
Abstract
The prevalence of depression amongwomen in the general population of Europe has been found to be twice as high as that among men [1], [2]. In a large population study [3] in six European countries, women more frequently reported depressive symptoms and reached the diagnostic threshold of depression more often than men. Similarly, marked gender differences have been found in causal attribution, in coping with depression [3] and in helpseeking behaviour [4]. In addition, as many studies have shown, depressive disorders often have poor long-term outcomes [5], [6].
Besides female gender, depression at the individual level has been associated with a low socioeconomic status [7], lack of social support [4], poor health status [8], [9], level of impairment [10], familiar risk [10] and suicidal ideation [11]. Moreover, many studies have found that negative life events can increase the risk of major depression [10], [12]. Interestingly, a community-based study by Maciejewski et al. [13] suggested thatwomen are approximately three times more likely than men to experience major depression in response to stressful life events. Life events especially associated with an increased risk of depression in women have included personal losses (the death of close friend or relative) [10] and other types of negative events such as a life-threatening illness or injury and physical attack [13].
Similarly, there is also some evidence that adverse childhood experiences (ACEs) could associate with depression in adulthood [14], [15]. According to Piccinelli and Wilkinson [4], ACEs could increase the risk of later depression by several pathways, including biological (such as long-term dysregulation of the hypothalamic– pituitary–adrenal axis), psychological (namely low selfesteem, poor coping strategies) and environmental (poor social support, low social status etc.) factors. In their review, Beatson and Taryan [15] pointed out that adverse early relational experiences could predispose a person to depression in adulthood. In addition, they noted that while secure attachment can act as a buffer in the face of stressful events in childhood, insecure attachment in close relationships could increase the risk of depression after adverse life events.
Aims of the study
Until now, there has been a relative lack of longitudinal studies simultaneously testing past and current risk factors for their ability to predict the occurrence of depression in women among the general population. Therefore, the purpose of the current 2-year follow-up study was to determine whether background factors, ACEs, social support, or stressful life events associated with recovery or non-recovery from depression and whether these factors associated with becoming depressed on follow-up.
Method
Study population
This study was a part of the ongoing Kuopio Depression Study (KUDEP) [16], [17], which has included both population and patient samples. The present study was carried out on a stratified random sample of women from a general population, all living in the district of Kuopio in eastern Finland. The sample was collected from the National Population Register. The study was approved by the Ethics Committee of Kuopio University Hospital and the University of Kuopio.
At baseline in May–June 1999, questionnaires were posted to 1502 women sampled from the general population. A total of 1011 questionnaires were returned, corresponding to a response rate of 67.3%. The follow-up data collection took place 2 years later, in May 2001. The follow-up questionnaires were sent only to thosewomen who responded at baseline. A total of 837 (82.8%) subjects responded on follow-up, but two questionnaires were rejected because of incomplete information. This left 835 women with a mean age of 46.0 years (SD=10.7, range=26–65 years), who were mostly married (70.3%) and working (67.9%).
Dropout analysis
Women who participated in both study phases were significantly older (46.0, SD, 10.6 years) than first-phase (T1) (43.4, SD, 10.7 years) and second-phase (T2) dropouts (42.5, SD, 10.9, F(2, 1501)=14.9, p<0.001). However, there was no significant difference in the mean baseline Beck Depression Inventory (BDI) score between the participants and the second-phase dropouts (5.6, SD, 6.7 points vs 6.2, SD, 7.3 points, p=NS).
Measures
Depressive symptoms were assessed using the 21-item BDI [18]. The BDI items each comprise four statements and reflect the intensity of a particular depressive symptom, with total scores ranging from 0 to 63. The BDI was used as a continuous as well as a class variable, the cut-off scores being ≥13 for depression and <13 for no depression [19]. If a BDI response was missing for one or two items, the missing item was replaced with the arithmetic mean for that subject. If more items were missing, the data set was regarded as incomplete.
At baseline, the subjects first completed a questionnaire relating to their sociodemographic background (classification in parentheses): age (mean and rated in four classes, 26–36 years vs 37–45 years vs 46–53 years vs 54–65 years); years of education (high vs low, ≥9 years vs <9 years); occupation (white-collar worker vs blue-collar worker); area of residence (urban vs rural); marital status (married or cohabiting vs single, divorced or widowed); subjective working ability (good or slightly reduced vs unable to work); employment status (employed vs unemployed); subjective financial situation (good or fairly good vs fairly poor or poor); and subjective general health status (good or fairly good vs fairly poor or poor).
The questionnaire at baseline also included a subjective assessment of the following ACEs (classification in parentheses): the relationship between the parents (good=1–2 vs poor or don't know=3–5); the happiness of the childhood home (happy vs unhappy); discipline (gentle=1–2 vs harsh=3–4); physical punishment, for example, hair pulling, spanking (no=1, yes=2–5); domestic violence with or without sexual abuse directed at the child (no=1, yes=2–4); and alcohol abuse in the primary family (no=0, yes=1) [17].
Life events over the 2-year follow-up period were charted with 12 questions [20]. The 12 stressful life events recorded were: divorce; the breaking off of a long-term relationship; the death of a spouse; the death of a close relative or friend; significantly more conflicts with the spouse than previously; a negative change in the state of health of a family member; sexual difficulties; considerable difficulties in a working relationship; considerable financial difficulties; the loss of a job/bankruptcy; illness causing work disability for over 3 weeks; and some other serious ordeal. Answers were classified as ‘yes’ (=1; i.e. ‘has happened and its meaning to me is quite significant/extremely significant’) or ‘no’ (=0; i.e. ‘has not happened/has happened and its meaning to me is minor’). Moreover, the total sum of all stressful life events was calculated for multinomial logistic regression analysis.
In addition, one question on follow-up assessed the social support received (‘Do you receive enough support and understanding for your problems from those closest to you?’ 1–2 sufficient, 3–4 insufficient). The subjects were also asked whether they had used health services (primary health care, mental health care) because of mental problems during the 12 months before follow-up.
Statistics
Statistical analyses compared the depressed female subjects (BDI score≥13) with the non-depressed women (BDI score<13) using the Pearson chi-squared test for categorical variables and the independent samples t-test and one-way anova for continuous variables.
On follow-up, subjects were divided into four groups according to their BDI scores at baseline (T1) and on follow-up (T2). Group RE (recovered, n=43) consisted of those subjects who were depressed (BDI score≥13) at T1 but not at T2, group FD (new depression cases, n=44) consisted of those who were not depressed (BDI score<13) at T1 but had become depressed at T2, group DD (non-recovered, n=73) consisted of those subjects who were depressed in both study phases and the ‘others’ (group O, n=676) were subjects who were depressed neither at T1 nor T2. Multinomial logistic regression analysis was used in order to identify the factors that were associated with each group.
All data analysis was conducted with SPSS v 11.5; all statistical tests were two-tailed and a p-value of <0.05 was considered statistically significant.
Results
At baseline, 13.9% (n=116) of the female subjects were depressed (BDI score≥13). The depressed women were significantly older, more often single/divorced/widowed andmore often blue-collar workers than the others. Depressed women assessed their health, working ability and financial situation more negatively than the non-depressed women. Depressed and non-depressed women also differed significantly in the frequency of all ACEs that were assessed (Table 1). Depressed women reported a poor relationship between the parents, parental alcohol abuse, harsh discipline, physical punishment, domestic violence and unhappiness of the childhood home significantly more frequently than nondepressed women.
Background characteristics and adverse childhood experiences (ACEs) of the depressed (BDI score≥13) and non-depressed (BDI score<13) women at baseline
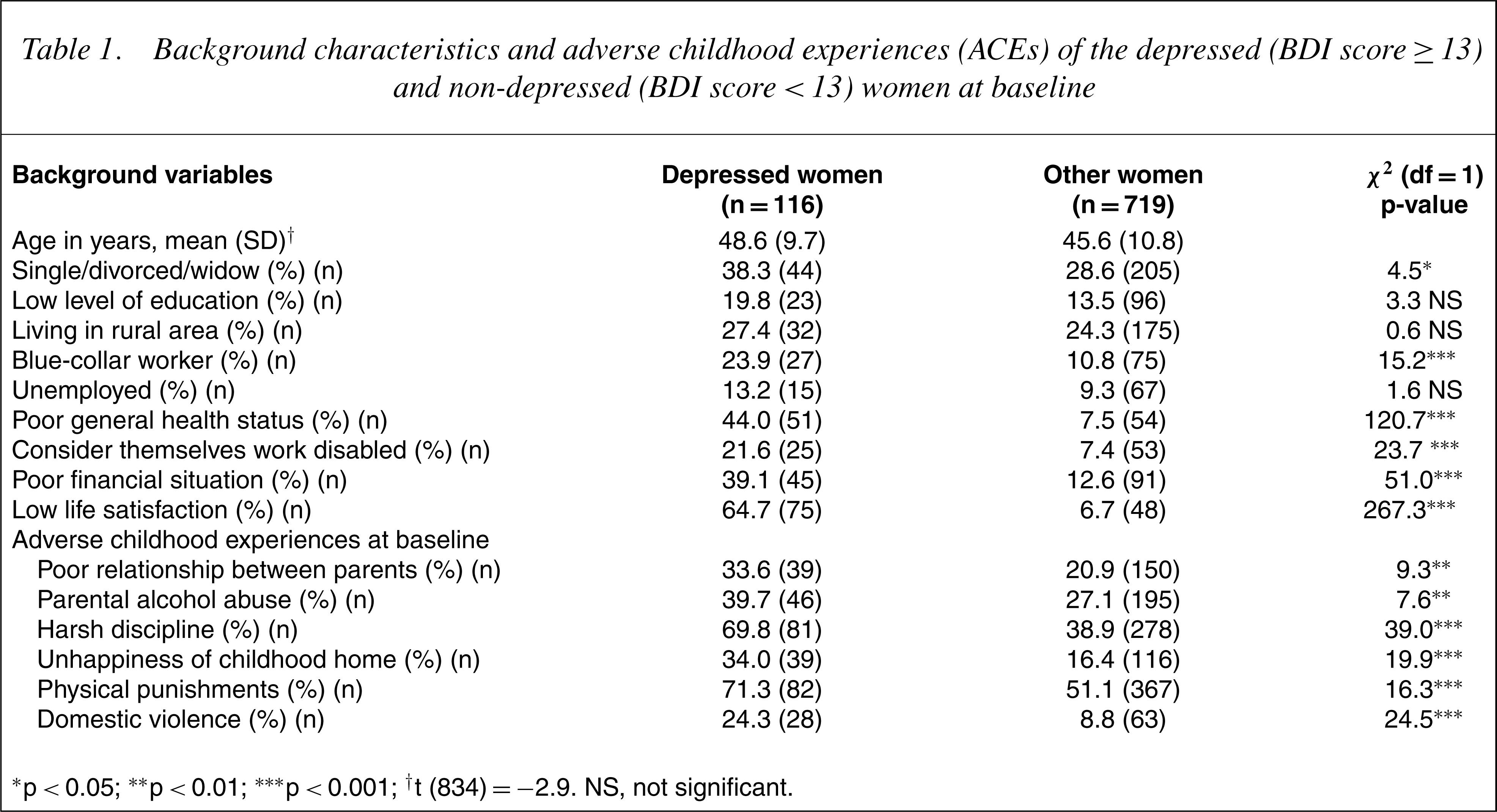
∗ p< 0.05; ∗∗ p< 0.01; ∗∗∗ p< 0.001; †t (834) =−2.9. NS, not significant.
On follow-up, the prevalence of depression was 14.0% (n=117) in the total sample and the incidence of new cases of depression during the 2-year follow-up period was 6.2% (n=44, group FD). The mean increase in BDI scores among this FD group was 11.4 (SD 6.7) points. There was also a significant difference in baseline BDI scores between the non-depressed women (group O) and women in the FD group (3.7, SD, 3.3 points vs 6.8, SD, 3.6 points, t=−6.2, df=718, p<0.001). Of the depressed women at baseline, 62.9% (n=73, group DD) remained depressed and 37.1% (n=43, group RE) had recovered from depression on follow-up. The decrease in the mean BDI score of the RE group during the 2-year follow-up was 9.7 (SD, 7.0) points. There was also a statistically significant difference in the baseline BDI score between RE and DD groups (17.7, SD, 5.1 points vs 23.2, SD, 7.8 points, t=−4.1, df=113, p<0.001).
Of all the females in this study, 55% had experienced at least one stressful life event during the follow-up. The mean sum of all stressful life events was 1.1 (SD, 1.4). The sum of stressful life events was higher among groups FD (mean 2.3, SD, 1.7) and DD (2.1, SD, 1.8) than among women in groups RE (1.6, SD, 1.9) and O (0.9, SD, 1.2, F(3, 835)=34.3, p<0.00). The death of a close relative or friend, illness causing work disability and conflicts in family and working relationships were reported more frequently by those women who became depressed during the follow-up (group FD) than among the others. Women in group DD had experienced a negative change in the state of health of a family member, sexual difficulties and considerable financial difficulties more often than the others (Table 2).
Stressful life events (%) of the studied groups during follow-up
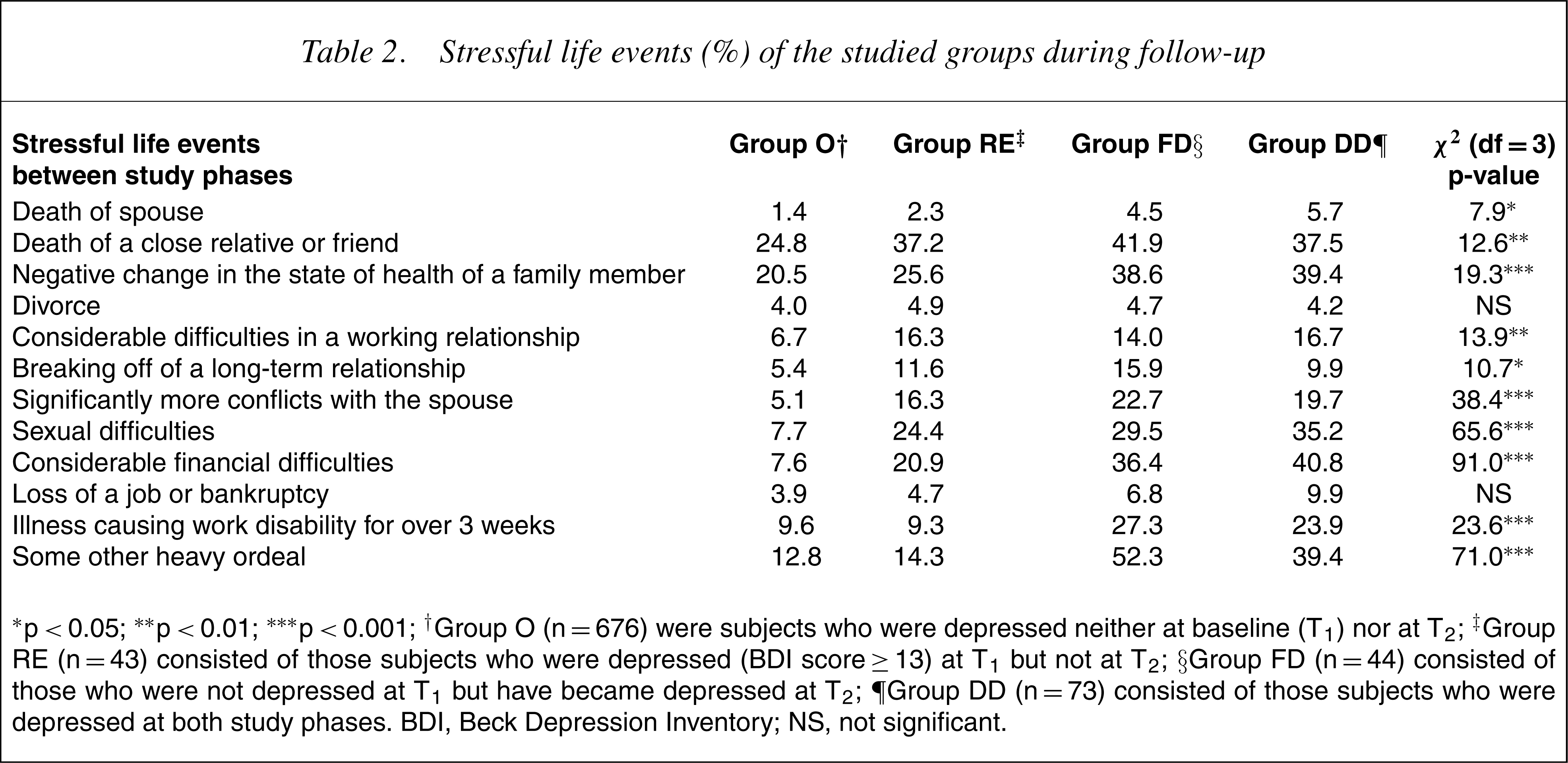
∗p<0.05; ∗∗p<0.01; ∗∗∗p<0.001; †Group O (n=676) were subjects who were depressed neither at baseline (T1) nor at T2; ‡Group RE (n=43) consisted of those subjects who were depressed (BDI score≥13) at T1 but not at T2; §Group FD (n=44) consisted of those who were not depressed at T1 but have became depressed at T2; ∥Group DD (n=73) consisted of those subjects who were depressed at both study phases. BDI, Beck Depression Inventory; NS, not significant.
On follow-up, more women in groups DD (38.4%), FD (25.6%) and RE (23.3%) felt that the social support they had received had been insufficient compared with group O (4.2%, χ 2 =118.1, df=3, p<0.001). In addition, health services were more often used in groups RE (32.6%), FD (29.5%) andDD(21.9%) than among subjects in group O (6.5%, χ 2 =61.3, df=3, p<0.001).
Multinomial logistic regression analysis was performed to simultaneously compare women in groups RE, FD and DD with those in group O in terms of their sociodemographic background, ACEs and stressful life events. The following sociodemographic factors were included in the model (Table 1): age (26–36 years=0, 37–45 years=1, 46–53 years=2, 54–65 years=3); marital status (married/cohabiting=0, single/divorced/widow=1); subjective health status (good or fairly good=0, poor or fairly poor=1); working ability (good or fairly good=0, disabled=1); and subjective financial situation (good or fairly good=0, fairly poor or poor=1). All the variables concerning ACEs (0=no, 1=yes) were also added to the model, since they were all found to significantly associate with baseline depression (Table 2). In addition, social support (0=sufficient, 1=insufficient), use of health services during the 12 months before follow-up (no=0, yes=1) and the sum of stressful life events were also included.
Compared to group O, those who had experienced a greater number of stressful life events during follow-up (OR=1.8, 95% CI=1.4–2.2, p<0.001) and had received insufficient social support (OR=4.0, 95% CI=1.6–9.9, p<0.01) had a greater likelihood of belonging to group FD. In addition, they used health services (OR=5.4, 95% CI=2.3–12.4, p<0.001) more often than women in group O.
A poor health status at baseline (OR=4.7, 95% CI=1.9–11.8, p<0.01), harsh discipline (OR=3.1, 95% CI=1.2–7.5, p<0.05), physical punishment (OR=4.6, 95% CI=1.6–13.6, p<0.01), insufficient social support on follow-up (OR=5.5, 95% CI=2.2–15.6, p<0.001) and use of health services (OR=5.5, 95% CI=2.3–13.0, p<0.001) increased the probability of belonging to group RE.
A high sum of life events (OR=1.4, 95% CI=1.2–1.7, p<0.01), being unmarried/single or a widow (OR=2.3, 95% CI=1.2–4.4, p<0.05), a subjectively poor financial situation (OR=3.1, 95% CI=1.6–6.2, p<0.01), a poor health status at baseline (OR=13.5, 95% CI=6.5–28.1, p<0.001), insufficient social support (OR=9.2, 95% CI=4.2–20.4, p<0.001) and use of health services (OR=2.4, 95% CI=1.0–5.7, p<0.05) increased the likelihood of belonging to group DD.
Discussion
The present study on women from the general populationwith and without depression at baseline compared the effect of sociodemographic variables, ACEs and stressful life events on recovery and non-recovery from depression on follow-up. The results showed that some factors from all areas were associated with depression, but differently in each group.
Interestingly, among the sociodemographic factors, a poor health status at baseline associated with both recovery and non-recovery from depression. This is thus a common experience among depressed women, but it did not alone inhibit the possibility of recovering from depression. Similar to this study, Aro et al. [8] found that in middle-aged women the perceived current physical health was a powerful predictor of depressive symptoms [21]. Another important risk factor was financial difficulties, which associated with non-recovery. Several other studies have also found an association between depression, financial difficulties [10] and low incomes [22]. It is therefore clear that financial difficulties increase the likelihood of long-term depressive symptoms among women in the general population.
The only single background factor that differentiated all depression-related groups from non-depressedwomen was the quality of social support. As we only assessed social support on follow-up, no causal effect could be established in this study. However, current depressive symptoms could negatively influence the social network and, conversely, insufficient social support may increase the likelihood of becoming depressed on follow-up. Wildes et al. [23] showed that insufficient social support was a strong prospective predictor of increased depressive symptoms in depressed women. They recommended determining the quality of a person's social support as a part of clinical assessment, which is also supported by the findings of this general population study.
As expected, the prevalence of depression was similar at baseline (14.0%) and on follow-up (13.9%), but was higher than in a study among general population adults in five European countries (women's prevalence 10.1%) [2]. However, among women in different urban areas in Europe, the prevalence of depression (assessedwith BDI-21)was quite similar to that in this study [2]. Interestingly, the incidence of new cases of depression in this 2-year follow-up study was 6.2%, which was higher than in the Netherlands Mental Health Survey and Incidence Study (NEMESIS) [24], in which the 12-month incidence of major depressive disorder (MDD) was 3.9% in women.
Similar to earlier findings [13], [25], stressful life events associated with both non-recovery from and new cases of depression on follow-up (groups FD and DD). Hammen [26] noted from a general population sample that the lives of depressed women are often chronically stressful and punctuated by more frequent negative events than those of non-depressed women; their life circumstances thus predicted an increased likelihood of further depression. In this study, stressful life events were relatively common, but conflicts in important relationships, deaths and illnesses happened more frequently to those women who became depressed during the follow-up (group FD) than among the others. These events cause high levels of life stress, which has been found to be a predictor of a depressive episode [25].
Earlier studies have shown that children who are either victims of physical violence or witness domestic violence are at greater risk of developing later psychopathology [27], [28]. Surprisingly, in this study ACEs (physical punishment and harsh discipline in childhood) associated with recovery from depression. Although childhood adversities are a risk factor for later depression [29], different coping strategies or resilience could inhibit the development of depressive disorders [30]. Interestingly, a recent study by Nemeroff et al. [31] showed psychotherapy to be a very efficient treatment, especially for those depressed patients who have a history of childhood trauma. Their results are in line with our findings, because in this study the recovered women were also receiving treatment from a doctor for their mental problems. Thus, regardless of ACEs, these women recovered from depression during follow-up.
Several limitations in the study design should be considered when interpreting these results. First, older subjects participated more frequently in both phases than younger ones, although no difference was found in their baseline BDI scores. Second, only the BDI scale and no other diagnostic instruments were used to assess depression. Finally, as the follow-up time was 2 years, it was not possible to accurately define the timewhen depressive symptoms started in thosewomen who became depressed during the follow-up. In addition, stressful life events, several background variables and ACEs were measured by single questions and there is a possibility of retrospective recall bias. However, the subjects were asked to rate the significance of each stressful life event and only significant stressful life events were coded as positive answers.
In this study, those who became depressed during the follow-up had higher BDI scores at baseline than nondepressed women. In addition, those who recovered from depression during the follow-up were less depressed (according to BDI scores) at baseline than those who were depressed in both phases. A previous history of depression or depressive symptoms has earlier been noted to be a predictor for later depression [32], [33]. In a community study, more than 50% of first-onset major depression cases were associated with prior depressive symptoms [32]. Similarly, in this study minor depressive symptoms at baseline affected the occurrence of depression on follow-up.
In summary, our results suggest that among the general population, women's current depression especially associates with stressful life events, insufficient social support, poor subjective health and financial difficulties. Those who recovered reported more ACEs but were also being treated by a doctor for their depression. It seems possible that past adverse experiences predispose women to depression, but current stressful life events actualize the depressive symptoms. In addition, treatment could be useful in those depressed women who have a history of childhood trauma.