scored high positive affect (teachers: mean=16.8 [SD=2.8]; students: mean=16.6 [SD=3.1]), 82% scored low negative affect (teachers: mean=8.1 [SD=2.8]; students: mean=9.6 [SD=3.3]), 93% scored high dispositional optimism scores (teachers: mean=20.4 [SD=4.7]; students: mean=18.2 [SD=4.9]) and all scored high self-rated health (out of 10) (teachers: mean=7.7 [SD=1.1]; students: mean=6.7 [SD=2.1]). There were no differences in these scores between the young and older men (PA [positive affect]: t=−0.38, p=0.79, CI=−1.69, 1.15; NA [negative affect]: t=1.97, p=0.25, CI=−0.02, 2.96; LOT: t=−1.91, p=0.57, CI=−4.51, 0.10) except for self-rated health where teachers scored higher (t=−2.37, p=0.02, CI=−1.93, −0.16).
Twenty-five women participated in this study (teachers n=15, students n=10). The average age of teachers was 46.1 years (SD=6.1, range=38–61, median=45) and students was 37.6 years (SD=14.2, range=18–56, median=40). These women taught, and studied, in office administration and information technology courses and some students were retraining to re-enter the workforce. Ninety-five per cent of the women scored high positive affect (teachers: mean=17.2 [SD=2.8]; students: mean=17.6 [SD=5.2]), 67% lownegative affect (teachers: mean=10.2 [SD=3.6]; students: mean=8.7 [SD=4.1]), 82% scored high dispositional optimism scores (teachers: mean=18.8 [SD=4.1]; students: mean=18.6 [SD=4.5]) and all women scored high self-rated health (teachers: mean=7.9 [SD=1.5]; students: mean=8.1 [SD=1.0]). There were no differences in their group scores (PA: t=0.25, df=23, p=0.80, CI=−2.88, 3.68; NA: t=−0.96, df=22, p=0.35, CI=−4.79, 1.76; LOT: t=−0.11, df=23, p=0.91, CI=−3.80, 3.40; health: t=0.37, df=23, p=0.71, CI=−0.92, 1.32). Overall, these results suggested a non-clinical status (i.e. absence of clinical treatment for and observation of depression) of both men and women.
The men's qualitative data were examined and analysed first to generate a theory of depression in men from the ‘ground up’. During the course of the discussions, both young and older men described experiencing all the commonly accepted symptoms of depression [49]. These symptoms included inability to think, loss of concentration (not being able to kick the ball straight; I put up a wall that was three inches out of plumb), being irritable, self-critical, sad or moody, loss of interest or lacking drive, being restless or lethargic, weight loss or gain, changed sleep patterns, low self-esteem, feeling helpless and having suicidal thoughts or attempting suicide.
In response to the question, ‘how can you tell… what do you notice in other men who are down in the dumps’, these men identified external signs including body language of slumped posture (shoulders are down), unkempt appearance (don't wash their clothes; hygiene), untidy environment (everything gets messy; it just snowballs), change in character, attitude, or mood (not their normal self; having a long face; being like an outside shell; having a blank look, being able to see it in their eyes; facial expressions), getting way behind at work or school and withdrawal (being absent emotionally – like they're somewhere else, like there's nothing there) or being physically absent from work due to illness.
The word ‘depression’ was used by the men in this study to describe a range of feelings or emotions such as grief (the biggest depression I've had is my grandmother died; my mum left my dad for my dad's cousin); annoyance (the only thing I get depressed about is when my family gangs up on me and I can't watch the news); rejection (getting dumped by your girlfriend you probably get depressed); alienation (I never got along with my parents therefore I couldn't be at home so I was always depressed); isolation (living by yourself, you're depressed, you've got no-one to talk to); disappointment (I didn't do as well as expected and I was depressed); defeat (I used to get quite depressed when my football team got beaten); insecurity (you might not have had a job for 6 months, you're going to be really depressed about that) and desperation (when people are depressed they drink more, they do drugs, they're probably just crying out for help).
A grounded theory analysis moved beyond descriptive analysis to elucidate the meaning and process of depression in men. That is, in addition to the commonly accepted symptoms of depression [49], the men described an escalation and intensification of negative affect. This section draws heavily on men's own words as the data from which analytic conclusions have been derived. The major categories derived from the data are presented. Each category exists discretely but also combines within the ‘core category’ which links and synthesizes ‘the whole’ (Fig. 1).
Synthesizing men's experience and expression of depression with clinical knowledge and ‘depressive equivalents’.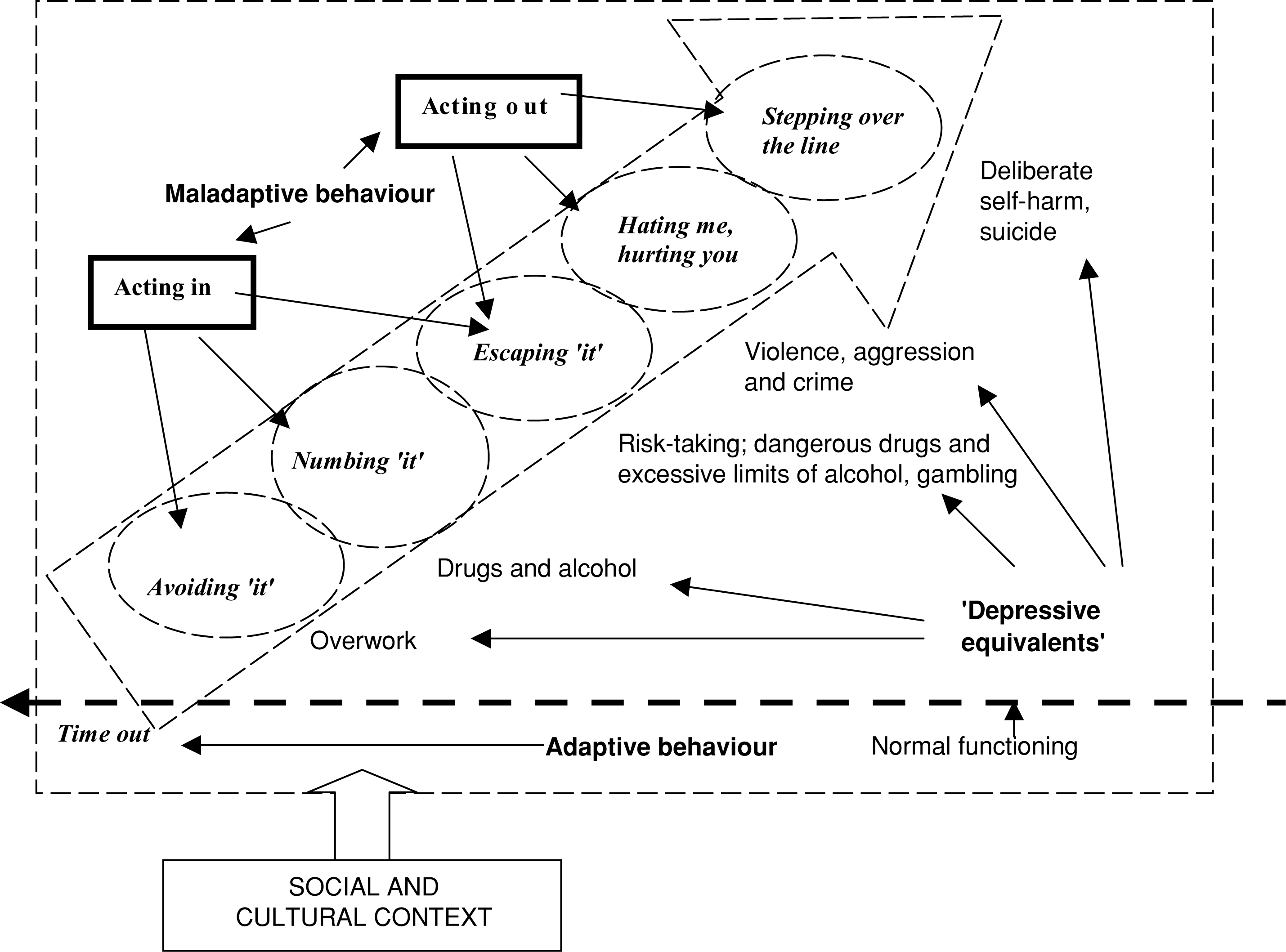
Avoiding ‘it’
Words in italics are taken directly from the raw data. The responses from men and women are reported in the text in the first, second and third person pronouns and indicated with (S) for student data and (T) for teacher data.
The men in this study reported avoiding problems or issues by not thinking about them, forgetting about them, or by distancing and distracting themselves from the problems by doing ‘other things’.
There's the ‘avoid’ the issue. Issue avoidance or try and forget about it altogether. You just don't recognise the problem. You just hope that it will go away. (T)
You just try to keep busy, don't think about it, just sit around doing things…. Work, surf, just stuff that takes your mind off everything else. (S)
However, avoidant behaviour such as avoiding work or putting more effort into work or burying themselves in work, or overwork (often rewarded as conscientiousness), also had the potential for personal, social or health consequences.
Just the absence of a person… could be just going sick from work, if they've got a problem. (T)
… you ‘wear it’ at work… you ‘wear it’ at home… [that is, endure criticism]. (S)
Numbing ‘it’
Both young and older men reported drug and alcohol use to relieve their emotional distress, although the younger men were more conversant with recreational drugs and the effects and ramifications of their use.
Drinking… it numbs it for a while. (S)
When you're stoned, you're more relaxed, right? When you're on ecstasy you're running around. When you're on cocaine you're running around. When you're on speed you're running around. When you're on heroin you're bl-e-r-k. [Splat. That's it!]…. You don't care any more when you get to heroin. You're gone. (S)
A lot of guys drink a fair bit more… and sort of neglect the problem and just drink it away. (T)
The means of escape they identified becamemore drastic when numbing ‘it’ (i.e. self-medicating emotional distress) became ineffectual.
Escaping ‘it’
Both young and older men attempted to escape from the pain, people, problems, pressures, hurt, loneliness and violence.
Anything to escape… anything just to get rid of the hurt and pain and loneliness… smoking pot, you just don't care… I don't care that it's gonna come back. When it comes back I deal with it again and then I take something else to escape. (S)
I got away from my old man. I put it all down to drugs and everything else. I just had to escape. (S)
The older men, either as having direct or indirect negative experience of risk-taking, or a result ofmaturing and having family responsibilities, tended to curtail their risk-taking behaviour. They would, however, adopt other ‘escape’ behaviours, such as increased hours spent at work, or act out of character, for example, engaging in extramarital affairs or reverting to adolescent behaviour.
It was total escape. He, he quite clearly could not cope in any way, shape or form, so he just reverted to his childhood… doing what he had done when he was a teenager [buying a surfboard and surfing all day]. (T)
I just go to the garage and play with my cars. [laughs] (T)
Prolonged periods of suppressing or escaping from negative emotions or problems resulted in an accumulation of problems and psychological distress or emotional pain for these men. As a result of keeping in or internalizing problems, letting problems smoulder, bottling or locking things up, both young and older men experienced a build up of their negative emotions.
Men tend to let things build up… and it all catches up with you and bang! (T)
I'll probably keep two or three problems together,… until it boils over with a bit more force, I guess, than necessary. (T)
We [men] hold it all in until we can find an outlet… (S)
Hating me, hurting you
The release of this ‘build up’ of emotions or problems was likely to be triggered by a negative external event, recognized and acknowledged as being injurious to self or having deleterious effects on others.
… they [men] let it build up and then they just snap… they don't snap in a small way. They'll take ‘em out [exert physical violence] sort of thing, in a big way. (S)
You take it out on the wrong people. (T)
Both groups of men reported self-abuse in the form of having a selfdestructive streak, being down on the self, or having a don't care attitude toward physical and mental health and wellbeing. The younger men reported more anger-related behaviours including rebellion, crime and aggression, breaking or smashing things and lashing out. The following quotes depict the experience of road rage and self-harm.
Like, don't be on the road when I'm on the road,… Everyone around me, just get off the road and get away from me. (S)
Most [men] don't really care if they do go over the edge … you'll see his speedo going up and up and you get more of a rush… you might see a tree up ahead. You focus on that tree, you look at the tacho [tachometer]. If you've gone over the edge then you know how much time you've got before you collect [crash into] that tree… (S)
These men suggested that this externalization of problems can have an effect on other individuals or objects close by.
It's a sort of anger, inappropriate anger it is, out of character…, that anger and intolerance were built up but it was directed in areas that you wouldn't expect them to have been directed. (T)
Just hit something, break anything… you break things… smash something, smash bottles… yeah, just release some anger… you just lash out real bad. (S)
Stepping over the line
The ultimate escape for some men was self-harm (experienced) or suicide (observed in others). The metaphors or euphemisms men used to describe suicide included stepping over the line, crossing the line, being on the edge, over the edge, or off the edge, going under, one other step or getting to a point or stage. The methods used to suicide included overdosing, guns (which make suicide easy – a one second operation), slitting/slashing wrists (which takes time), gassing [carbon monoxide poisoning], hanging, crashing or jumping [off buildings or bridges].
I had a mate who was going along [a] bridge, and asked his mum to pull over… he was on the way to relatives… he jumped over the bridge and killed himself. No reason. (S)
He took his dog for a walk and someone found him hanging from a dog leash, but there was no warning. There was no note. (S)
Suicide in others often came unexpectedly, without obvious reason and was difficult to detect or predict and left others feeling guilty or helpless (it's too late). Some who had been indirectly affected by it considered suicide a weak option (what other people think still matters) and others suffer because of it (it's not the way to go… you're put on this earth to do something).
The women in this study noticed that some men who are depressed avoid, numb and attempt to escape from problems. They suggested (as did the men) that kept in (suppressed) emotions get built up over time and can be released in the form of anger, violence or aggression with deleterious consequences for other men, women, children and pets. When women talked about their own experience of depression (and observations in other women), similarities emerged to those of the men's accounts. For example, the women identified or noticed that some women who are depressed avoid or escape from problems (by shopping), numb emotional distress (by taking prescribed medication) or lose control and lash out at children, or self-harm or suicide.
As a response to emotional distress, some men in this study (and observed by men in other men), take time out from problems that gives them a pause to put things into perspective. This appears to be an adaptive strategy that allows men time to think about [the problem], to weather it mentally, to work it through, or to try to solve the problem themselves. It also gives them a chance not to think about the problem, or to be in their own world for a while.
I think sometimes you need not to think about some things sometimes… you just need some time out, sort of thing. (T)
Other ways men minimized their problems or distracted from the problem in the short term was to do something active, doing physical things, for example, running, swimming, walking, riding the bike for miles, working on cars, or digging the spuds (potatoes). Being active was also considered a way to take the mind off the problem, get rid of the problem, clear the head, leave a person calmer to deal with issues, to then be able to talk about the problem when ready. These physical or active ways of coping with problems were considered by these men as a predominant function of men whereas women who were depressed were more likely to find comfort in food, to cry, or to seek help and ‘talk it out’.
The men and women in this study, particularly those who had experienced the depths of despair and helplessness, also spoke about a spiritual dimension to depression.
However, the women in this study spoke more freely about reliance on God and their practice of prayer to ‘offload’.
Prayer is helpful. I mean I think if I didn't have faith I would have gone off in a different direction. Praying enables you just to hand it over. It's not all on my shoulders. (S)
This practice seems to reinforce women's general propensity to seek help and to admit to needing help while emphasizing men's reticence to seek help and need to keep control of situations and feelings.
Discussion
The men's understanding of ‘depression’ involves a complex interaction between the experience of emotional distress and their responses to it. Once responses to emotional distress become ineffective there is the likelihood that some men will employ behaviours that become increasingly risky, dangerous or life-threatening and are ultimately released through anger, aggression, violence and suicide. Such externally directed physical release of emotional distress marks the triggered response of suppressed or built up negative emotion. The women's data reinforces this trajectory of emotional distress as common in men.
The ‘big build’ is an interpretation of the interaction between internalized feelings and externalized behaviours [45]. This play on words depicts men's ‘strong’ outer physical appearance but, at the same time, belies men's inner distress. It is presented in 9], [36], [50], [51].
This trajectory of emotional distress common to men is aligned to Pollack's [9] description of a ‘male-type’ depression that includes an increase in the intensity or frequency of angry outbursts and the ‘male depressive syndrome’ proposed by Walinder and Rutz [52] comprising low stress tolerance, acting-out behaviour, low impulse control, substance abuse and suicide.
The ‘big build’ (common to men) can be juxtaposed with the literature on the range of risk-taking behaviour associated with men, shown in Table 1.
This is an important link because each of thesemanifestations of risk-taking behaviour (often not associated with men being depressed) can be located at different points on men's trajectory of emotional distress. For example, avoidant behaviour such as sickness absence [53] may be subtle and difficult to detect as an early signal of depression. ‘Overwork’ as a coping style that distracts or avoids problems is often rewarded by employers who inadvertently collude with depressedmen [36] by rewarding their ‘conscientiousness’. Furthermore, the interaction of depression with aggression and alcohol abuse, has been linked with suicidal ideation [38].
Problems measuring depression in men
We know from this study that men and women experience depression similarly with reference to DSM-IV criteria [49]. However, the expression of depression in men is more complex than depression defined (gender neutrally), by DSM-IV. Problems associated with measuring depression in men are related to hidden symptoms of depression, the wide-ranging repertoire of strategies that men employ to manage depressive symptoms and the arbitrary nature of the ‘big build’ (54], [55].
The questions currently used to detect depressive symptoms appear to measure something different in men and women. Depression in men seems to be hidden in antisocial and risk-taking behaviours including drug and alcohol abuse, deliberate self-harm, suicide, road rage, sexual encounters, gambling, binge drinking, aggression and violence often referred to as ‘depressive equivalents’ or ‘masked depression’. As Bennett and Bauman [56] point out, risk-taking behaviour such as risky sexual encountersmay function as an escape mechanism (escaping ‘it’), as an indirect expression of anger or as control over another person (hating me, hurting you), as a diversion (avoiding ‘it’), or to relieve tension and as a salve of affection seeking – a sort of self-medication (numbing ‘it’). In this regard, detecting depression in men is likely to be made more difficult to identify because some maladaptive behaviours in response to depressive symptoms may be socially sanctioned and therefore masked.
Juxtaposition of the ‘big build’ with the literature referred to as ‘depressive equivalents’
In addition, constrained emotional distress, the process at the core of the ‘big build’, is likely to make depression even more difficult to detect or measure in men because of its latent or arbitrary nature beyond the ‘2-week’ period established by DSM-IV criteria [49]. Furthermore, the meaning of depression is extended by Angst and Merikangas [57] who have argued for a more multidimensional approach to the classification of depression. This multidimensional approach is captured by Solomon's [58] description of his depression, as follows (Fig. 2).
Multidimensional aspects of depression.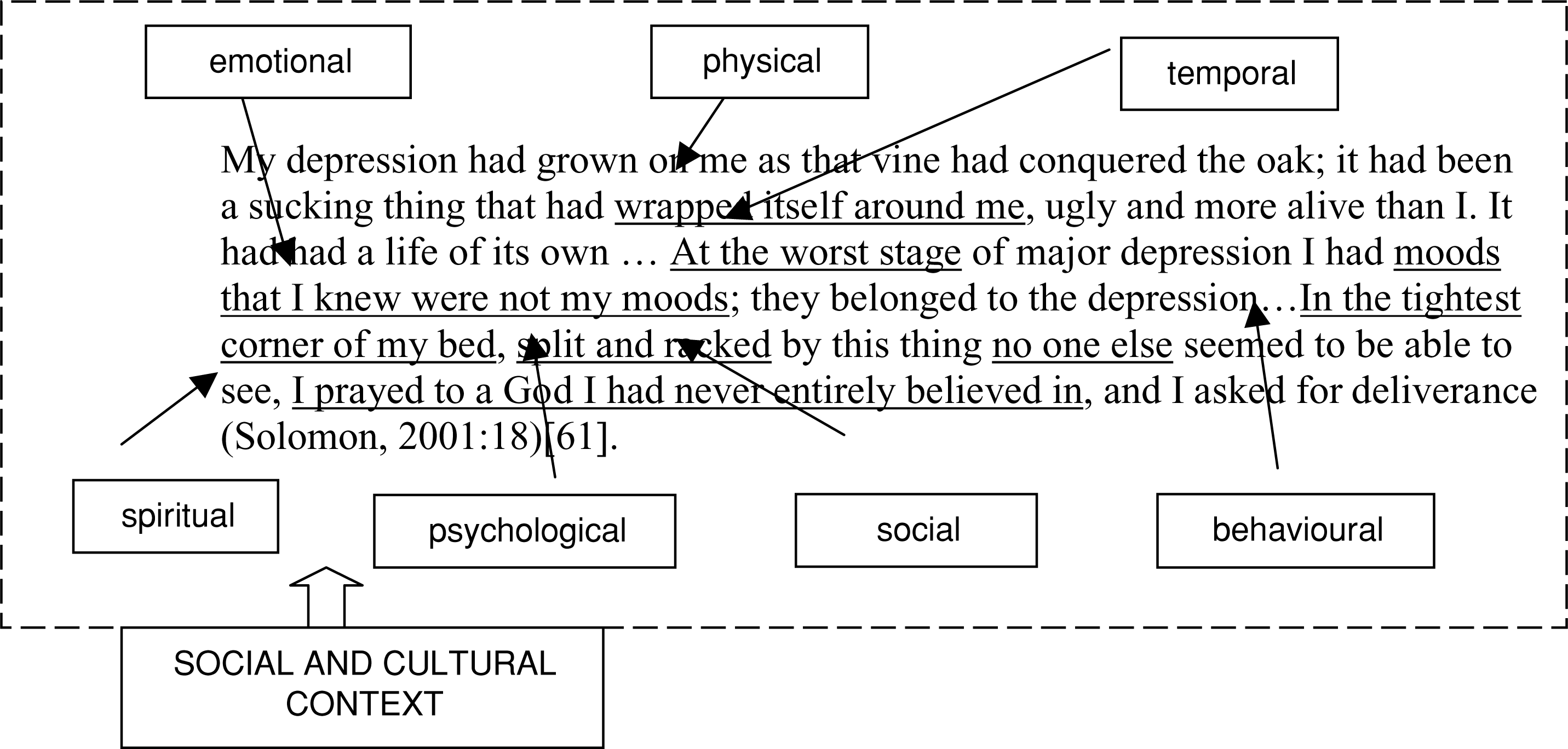
Solomon acknowledges a spiritual dimension to his depression. Other references include a sense of hopelessness and being disquieted in spirit, being spiritually shrivelled, spiritually bereft or spiritually empty [59], [60], or the feeling of a meaningless abyss [61]. Interestingly, neither Real [36] nor Pollack [9] deal in any depth with the spiritual dimension of depression in men yet it may be an important, but ‘silent’, aspect of men's experience of depression, difficult to articulate and difficult to measure.
Gender differences in depression
The emergence of gender differences in adolescence may reflect the tendency of men to show high-risk maladaptive behaviours [62] as a means of ameliorating depressive symptoms. This disparity in adolescence is supported by Rosenfield's view that men are more likely to decrease their reporting of depressive symptoms to avoid signalling distress [63] and showing signs of weakness and vulnerability [39], [50]. Any labels that would suggest depression as a ‘weakness’ (including care-eliciting signals) are likely to deter men from admitting to being depressed. Angst and Dobler-Mikola [11], [64] suggested that ‘differential forgetting’ to report symptoms by men may ‘perhaps’ be linked with the socially desirable male role in society that is less compatible with mood changes or even suffering depression. The findings in this study reinforce their view.
Observations of women by the men in this study and the women's personal accounts and observations of other women suggest that women seem ready or prepared to release or express emotions early by crying and seeking out others for help and to admit to depressive symptoms. This, in turn, leads to depression being observed and understood more in terms of women's experience, while men's experience may remain hidden and misunderstood. Although women can experience an intensification of negative emotion and loss of control of feelings (to the detriment of others), the societal and internal pressure to keep in emotional distress seems to be less for women, My depression had grown on me as that vine had conquered the oak; it had been a sucking thing that had wrapped itself around me, ugly and more alive than I. It had had a life of its own … At the worst stage of major depression I had moods that I knew were not my moods; they belonged to the depression…In the tightest corner of my bed, split and racked by this thing no one else seemed to be able to see, I prayed to a God I had never entirely believed in, and I asked for deliverance (Solomon, 2001:18)[61]. spiritual psychological physical emotional behavioural social temporal thus making it safe to report depression. The tendency for women to signal distress and to expose their need for help or support seems to be inversely matched by men's internalized avoidance of, or aversion to, showing signs of weakness or vulnerability. Thus, gender differences in depression appear to lie not in the ‘experience’ of depression per se (both men and women experience depression similarly), but in the ‘expression’ of depression. What men ‘do’ has (unfortunately) been associated with ‘men behaving badly’ [65] rather than associated with men being depressed.
45] have been incorporated in a screening instrument (the For Men Only Prompt List) and piloted in the context of general practice, positive results of which are reported elsewhere [66].
Common and differentiating symptoms of depression in men and women.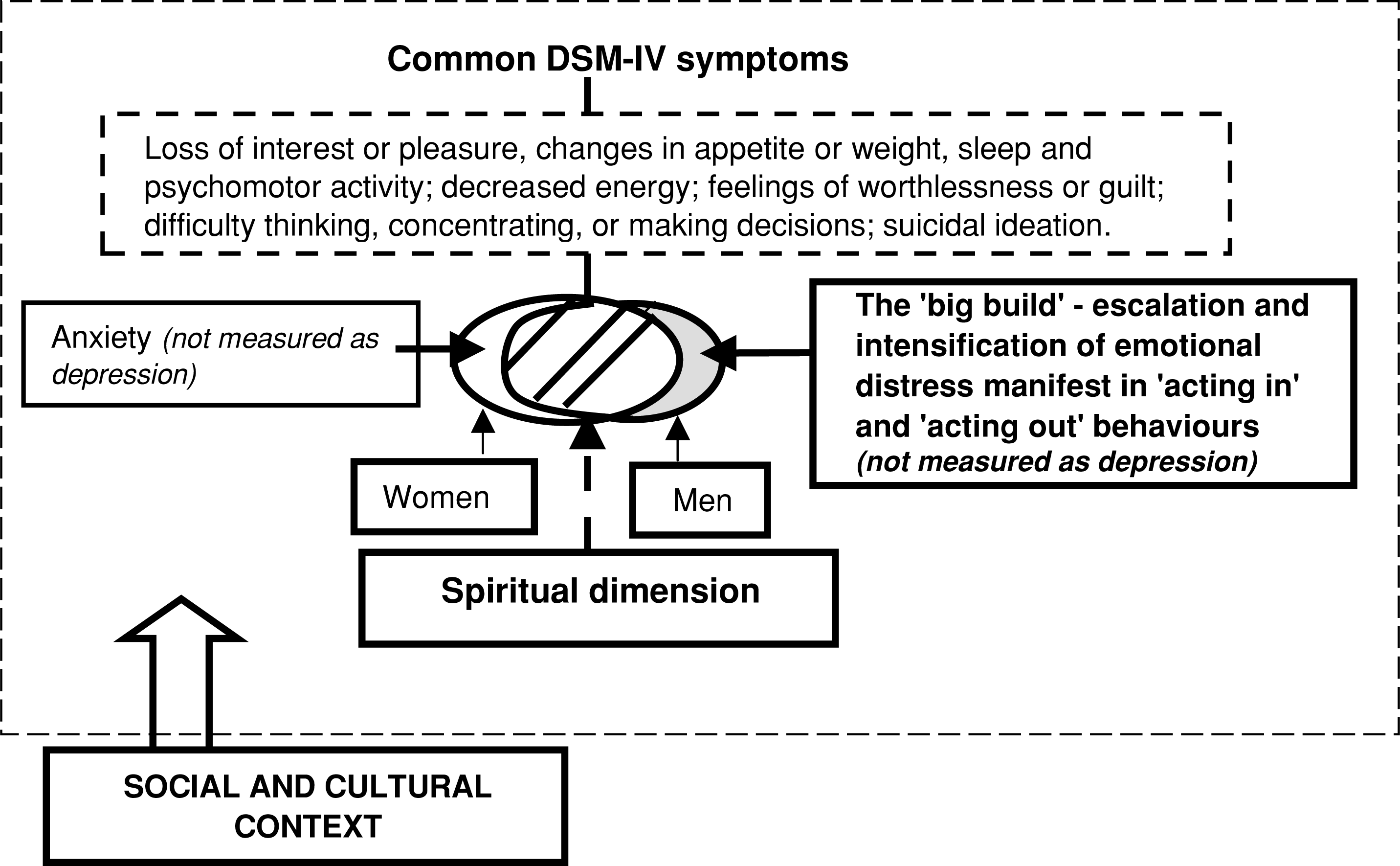
In addition, a spiritual dimension needs to be considered when eliciting depressive symptoms and exploring meanings attached to being depressed. Despite evidence to suggest a relationship between spirituality and depression (as either religious comfort or strain) [67–69], an item enquiring of a spiritual dimension of depression is missing from DSM-IV classification of depression.
Further research
One of the strengths of qualitative research is that, in addition to generating new information, findings can provide a starting point for testing out hypotheses in different settings. Three hypotheses generated from this study may be worth testing:
Hypothesis 1: That instruments that incorporate items related to withdrawal and manifest behaviours of escalation of negative affect (in addition to the commonly accepted symptoms of depression) yield higher rates of depression in men.
Hypothesis 2: That men respond to questions relating to the trajectory of emotional distress (with reference to the ‘big build’) more readily than depressive symptoms aligned with symptoms associated with women's expression of depression (viewed as a ‘weakness’).
Hypothesis 3: That men who are emotionally constrained by traditional notions of masculinity report symptoms of depression at lower rates than men who are not.
Limitations of the study
There are three major limitations of this study:
Conclusion
‘Simply asking men’ and women about their experiences of depression [35] (and their observations in others) proved to be a useful technique in examining the meaning of depression. This extended definition of depression, incorporating a constrained trajectory of emotional distress common to men, beyond that which is based solely on diagnostic categories (e.g. DSM-IV). These findings point to the need to review gender-neutral questions commonly used to elicit prevalence rates of depression in community samples and to aim for the development of gendersensitive instruments [70] that are more likely to pick up symptoms of depression in men.
Footnotes
Acknowledgements
We thank the teachers and students of the Institute of Technical and Further Education (TAFE NSW) who participated in the group discussions. We also thank Edward Lukaszewski for facilitating the groups, Adam Finch for reviewing an early draft and Glenda Lawrence for helpful comments. This study was supported by NH&MRC Grant no. 222708 and an NSW Centre for Mental Health Infrastructure grant.