
Abstract
The relationship between obstetric complications (OCs), such as birth and pregnancy complications and the later development of schizophrenia was first reported in 1934 [1]. The neurodevelopmental hypothesis asserts that schizophrenia results from an early (pre- or perinatal) static brain lesion with a long latency before the appearance of clinical signs and symptoms [2]. Obstetric complications represent one potential contribution to this early neurodevelopmental vulnerability.
Various studies have shown that there is an association between some specific OCs and schizophrenia, but the strength of this association is modest [3]. There are several possible reasons for this [2]. First, the effect size of the relationship is small, usually less than 2.0. Second, the definition of OCs varies across studies. Finally, the measurement of OCs is frequently retrospective with various methods of assessment ranging from parental interview to review of hospital records with potential bias resulting [4].
One strategy that has been used to elucidate the contribution of OCs as a risk for schizophrenia is the ‘nested’ approach. This is based on the idea that several types of OCs can result in a specific type of neuronal damage and constitute a single pathway of risk. For example, neonatal intrapartum asphyxia can result from maternal hypoxaemia, maternal severe stress, cord prolapse and cord engagement [5]. The common result of these different complications is ischaemic damage in the neonatal brain, especially ischaemia-sensitive regions like the hippocampus [6], which is also affected in several forms of mental illness[7–11]. Thus it makes sense to organize these complications into a single risk factor associated with ischemia, within the overall rubric of OCs. Epidemiological studies have been important in clarifying the link between particular groups of OCs and schizophrenia in recent years [12–16].
There are two kinds of hypoxia-related OCs. One is acute hypoxia, resulting from neonatal asphyxia. The other is chronic hypoxia because of intrauterine growth restriction (IUGR), which is reflected in a range of measurable indicators such as small head circumference, low birthweight and delayed weight gain after birth [17]. Indicators of both acute and chronic hypoxia have been linkedto later schizophrenia [2], [3],[18–20].
Previous studies of OCs have focused on established schizophrenia. Although the association is modest, OCs are one of the few known risk indicators for schizophrenia. To date, no studies have examined the potential contribution of OCs in accurately predicting the transition to first-episode psychosis from the ‘ultra’ high risk (UHR) mental state [21]. Our group has developed clinical criteria that have relatively good predictive power for transition, however, a significant level of false positives remains [22], [23]. A focus on OCs represents an opportunity to sharpen our predictive capacity in linking distal and proximal predictors. This is essential to improve the capacity to accurately identify individuals who are at a heightened risk of developing psychosis, and possibly to assist in the development of preventive interventions.
Method
Setting
The Personal Assessment and Crisis Evaluation (PACE) Clinic is a specialist clinical research program for adolescents and young adults at UHR of developing a psychotic disorder, taking referrals from the health, education and welfare services within the Melbourne metropolitan area [24]. This study is a component of a large program of research addressing issues of identifying young people at high risk of psychosis, characterizing the transition from high risk to acute psychosis and developing appropriate preventive interventions for this population [21], [24]. The local research and ethics committees have approved the design and aims of this study.
Participants
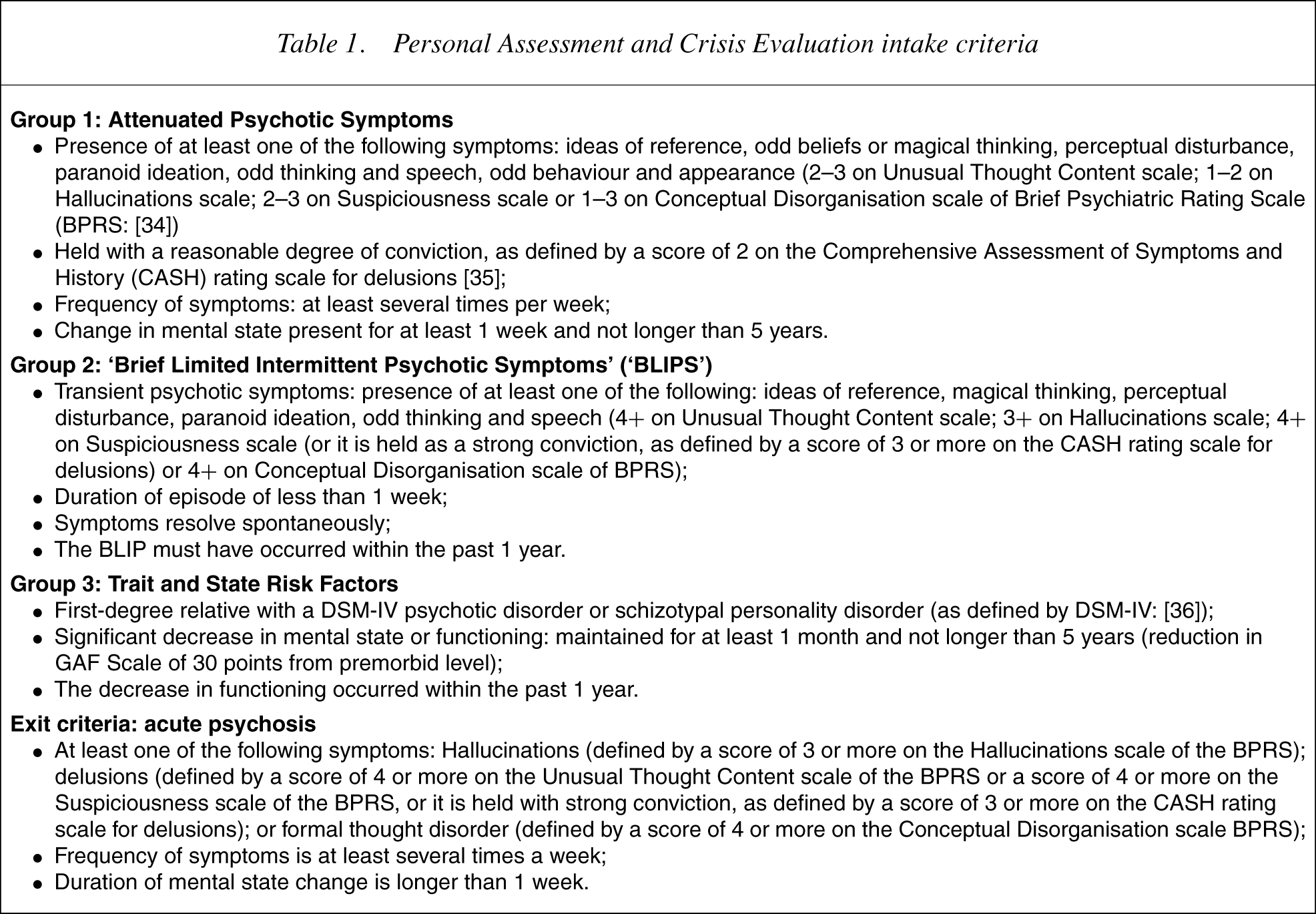
The participants in this study were recruited from patients attending the PACE Clinic. Young people are thought to be at a heightened risk of developing a psychotic disorder within a relatively short follow-up period if they meet one or more of the following criteria: (i) Attenuated Psychotic Symptoms Group: have experienced subthreshold, attenuated forms of positive psychotic symptoms during the past year; (ii) Brief Limited Intermittent Psychotic Symptoms Group:haveexperi-enced episodes of frank psychotic symptoms that have not lasted longer than 1 week and have spontaneously abated; or (iii) Trait and State Risk Factor Group: have a first-degree relative with a psychotic disorder or the identified patient has a schizotypal personality disorder and they have experienced a significant decrease in functioning during the previous year. Operationalized criteria are listed in 22], [23], [25], [26].
Personal Assessment and Crisis Evaluation intake criteria
Measures
Obstetric complication data were collected via the Lewis–Murray Obstetric Complication Scale [18] with seven additional items: season of birth (winter or non-winter); place of birth (rural or urban); maternal age; number of previous pregnancies; parity; illnesses during the pregnancy; and medication use during pregnancy. Some items were recorded numerically such as maternal age, duration of birth and birthweight. Others such as birthweight and gestation length were recorded as normal or abnormal. The questionnaire was completed by mothers of the UHR group. In most cases the questionnaire was administered verbally to mothers who often consulted their own personal records to respond to the questions. In a few cases the questionnaire was sent to the mother for completion and then returned to the investigator. Hospital records could not be reviewed if the questionnaire was in the mothers' possession.
Data analysis
Chi-square analysis was used to examine the relationship between group membership and categorical variables. Fisher's exact test was used in circumstances where the expected frequencies were less than 5. To determine whether there were significant differences between subsequently psychotic and non-psychotic cases on continuous variables, the Mann–Whitney U-test was used because data was not normally distributed. Survival analysis using the Cox regression model was also used to study the relationship between OC data and transition to psychosis survival analysis. All statistical analyses were performed using Statistical Package for Social Sciences (SPSS)v 10.0.05. Results were considered statistically significant when the corresponding p-value was 0.05 or less by two-tailed analysis.
Results
‘Ultra’ high risk sample
Seventy-four PACE UHR subjects were recruited. Over half of the young people were female (53%) and the mean age was 18.85 years (SD = 3.62). Over one-third of the UHR cohort developed psychosis within the 12-month follow-up period (n = 28; 38%, UHR-P group), whereas 46 (62%) did not (UHR-NP group). Descriptive characteristics are presented in Table 2. There were no differences between the UHR-P and UHR-NP groups in age, sex or proportion with a first-degree relative with a psychotic disorder. The UHR-NP group had a significantly higher GAF score at intake than the UHR-P group. No other differences were found between the groups in the level of psychopathology at intake.
Baseline characteristicsof ‘ultra’ high risk (UHR) participants and results of comparisons between UHR-P and UHR-NP groups
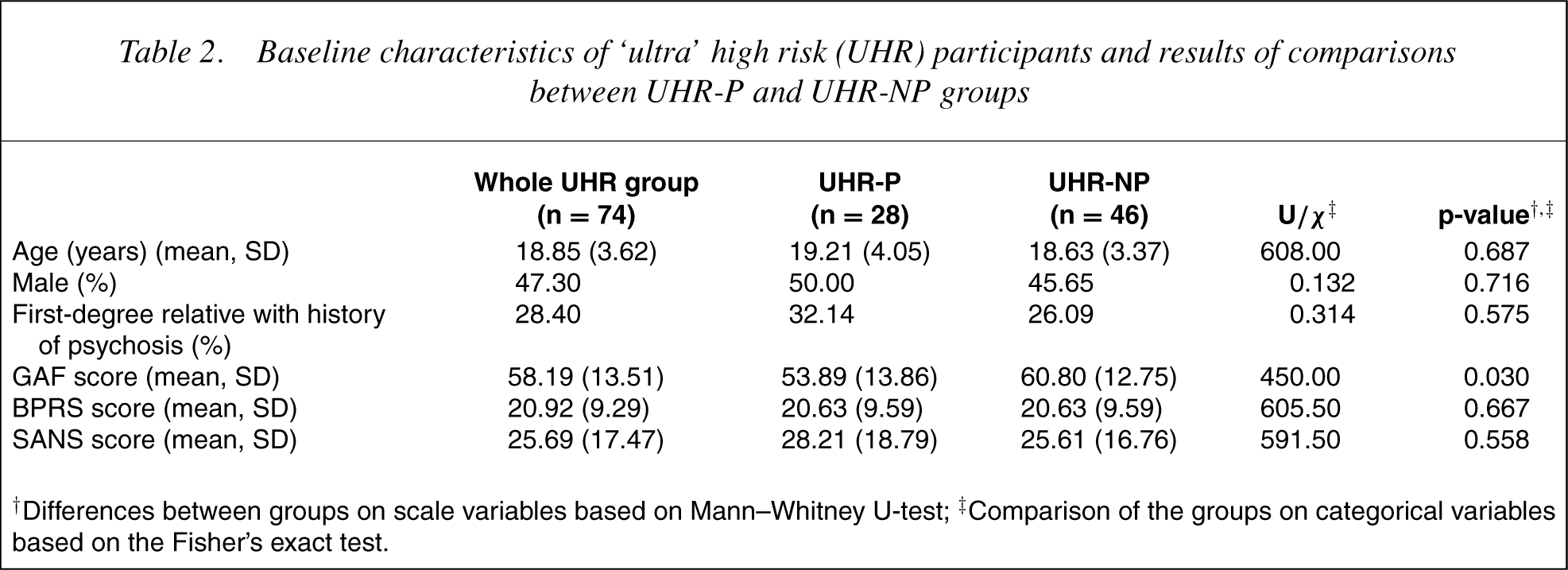
†Differences between groups on scale variables based on Mann–Whitney U-test; ‡Comparison of the groups on categorical variables based on the Fisher's exact test.
Levelof obstetric complications and subsequent clinical outcome
Very few differences were found between the UHR-NP and UHR-P groups on the experience of OCs (Table 3). The mean maternal age of the UHR-P group was slightly older than the UHR-NP group but this difference was not significant. The birthweight of the UHR-P group was significantly higher than the NP group (p = 0.01).
Comparison of obstetric complications between the UHR-P and UHR-NP groups
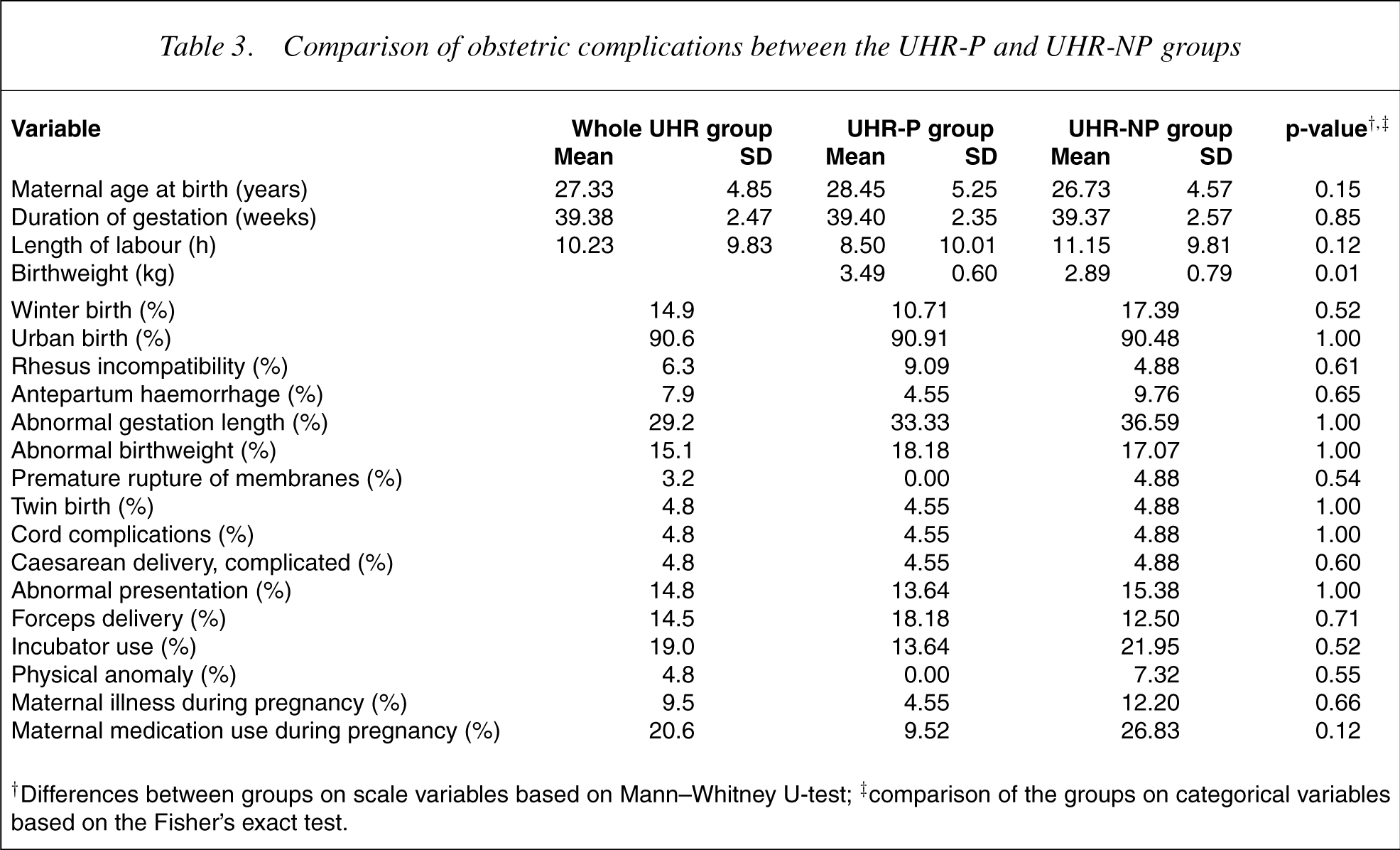
†Differences between groups on scale variables based on Mann–Whitney U-test; ‡comparison of the groups on categorical variables based on the Fisher's exact test.
The relationship between obsteric complications and transition to psychosis
The association between transition to psychosis and two groups of OCs was analyzed using survival analysis. The first analysis focused on OCs that indicated possible IUGR-preterm delivery and low birthweight. The end-point for the analysis was ‘transition to psychosis’, the number of days remaining non-psychotic was the dependent variable and the OCs were covariates. Cox regression analyses showed no significant association between transition to psychosis and the IUGR-related OCs (χ2 [df = 2] = 0.763, p= 0.683).
The second group of OCs that was analysed was acute hypoxiarelated OCs. The same end-point and dependent variable were used as the analysis described above, whereas the covariates were breech or other abnormal presentation, long duration oflabour, Caesarian delivery and incubator use after birth. Analyses again showed no significant association between transition to psychosis and these hypoxia-related OCs (χ2 [df = 4] = 1.661, p= 0.798).
Finally, no significant association was found between total OCs and transition to psychosis (χ2 [df = 1] = 0.148, p= 0.700).
Discussion
The level of OCs was not associated with the later development of psychosis in the UHR group included in this study. This finding contrasts with previous research indicating that OCs have an albeit modest association with at least subsequent schizophrenia [18],[27–29].
The birthweight of the UHR-P group was significantly higher than the NP group. This was an intriguing finding because low birthweight has previously been shown to be positively related to later onset of schizophrenia (with an odds ratio of 2.6) [30]. One possible explanation for this finding is that the UHR-P group is not representative of the broader schizophrenia population. Although most UHR subjects who developed psychosis were eventually diagnosed with a schizophrenia spectrum disorder, the UHR-P group might have been different from the subsequent core schizophrenia group at this early stage of disorder and even from the full spectrum of first-episode psychosis patients. Of relevance is that structural brain changes at this phase of illness have been shown to differ from those found in established schizophrenia [31], [32].
An alternative explanation for the unexpected birthweight difference between the two groups is that it reflects the fact that the association between birthweight and the risk of developing psychosis in the general population is not linear, but is a reverse J-shaped curve as described in a cohort study by Gunnell et al. [33]. They also found that the relationship between birthweight and height as an adult was also important, suggesting that studies in the UHR population possibly need to take this factor into consideration.
Using Cox regression and survival analysis, we found no relationship between transition to psychosis and either total number of OCs, or any group of hypoxiarelated OCs. These findings indicate that OCs (general or hypoxia-related complications) had no detectable influence upon the risk of transition to psychosis in this UHR sample, despite the association between schizophrenia and OCs compared to normal controls seen in case– control and cohort studies. Since there was no normal control group, one explanation might be that hypoxia (chronic or acute) does cause subtle brain changes that do indeed increase the susceptibility to develop mental disorder, but this increased susceptibility is not specific to schizophrenia or even to psychosis.
This study has focused on the development of acute psychosis in the UHR group as the primary outcome of interest. There may be other outcomes of the UHR group that are related to OCs such as course of illness, response to medication, development of psychopathology other than psychosis and functional outcome. Longerterm follow-up of the UHR group that emphasizes these alternative outcomes is required.
The sample size of this study may have also made it difficult to detect a relationship between transition to psychosis and OCs. Other factors may include measurement error in retrospectively rating OCs and difficulty in focusing on the subset of OCs which most heavily influence risk [3], [16]. A related issue is the threshold at which OCs may begin to exert an influence. For example, there appear to be degrees and/or durations of hypoxia that can be tolerated by the fetus or neonate without obvious effects on mental or motor function, yet, when the duration or severity of hypoxia exceeds these thresholds, dysfunction does result and may be accompanied by severe retardation or epilepsy [28]. A similar ‘dose–response’ relationship might occur between the experience of OCs and subsequent development of psychosis. Using a summary score to provide a measure of OCs disguises the different relative risk of individual OCs and their severity to the development of psychosis. For instance, the odds ratio between congenital malformation and development of psychosis/schizophreniais 2.35, whereas the odds ratio between breech delivery and psychosis/schizophrenia is 0.87 [3]. This is suggestive of a protective effect of breech delivery. However, in the Lewis–Murray scale congenital malformation and breech delivery add the same weight to the summary score. These considerations question the validity of the global concept of OCs. We did examine individual OCs but low power then becomes a major consideration.
A further limitation of this study relates to a possible sampling bias. All the UHR subjects included in this research were patients of the PACE Clinic. Attendance at PACE for clinical assistance is voluntary and it is possible that young people who attend the service and meet UHR criteria are not fully representative of the wider ‘at-risk’ population. It has been posited that factors such as ‘helpseeking’, social support or level of insight into presenting symptoms might distinguish the PACE-UHR cohort from others with a similar clinical profile [24].
Furthermore, even individuals in the UHR-NP group are not a ‘normal’ group of young people. Theypresented to the PACEClinic with a variety of psychiatric problems. It may be that OCs are a non-specific risk factor for a range of mental disorders and syndromes.
Another complicating factor is that there may be some individualsin the UHR-NP group who would have developed a psychotic disorder had they not been receiving help at the PACE Clinic. That is, at follow-up they appear to be false positives, but in fact may have the same trait risk factors as true positives. We have coined the term ‘false false positives’ to describe this group [22]. Thus, interpretation oftrait markers is difficult in this cohort. It is also acknowledged that outcome ofthe UHR group was only assessed at 12 months after initial presentation to the service and that it is possible that some UHR individuals developed acute psychosis after this time point. However, previous research at the PACE Clinic has shown that the onset of psychosis in the UHR group is most likely during the first 12-month period following initial presentation [23]. Longer-term follow-up of the UHR group is possible to establish if more subjects developed psychosis at a later date.
Additionally, having ‘psychosis’ rather than schizophrenia as the target outcome of interest could have had an impact on the results. This was carried out because first-episode psychosis is a more proximal and treatmentsalient target and is always required for a diagnosis of schizophrenia. However, previous studies have focused on schizophrenia and it is possible that OCs play a larger role in the development of schizophrenia than other psychotic disorders. Dividing the UHR-psychotic subgroup into schizophrenia or non-schizophrenia diagnoses and comparing OCs with a first-episode psychosis sample as well as groups of other psychiatric diagnoses, might have clarified the question of specificity of the effect of OCs.
A final limitation is the reliance on maternal recall of OCs in lieu of obtaining this information from other sources such as hospital records. Effect after meaning and recall difficulties might have an impact on the reliability and validity of the OC information. Information such as birthweight and length of labour or gestation is much less subject to such recall problems.
This is the first study to examine the relationship between OCs and transition to psychosis in a UHR population. We failed to find an association that could enhance our capacity to predict transition. This indicates that measurement of OCs is unlikely to be clinically useful in this predictive task, even though weaker associations may be present, particularly for specific OCs. These associations could not be detected with this study design. Since there was no control group in the present study, itremains possible that OCs have a more general effect on the risk for psychiatric disorder. This could be useful clinically for the prediction of caseness. The finding linking birthweight with transition is intriguing and unexpected, since it was in the opposite direction to what was expected. Further research may help to clarify this result.
Footnotes
Acknowledgements
This work was a component of Yang Yun's Masters of Medicine degree in the Department of Psychiatry, University of Melbourne. Yun's study in Australia from January 2001 to April 2003 was sponsored by an Aus AID scholarship from the Australian Development Service, Australian Government.