
Abstract
Keywords
Patients with borderline personality disorder account for up to 20% of admissions to inpatient psychiatric units [1]. Up to two-thirds of this group of patients have comorbidities [2], [3]. Although inpatient treatment is an important component of the management of patients with borderline personality disorder, it can be counter-therapeutic if not delivered properly [4], [5]. Published work on inpatient management of borderline personality disorder is limited and is mainly confined to anecdotal reports or small studies. They focus on the use of treatment contracts [6], proactive intervention [7], risk assessment [8], [9], hierarchical strategies [10] and emphasize the benefits of using a time-limited approach [11–13] and special nursing skills [14], [15].
Southern Health in Victoria, Australia, has three inpatient units on two separate campuses (Monash Medical Centre and Dandenong Hospital), with a total of 75 beds, serving a catchment area with an adult population of 600 000. All patients with borderline personality disorder admitted to inpatient services are assessed and treated with a standard management protocol that has a crisis intervention orientation, offering time-limited inpatient and least-restrictive treatment. The focus is client-centred, community-oriented, forward-looking, problem-focused and skill-based. On discharge from the inpatient unit, those patients treated with a standard management protocol are referred to a general practitioner, a counsellor, a psychologist or a psychiatrist without case management. The protocol works on the rationale that these clinicians in the community will provide regular ongoing support while the area mental health service will deliver clinical intervention in time of crisis either through contacts with the crisis assessment and treatment team (CATT) or time-limited (usually 24–48 h) inpatient admission.
A number of patients receive an additional special treatment contract as part of their treatment when the clinicians are of the opinion that there are ongoing psychiatric and psychosocial issues that put them at risk of presenting again for hospital admission. For those treated with a special treatment contract, the follow-up involves a case manager based at the area community mental health clinic or mobile support and treatment team (MSTT), who liaises with a psychiatrist (public or private), a general practitioner (for general medical issues) and other relevant carers and clinicians (for special issues such as alcohol and substance misuse, gambling problem, sexual abuse, domestic violence, itinerant lifestyle). The special treatment contract is informed by the published works [6], [11], [16], [17]. It includes both inpatient and outpatient treatments and is tailored to the individual, based on a thorough assessment of the individual's current and chronic level of risk and the goals of the contract. The contract has three sections [17]. The first section is administration issues and is kept on file and available to clinical staff involved in the care of the patient. The second section is the crisis plan–clinician-focused which is made available to the patient and clinicians involved in the care. This section is to guide clinicians on the management plan for their client. The third section is the crisis plan–client-focused which is made available to both the patient and the clinicians in their care. This section is to guide the patient on strategies which they find helpful when in crisis and is to be used with the clinician-focused plan to guide the management. Miller [6], [16] has emphasized the importance of principles such as collaboration with the client, positive reinforcement, maximizing responsibility and the provision of achievable goals within the contract, as well as the tools to achieve these goals. At Southern Health the special treatment contract is based on these principles and is also seen as a ‘work in progress’ that can be modified throughout the admission and community contacts in a collaborative manner to meet the individual's needs. The special treatment contract allows close liaison between the area mental health service and community clinicians to arrange elective time-limited hospital admission. This proactive use of inpatient service aims to prevent unplanned and prolonged hospital stay which is potentially countertherapeutic.
The aim of this study is to review how the standard management protocol and the special management contract relate to hospital admission.
Method
A retrospective review was carried out using Client Management Interface (CMI) data on patients admitted during a 2-year period between 1 July 2000 and 30 June 2002. All patients who received a diagnosis of borderline personality disorder were identified. The diagnosis was made clinically. Variables collected included basic demographic data, diagnosis (ICD), comorbidities or other concurrent diagnoses (ICD), number of admissions, length of stay and the presence of a special treatment contract. The patients who received a special treatment contract as part of their inpatient management for borderline personality disorder and those who did not were compared with respect to these variables. The statistical software SPSS was used to compute t-test and anova for continuous variables. This project was approved by the Human Research Ethics Committee of Southern Health.
Results
There were 80 patients identified with the diagnosis of borderline personality disorder. The mean age was 30.9 years (range=18–57 years, SD=9.5 years). The majority were female (77.5%). More than half were single (56.8%) with the other half being either married (27%), divorced (9.5%) or separated (6.8%).
Nearly half the patients (n=39) had only one admission (48.1%), 16 (20%) had two admissions, 10 had three admissions (12.5%), five had four admissions (6.2%) and 10 had five or more admissions (12.5%).
The majority of these patients (81.2%) were treated with the standard management protocol. The rest (18.8%) received a special management contract. These two groups of patients had a different distribution of the number of admissions. In the standard management protocol group, more than half of them (58.5%) had only one admission. Fourteen (21.5%) had two, seven (10.8%) had three, three (4.6%) had four, two (3.1%) had five and one (1.5%) had seven admissions. In the special management contract group, only one patient (6.7%) had one admission. The rest (93.3%) had more than one admission – two (13.3%) had two, three (20.0%) had three, two (13.3%) had four, one (6.7%) had five, one (6.7%) had six, two (13.3%) had nine, one (6.7%) had 10, one (6.7%) had 11 and one (6.7%) had 14 admissions.
The two groups were compared with respect to their total admissions, admissions with a diagnosis of borderline personality disorder, admissions without a diagnosis of borderline personality disorder and presentations to the emergency department using anova (Table 1).
The distribution of number of admissions and types of management
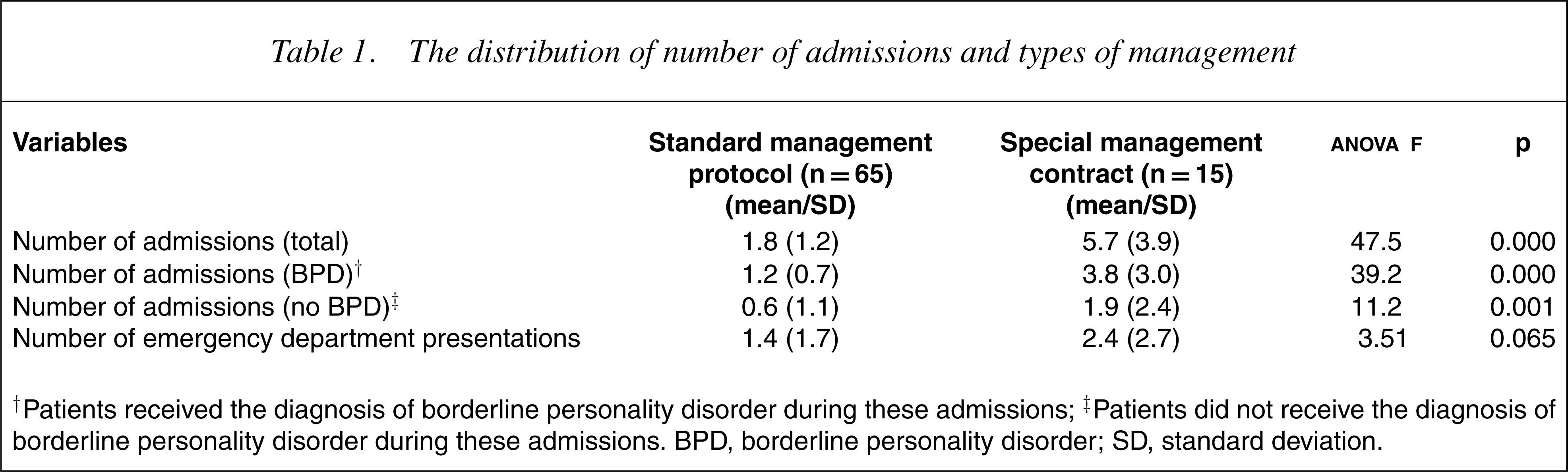
† Patients received the diagnosis of borderline personality disorder during these admissions; † Patients did not receive the diagnosis of borderline personality disorder during these admissions. BPD, borderline personality disorder; SD, standard deviation.
The special management contract group had significantly more psychiatric admissions (with or without the diagnosis of borderline personality disorder) but not more contacts with the emergency department.
The number of diagnoses other than borderline personality disorder in the special management contract group (range=0–8, mean=3.3, SD=2.3) was significantly higher (t=3.4, df=15, p=0.04) than that of the standard management protocol group (range=0–4, mean=1.2, SD=0.95).
Those who received a special treatment contract (range=1–94 days, mean=15.7 days, SD=23.6 days) had longer admissions than the standard management protocol group (range=1–43 days, mean=11.1 days, SD=13.95 days) but the difference was not significant (t=0.72, df=16, p=0.48).
The length of stay and concurrent diagnoses of the 15 patients who received a special treatment contract are listed in Table 2. The most common concurrent diagnosis (in eight patients) was depression (two with psychotic symptoms) and related mood disorders (dysthymia). Seven patients received a concurrent diagnosis of psychosis (schizophrenia, schizoaffective disorder, bipolar-affective disorder, non-organic psychosis), three had obsessive–compulsive disorder, three had adjustment disorder, two had anxiety disorder, two had acute stress reaction and two had alcohol misuse. Eating disorders were diagnosed in one patient. In 12 of the 15 patients, the diagnoses received unspecified subtyping.
Clinical profiles of the special treatment contract group
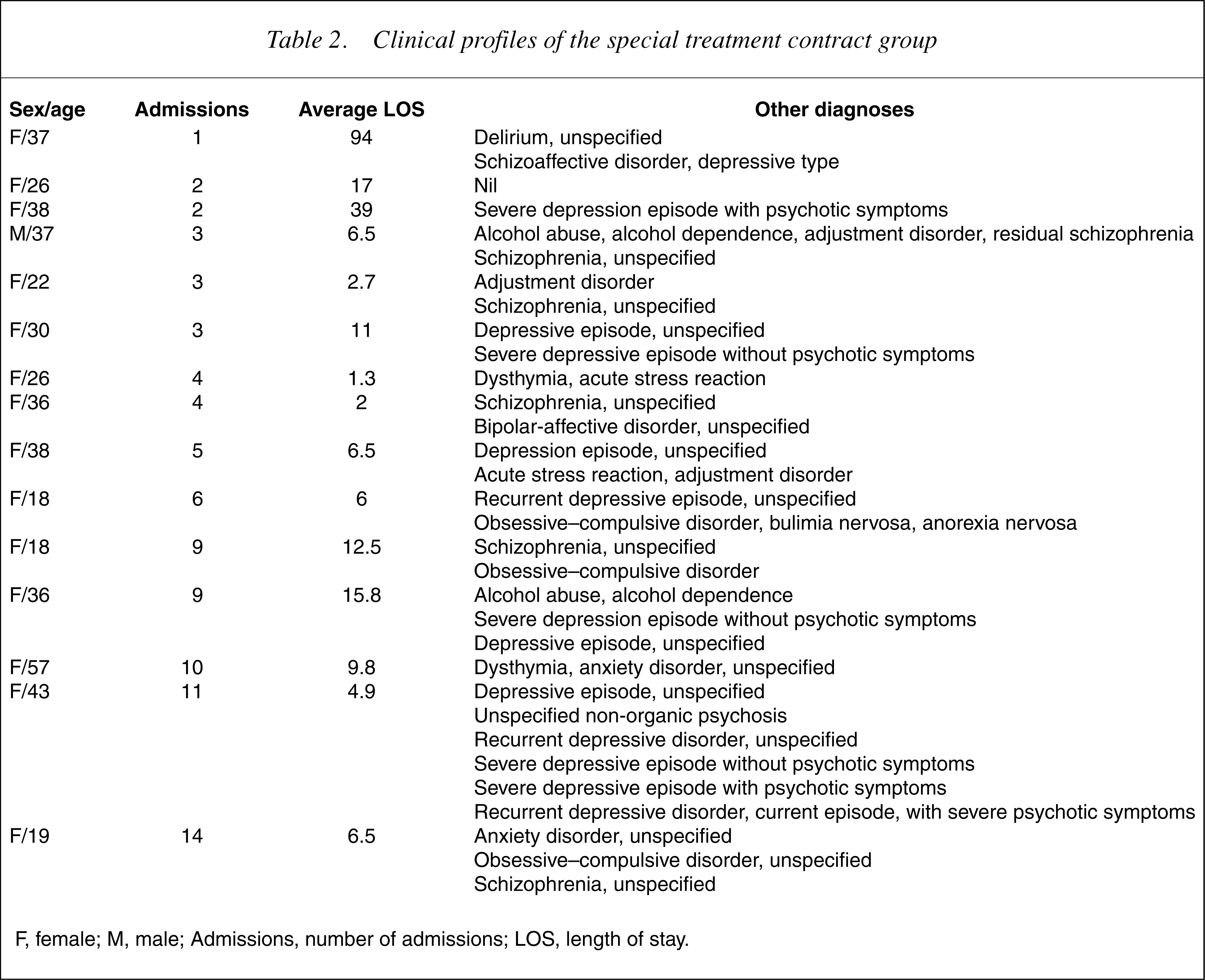
F, female; M, male; Admissions, number of admissions; LOS, length of stay.
Discussion
Our sample has a gender distribution comparable to that reported in the published works. It represents a patient population with borderline personality disorder managed at an inpatient psychiatric service at a metropolitan teaching general hospital network. The management plan is similar to those who require extra support reported in the published works. It is time-limited and crisis-intervention in nature and focuses on linking patients to ongoing community support in general and developing a special management contract for those who require extra support because of psychiatric comorbidities and challenging psychosocial circumstances.
This review emphasizes the limitation of a retrospective study, which looks at variables such as diagnosis and interventions in a naturalistic way rather than with the help of diagnostic schedules and randomized controlled trials. However, in this population of borderline personality disorder, which is difficult to engage in research, such retrospective data has the merit of drawing our attention to clinically interesting observations such as the correlation between the type of interventions and clinical profiles (the number of admissions, the consistency of receiving the diagnosis of borderline personality disorder and the number of comorbidities or concurrent diagnoses) as emphasized in this study. Because of the nature of the design of this study, it is not possible to interpret if these correlations bear a causal relationship. Indeed, further prospective studies are required to clarify how standard management protocols and special treatment contracts, as described in this study, impact on the mental health of this group of patients, including additional benefits, if any, of the special treatment contract.
The study is also limited by its arbitrary choice of duration for study, which has the potential to bias the record of the presence or absence of psychiatric morbidity and the rate of readmission. Also, the nature of the data collected does not allow us to ascertain if the patients in this sample moved out of the catchment area during the specified period or had admissions elsewhere.
Bearing these limitations in mind, it is interesting to note that the study shows that nearly 60% of patients with borderline personality disorder who received the standard management protocol did not have a readmission during the study period. For the 40% who had more than one admission, half of them got readmitted once and one-quarter of them were readmitted twice. It suggests that most patients with borderline personality disorder treated with a standard management protocol were associated with a low readmission rate. Although this result may suggest that the majority of patients with borderline personality disorder responded well to the standard management protocol, it is equally plausible that these patients had a lower readmission rate because they had a less severe form of the disorder. The lower readmission rate may also be because of the effectiveness of the protocol in keeping patients from admission without necessarily implying therapeutic efficacy. The lack of symptoms, behavioural and functional ratings in this study does not allow us to test these hypotheses.
However, only one patient (6.7%) receiving the special management contract did not get readmitted again. This may be because this group has a more severe form of the disorder. The additional diagnoses of psychosis listed in 3]. The use of this marker may lead to earlier and more accurate diagnosis of and more effective treatment planning for borderline personality disorder, although one can argue that the diagnosis of borderline personality disorder is only appropriate, if not only possible, after a longitudinal pattern becomes evident and not simply based on a particular cross-sectional clinical profile.
It is interesting to note that the special treatment contract group had significantly more admissions, but not more contacts with the emergency department. This paradoxical observation can be explained by the fact that the treatment contract allows elective and precrisis hospital admissions which may have reduced contacts with the emergency department. As case management is an integral element in the special treatment contract, this may suggest the effectiveness of case management in limiting crisis presentation to the emergency department. Controlled trials are required to test this hypothesis.
This retrospective review of naturalistic data suggests that managing patients with borderline personality disorder with the standard management protocol practised in Southern Health is associated with low readmission rate in most of the patients. However, there is a small group of patients who had comorbidities and multiple readmissions. Managing them with the special treatment contract is associated with no increase in crisis presentation to the emergency department.
A prospective study with multiple therapeutic arms and symptoms and behavioural ratings is required to elucidate how the standard management protocol and special treatment plan interact with the severity of the borderline personality disorder, the delay or uncertainty in the diagnosis of the disorder and the presence of comorbidities and psychosocial issues and how they impact on presentations to the emergency department, hospital admissions and readmissions and actual clinical improvement.
Footnotes
Acknowledgements
The authors thank the reviewers for their helpful comments.