
Abstract
Most studies of psychiatric disorder in prisoners have shown a high prevalence of psychotic illnesses, which include schizophrenia, schizophreniform psychosis, schizoaffective disorder, delusional disorder and affective psychoses.
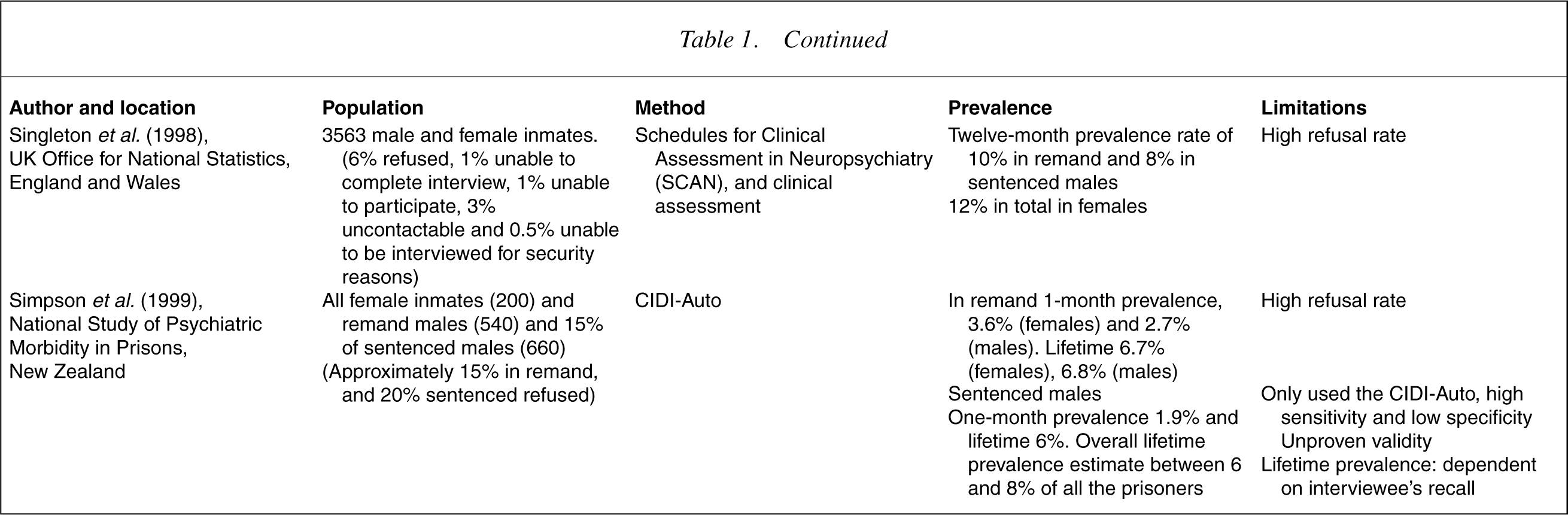
Studies by Taylor and Gunn [1], Valdiserri et al. [2], Bland et al. [3], Teplin [4], Gunn et al. [5], Herrman et al. [6], Robertson et al. [7], Birmingham et al. [8], Brooke et al. [9], Smith et al. [10], Singleton et al. [11] and Brinded et al. [12], have found a prevalence of psychotic illnesses among remand prisoners ranging between 2.7% and 10% and among sentenced inmates between 1.7% and 8% (see Table 1).
Selected studies of the prevalence of psychoses in prison populations
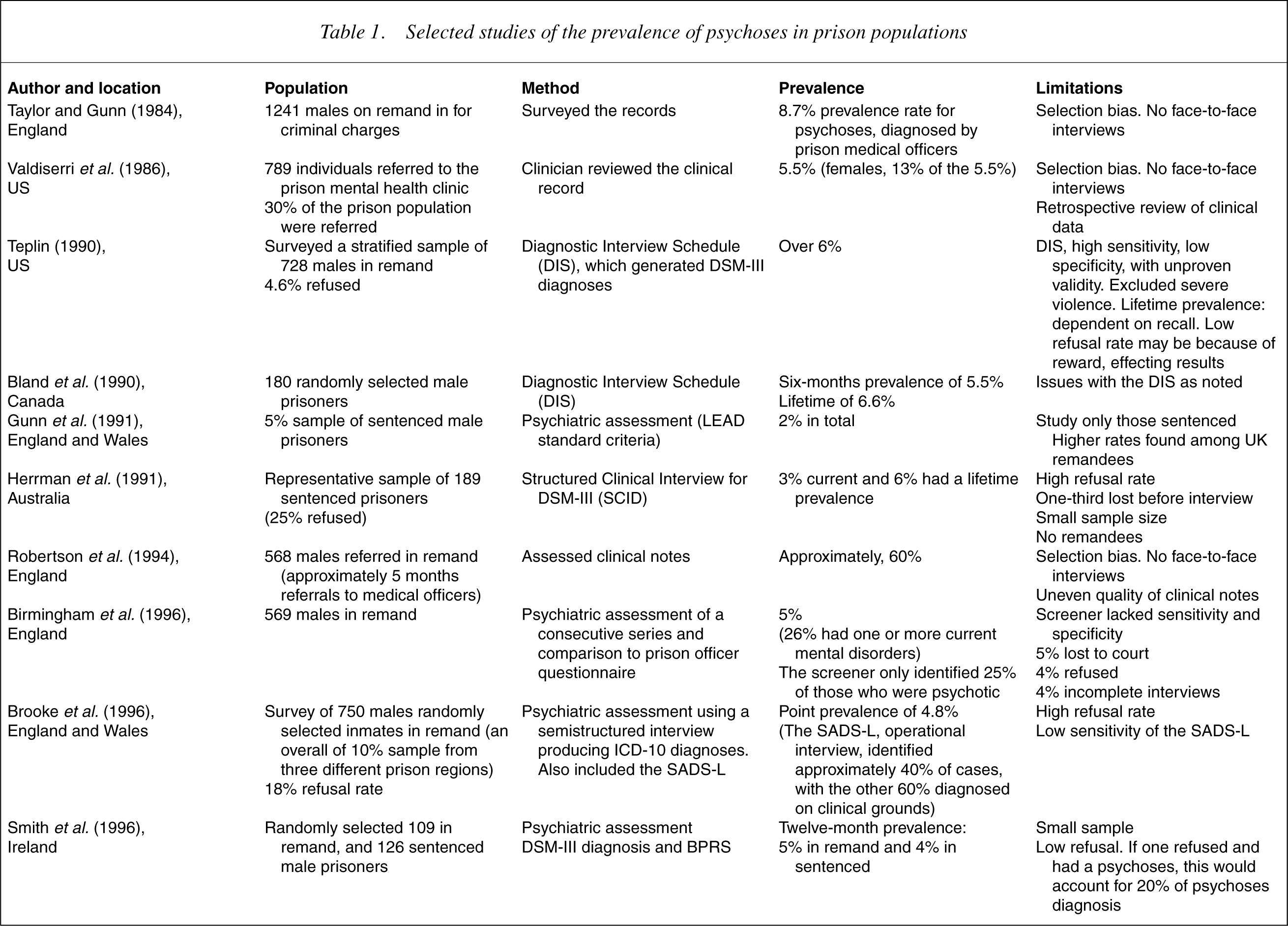
The studies summarized in Table 1 were performed in several countries, on different classes of prisoners (remanded as well as sentenced prisoners) and some included female prisoners. The methods used to estimate the prevalence of psychotic illness also varied and several studies used diagnostic instruments whose validity in prisoners had not been determined. However, all the studies indicate that the rate of psychotic illnessis significantly higher in prisons than in the wider community.
Differences in the rate of imprisonment and the ethnic make-up of prisoners would appear to limit comparisons of studies performed in the US to those of other countries. However, the prevalence of psychotic illness found in the most cited study by Teplin [4], based on diagnoses generated by the Diagnostic Interview Schedule (DIS) [13] were similar to the findings of large studies performed elsewhere.
Singleton et al. [11] found a high prevalence of psychotic illness in prisoners in England, despite a policy of diverting the seriously mentally ill from prison. They recognized the difficulty in the identification of psychotic disorders using structured instruments administered by lay interviewers and referred a random sample for assessment by psychiatrists who had been trained to use the semistructured Schedule for Clinical Assessment in Neuropsychiatry (SCAN 1.0, which incorporates the Present State Examination). They found that the structured questionnaire failed to identify significant numbers of prisoners with psychotic illness and concluded that clinician interviewers are superior to diagnostic instruments in the detectionofthe psychoses in prisoners.
Birmingham et al. [8] showed that the screening questionnaire used by hospital officers to identify mental health needs of new receptions missed 75% of those identified by the researchers to be psychotic. Brooke et al. [9] found that the screening instrument in use missed 60% of the cases.
Attempts to establish the prevalence of psychotic illness in prisoners reflect the methodological difficulties in estimating the prevalence of psychotic illness in the community at large. The Epidemiological Catchment Area Study using the DIS [13] found that about 0.7% of the adult population had schizophrenia. More recently, using a semistructured interview performed by mental health professionals, Jablensky et al. [14] found the prevalence of psychotic disorders to be 0.47%.
Some studies of the prevalence of psychotic illness in prison settings are based on diagnoses made at clinical interviews [1],[8–11]. Most ofthe large studies of prisoners have used either the psychosis module of the Composite International Diagnostic Interview (CIDI) or the DIS to diagnose psychotic illness, despite the fact that no studies that confirm the reliability and validity of these instrumentsin forensic populations. Cooper et al. [15] found the CIDI psychosis module to have low sensitivity as it found only 18% of DSM-IV and 41% of ICD-10 cases of schizophrenia diagnosed by psychiatrists.
Self-report questionnaires may also have only limited validity in surveys of prisoners. Wilson et al. [16] found that the Symptom Check List (SCL-90) incorrectly classified 15 out of a sample of 89 men, who had already been diagnosed with psychoses by the assessing psychiatrist as not psychotic. The subjects were found to have denied the presence of past or current symptoms. Spengler and Wittchen [17] concluded that although many studies found the DIS to be reliable in general populations, the diagnoses were less accurate in those with a severe mental illness, especially psychotic disorders.
Rosenman et al. [18] found that the CIDI-Auto, a computer-administered version of the CIDI [19] ‘was less likely to diagnose schizophrenic disorders than the psychiatrist’ and that ‘poor validity… may diminish the clinical acceptance of diagnosis by this instrument and of population rates of psychiatric diagnosis established by surveys which use this instrument’.
Reid et al. [20] found that prisoners could manipulate most instruments, including the DIS. They found that forensic populations are less trusting and tend to give answers that suit their own interests and are also more likely to lack insight regarding the presence of mental illness.
None of the instruments have a mechanism for assessing the subject's understanding of the questions, a problem that is likely to be greater among prisoners with lower education and belonging to non-English-speaking backgrounds [21]. Interpreting the common phenomena of psychotic illness may also be more difficult in prisoners, as for example, it is often difficult to separate plausible threats from persecutory delusions.
There have been no published studies of the prevalence of psychotic illness in New South Wales prisons, which may differ from the rates in other states of Australia and other countries for several reasons. New South Wales has a comparatively low number of acute psychiatric beds per head of population [22], which reduces the likelihood of admission to a community hospital. New South Wales is also atypical in not having a coordinated forensic mental health service and has fewer secure hospital beds per head of population than other jurisdictions [23]. Furthermore, recent changes to the New South Wales Bail Act have removed the presumption for bail for repeat offenders, which is thought to include more people with mental illnesses.
Another factor that may have affected the observed rate of psychotic illness is the particularly high level of amphetamine abuse in New South Wales. In the survey of mental health of which this study was a part, amphetamine was the most recently used drug of 31% of the subjects. Amphetamine is known to induce episodes of psychotic illness in susceptible individuals [24]. The high rate of amphetamine abuse made it more difficult to determine the nature of the psychoses and hence the number of inmates with psychotic illness requiring long-term treatment.
Hence factors that influence the prevalence of severe mental illness in prisons in different jurisdictions include the performance of mental health services in the wider community, judicial policies towards the mentally ill, the overall rate of crime, and the patterns ofsubstance abuse. Areasonably accurate estimate ofthe prevalence of psychotic illness in New South Wales prisons is essential to assist in the planning of services and in the development of policies toward mentally ill offenders.
The aim of the study was to estimate the prevalence of psychotic illness in the remand population of NSW prisons.
The study also allowed an estimate ofthe sensitivity and specificity of the screening instrument in the CIDI-Auto in a population of prisoners on reception to gaol.
Method
The study was part of a survey of the mental health of prisoners that was similar in method to the earlier National Survey of Mental Health and Wellbeing, which had excluded prisoners [26].
Prisoners received to the Metropolitan Reception and Remand Centre in Sydney and to several rural reception centres who agreed to participate in the study were administered the CIDI-Auto, which included screening questions for psychotic illness. Although the interviewers were trained to perform the CIDI-Auto without applying any clinical judgment, they were drawn from the mental health nurses and trainee psychiatrists employed by the Corrections Health Service and hence were in a position to make clinical observations of the subjects. The interviewers were asked to refer to the researchers any subjects who made positive responses to any of the screening questions for psychotic illness and also any other subjects whom they thought warranted further assessment to exclude psychotic illness based on their clinical impression.
The psychosis screener was developed for the Australian National Survey on Mental Health and Wellbeing [27] using elements of the full psychosis module of the CIDI [19] to detect the presence of characteristic psychotic symptoms.
The psychosis screener contained seven questions to elicit typical symptoms of psychosis, specifically, delusions of control, thought interference and control, delusions of reference, persecution, or of having a special power and a past diagnosis of schizophrenia. The psychosis screener was designed as part of the study of low prevalence disorders [16] to be overly sensitive in order to screen cases for further examination. However, the schizophrenia section of the CIDI was not administered to the subjects of this study because the interviews already took as long as 3 hours to perform in subjects who were already often very disturbed and difficult to interview. Instead, the subjects who were found to be positive on the screener or on clinical impression were referred for further assessment by a psychiatrist.
The clinical assessment was performed using what has been termed the LEAD criteria [28] derived from Longitudinal history, Expert Assessment and all available Data. The clinical assessment took the form of a semistructured interview looking for typical symptoms of psychotic illness, objective features suggesting the presence of mental illness and any corroborative material from the medical records and other documents supporting the diagnosis of psychosis. Subjects were interviewed by experienced psychiatrists and classified as either ‘definite’, ‘possible’, or ‘unlikely’ to have psychotic illness.
Subjects found to be mentally ill were referred for further treatment and in several cases treatment was initiated immediately.
Approval for the study was obtained from the Corrections Health Service Research and Ethics Committee.
Results
Prevalence of psychotic illness
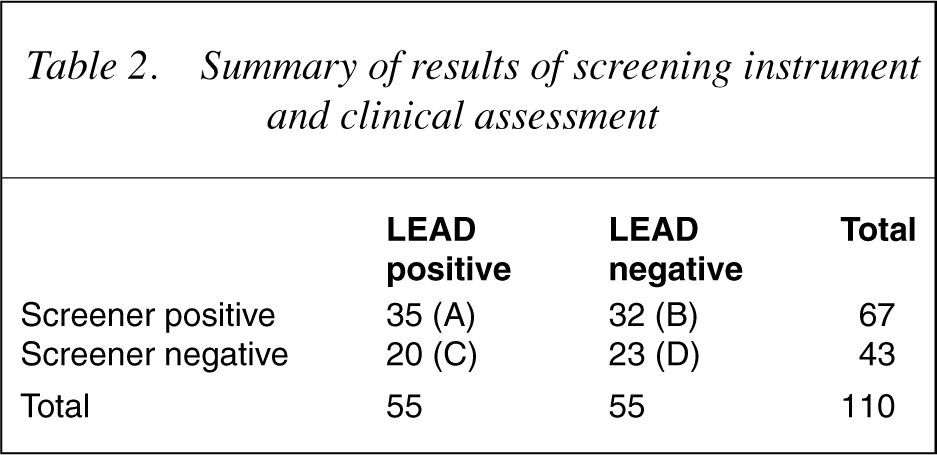
During the period of this study, 788 men received to prison were screened, of whom 60 were unable or refused to complete the CIDI-Auto. Sixty-seven subjects were positive on the CIDI-Auto psychosis screener and a further 43 were referred on the basis of the clinical impression of the interviewers (a total of 110, or 14% of the sample). Sixty subjects were unable to complete the CIDI-Auto, of whom 11 were referred for assessment on the clinical impression of the interviewers.
Thirty-two subjects who were negative on the screening instrument, were referred for further assessment by the researchers. Of these, eight were found to have ‘definite’ psychosis and five were found to have ‘possible’ psychosis (13 of 32 subjects, or 41%).
Eight subjects were referred but not assessed by a psychiatrist, either because they were released from prison (seven subjects) or were transferred to a remote prison (one subject) where no psychiatrist was available. However, review of their clinical notes showed that they had all seen other mental health professionals during the time they spent in prison and the data extracted from their medical records supported the conclusion that those subjects were unlikely to have a psychotic illness.
After a clinical interview, 42 of the 788 prisoners (5.3%) were found to have a definite psychotic illness. A further 13 subjects were considered to be ‘possible’ cases of psychotic illness, increasing the likely prevalence of psychotic illness to 6.9% (55 of 788).
Sixty men (almost 8%) were unable to complete the CIDI-Auto, of whom 11 (18% of that sample) were referred for further assessment and seven (13%) were found to have psychotic illnesses and to be in need of psychiatric care.
Performance of the screening instrument
A comparison of the results of the screening instrument and clinical assessment are summarized in Table 2. The letters in parentheses refer to the method of calculating sensitivity and specificity. The table provides an estimate of the sensitivity of the screening instrument of 63% (A/[A + C]) and an estimate of the specificity of 58% (D/[B + D]). The estimated false positive rate is 58% (B/[B + D]) and false negative rate (including non-completers) of 36% (C/[A + C]).
Selected studies of the prevalence of psychoses in prison populations
Discussion
The study showed for the first time that the prevalence of psychotic illness at the time of reception to NSW prisons is approximately 7%, a finding similar to that of studies performed in other countries using different methods. The prevalence of psychotic illness in NSW male prisoners on reception was approximately 14 times greater than the recent estimate of the prevalence of psychotic illness in the Australian community derived by clinician assessment [14].
Subjects identified as having a ‘possible’ psychotic illness were included, as they were a group with significant psychiatric disability whose service needs were similar to those of ‘definite’ cases. This approach was also taken by Brinded et al. in New Zealand [12], Singleton et al. [11] and Jablensky [14] on the grounds that further evaluation was more likely to identify at least some of the subjects as having definite mental illness and this group required psychiatric services.
The high number of men with psychotic illness remanded to prison has been attributed to disturbed behaviour when acutely mentally ill, the impairment in social function of people with severe mental illness and the effects of comorbid substance abuse [5].
The findings of this study show that NSW remand prisons contain as many as 550 men with psychotic illness, equivalent to the population of a large psychiatric hospital. Prison has been described as a countertherapeutic institution and an unsuitable place to treat the acutely mentally ill. Gunn [25] concluded that most of the prisoners found to have a psychotic illness required treatment in hospital because of the risk of violence, life threatening self-harm, victimization by other prisoners and the difficulties in providing treatment.
The importance of assessments by an experienced clinician at the time of reception to prison is supported by the finding that 20 subjects (36%) would have been missed by the screening instrument if it was used alone, resulting in delays in receiving treatment if screening was performed only by non-clinically trained staff. The clinicians performing the screening were asked to refer anyone they thought should have further assessment and not subjects they only suspected to be psychotic, which may account in part for the high number of patients referred on clinical impression who were not found to be psychotic after further interview using the LEAD criteria. Clinical assessment included establishing the presence of typical symptoms, identifying objective signs of mental illness and eliciting a history of disability and past treatment in subjects who were often extremely disturbed and guarded.
The estimates of the specificity and sensitivity of the screening instrument for psychosis contained in the CIDI-Auto were low. The full diagnostic instrument was considered unlikely to be much better for the same reasons that the screening instrument was unsuccessful in identifying cases [18], [20]. The findings of this study cast doubt on the conclusions of studies that relied solely on the CIDI screening instrument to identify cases.
The recent abuse of amphetamine and other drugs known to induce transient psychotic illnesses may explain why some subjects reported symptoms of psychotic illness at screening, but were not assessed to be psychotic at clinical assessment during the subsequent week. The initial screening may have occurred at a time when some subjects were still affected by drugs. However, subjects who reported symptoms of psychotic illness secondary to drug use and who recovered without treatmentwould have been defined as ‘unlikely’ according to the researcher's assessment criteria, unless there were other features indicating the presence of chronic illness.
A limitation ofthis study was that there was no control group referred for assessment who were negative on both the screener and clinical impression, although a finding of more cases in a control group would only have increased the final prevalence figure. Another limitation was that most of the subjects were examined by only one psychiatrist for the purposes of the study, although all the cases were discussed by the authors and the diagnostic criteria reviewed. However, the assessment often included a review of documents relating to assessments performed by other psychiatrists, both in custody and in the community.
Conclusions
The study showed a rate of psychotic illness of around 7% among remand prisoners in NSW, 14 times the rate found in a similar study of the prevalence of psychotic illness found in the wider Australian community. The study confirmed the perception that reception prisons in New South Wales carry a significant burden of the care of men with schizophrenia and other psychoses.
The inadequate performance of the psychosis-screener used in this study confirmed the need to develop of a more sensitive screening instrument to detect psychotic illness among prisoners. The finding also confirms the importance of early assessment by experienced clinicians to identify and treat prisoners with mental illness.
There are currently very few secure hospital beds available for treatment of the acutely mentally ill in New South Wales, as most of the beds are taken up by longterm forensic patients. This study confirms the need for the development of appropriate facilities for managing acutely mentally ill inmates within the prison system, as well as community-based mental health services to care for the large number of mentally ill men in prisons on their eventual release.