
Abstract
Intellectual disability is formally conceptualized in most definitions as deficits in cognitive ability, adaptive behaviours and the appearance of these problems during the developmental period [1]. People with an intellectual disability may have abnormalities of brain development and function, and associated difficulties in communication and mobility, and self-care is needed to develop socially. Adults with an intellectual disability form a very diverse group, inclusive of those with low support needs or mild disability through to people who have high and often complex support needs, for example profound disability. This population is growing in numbers and will continue to make significant demands upon human, health and disability services across Australia.
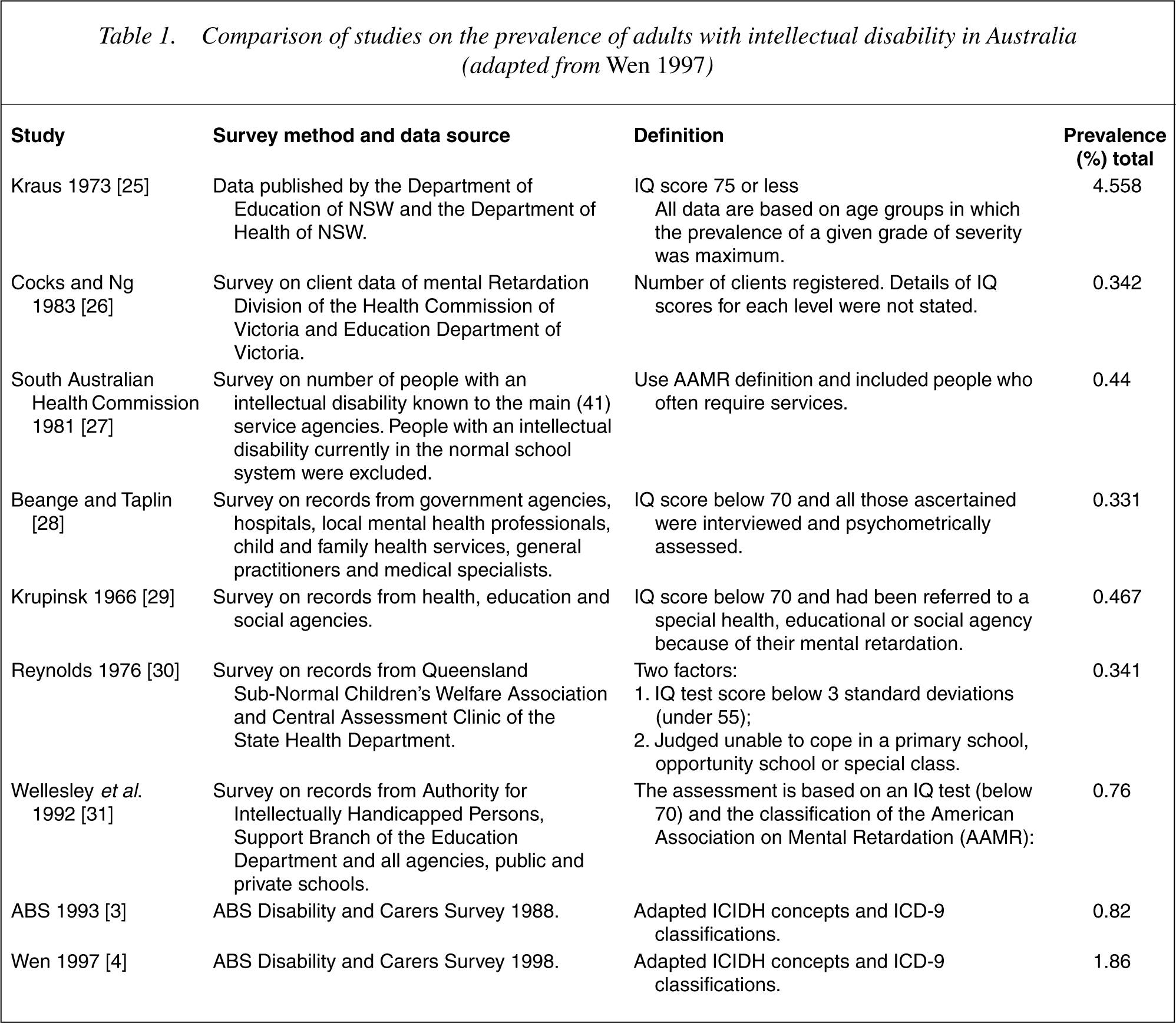
Over the past 50 years prevalence rates have differed according to the definitions of intellectual disability used in research studies [2]. Examples of these since the 1970s are described in 3]. The 328 000 people identified had an intellectual disability either as a primary disabling condition or as an associated condition. Within this group 174 000 (0.99% of the total population) need ongoing support [4]. The difference to the results reported here relate to different classification systems and analyses with the earlier database.
Comparison of studies on the prevalence of adults with intellectual disability in Australia (adapted from Wen 1997)
Dual diagnosis
Dual diagnosis is a conceptualization of comorbidity in adults with an intellectual disability. Co-morbidity refers to the presence of at least two distinct and separate disabilities or pathologies in the same individual. First utilized in the US during the 1970s, dual diagnosis was used to describe mental health problems in adults with an intellectual disability. The term dual diagnosis specifically refers to coexisting intellectual disability and mental disorder [5]. The term is also popular within the UK although ‘learning disability’ is preferred to the term, intellectual disability. Some academics and professionals around Australia appear ambivalent about the term dual diagnosis, preferring the term dual disability. This concern is that the term dual diagnosis fits poorly with the concept of social role valorization.
There are a number of key issues related to why adults with an intellectual disability are more likely to experience an episode of mental illness during their lifetime. A number of syndromes of genetic origin result in intellectual disability associated with mental disorders and brain trauma or insult can result in mental health problems. In addition, factors that increase the development of mental health problems cluster in the lives of adults with an intellectual disability, for example genetic, biochemical, early experiences, psychosocial stressors and cognitive/ behavioural problems [6].
Numerous issues exist complicating the accurate assessment of mental health in people with intellectual disability. Signs and symptoms that are suggestive of mental health problems in people with intellectual disability may not correlate well with the diagnostic criteria within the DSM-IV-TR or the ICD-10. Other factors which may compromise the value of classification criteria include:
Intellectual distortion: concrete thinking and impaired communication skills regarding the person's own experiences; Psychosocial masking: impoverished social skills and life experiences that can lead to unsophisticated presentation and therefore a ‘missed’ diagnosis or perhaps a ‘misdiagnosis’; Cognitive disintegration: stress-induced disruption of information processing presenting as bizarre behaviour and psychotic symptoms; Baseline exaggeration: pre-existing cognitive deficits and maladaptive behaviours that distort symptoms and signs, making interpretation difficult; Overshadowing: where the existence of the intellectual disability masks psychopathology; Developmentally appropriate phenomena including talking to oneself, solitary fantasy play and imaginary friends can be mistaken for psychopathology [1]. It can be a difficult task to tease out whether behaviours of concern are in response to an organic, psychiatric, environmental causation or a combination [7].
Prevalence of dual diagnosis
There is a general agreement within the literature that the lifetime prevalence of mental disorders in adults with an intellectual disability is higher than in the general population. However, there are differing opinions regarding the prevalence rate [8]. Estimates of the prevalence of dual diagnosis vary according to the age and location of the population studied; definitions of intellectual disability and mental disorders; diagnostic criteria; exclusion or inclusion of challenging behaviour; and the instruments used. Prevalence rates in some studies have varied from 14.3% through to 67.3% [9]. A review of 12 epidemiological studies found prevalence rates ranged from 14% to 80% [10]. Davis et al. [11] reviewed the literature relating to depression and found rates between 1.2% and 8.9%.
Einfeld and Tonge [12] in an ongoing Australian study of young people aged 4–18 years have shown the prevalence of clinically significant emotional and behavioural problems is approximately 40%. Rutter's classic prevalence study of psychopathology in children living on the Isle of Wight in the UK [13] found similar rates. These prevalence rates suggest that psychopathology in adults with an intellectual disability is a more serious community problem than schizophrenia, which has a lifetime prevalence of approximately 1%. If adults with an intellectual disability have increased exposure to risk and psychosocial vulnerability factors that increase susceptibility to mental health problems, it may be argued that the presence of intellectual disability can be considered to be a risk factor for the development of mental disorders [14], providing there is acknowledgement that not all people with intellectual disability develop mental health problems [15].
The aim of this study is to highlight that there are many Australians affected by intellectual disability and comorbid serious mental illnesses. It explores a common clinical picture and the reasons for which it is commonly overlooked.
Method
Data source
Data were analysed from a confidentialized unit record file (CURF) provided by the ABS. The SDAC 1998 was conducted from 16 March to 29 May 1998 [16],[17]. The household component of the survey gathered data from 37 580 people. The survey was authorized by the Australian Federal ‘Census and Statistics Act, 1905’. The ABS protected the confidentiality of individuals in the data set by removing identifiable households from the file, and where necessary, unlinking variables to suppress the detail available. Hence, data from this CURF may not exactly match that reported elsewhere by the ABS. Other than reducing the total sample size by 1.5% these confidentiality protections did not limit analyses.
Sampling
The survey design and operation are detailed elsewhere [17],[18]. The survey took place in both urban and rural areas in all states and territories, except in remote and sparsely settled parts of Australia. Statistical adjustments for not sampling remote residents were applied to the Northern Territory sample because unlike other states, a significant proportion (≈ 20%), of Northern Territory residents live in remote areas. Participants included all people except prisoners, non-Australian diplomatic personnel, and members of non-Australian defense forces stationed in Australia. The survey sample was selected using multistage sampling techniques based on census collection districts. The effective sample included 15 316 private dwellings (representing approximately one per 400 dwellings in Australia) and 399 non-private dwelling units (such as hotels, motels, boarding houses, educational and religious institutions, guest houses, construction camps, short-term caravan parks, youth camps and camping grounds, staff quarters, and self-care components of retirement villages). Non-private dwellings were selected separately from private dwellings to ensure adequate representation. Each was given a chance of selection in proportion to the average number of people accommodated.
Identifying persons with comrbid mental disorders
All health conditions of at least 6 months duration were coded according to the ICD-10. A large proportion of health conditions were coded automatically in the field. Experienced ABS household interviewers (who were not medically trained) were given three days training in the computer-assisted interview schedule and the ICD-10 classification system. The 1998 schedule was updated from a similar survey conducted in 1993.Mental health disorders were identified in three possible ways: by self-report; with a responsible adult of the household; or by another responsible adult person assisting with the interview. Multiple interviews with respect to the same person were sometimes required to complete the schedule. Intellectual disability and developmental disorders (F70–F89), autism and related disorders (F84) and developmental learning disorders (F80–83, F88, F89) were the primary ICD-10 classifications (bracketed numbers refer to ICD-10 reference codes). Secondary diagnoses clustered as schizophrenia (F20) and other psychosis (F001, F04–06, F21–29). Anxiety as the secondary condition included: phobias (agoraphobia, social phobia and specific phobia (F40); panic disorder and generalized anxiety disorder (F41); obsessive compulsive disorder (F42); acute stress disorder and post-traumatic stress disorder (F43); and other neurotic, stress related or somatoform disorders (F44-48). Depression as a secondary condition included ICD codes F32–34. Text fields were used for any disorders reported which did not appear to match items on the pick lists. Codes for all text entries were determined post-interview by more experienced ICD-10 coders. This was necessary because some anxiety disorders were collected under more general descriptive categories within the pick lists. For instance, acute stress disorder (F43.0) and post-traumatic stress disorder (F43.1) were both coded under the description ‘nervous tension/stress’. To ensure coding accuracy, all interviews were checked until each interviewer achieved 90% agreement or higher with an experienced coder. Sample monitoring of coding continued throughout data collection.
Disability, long-term health conditions, and employment restrictions
The survey used the World Health Organization's International Classification of Impairments, Disabilities and Handicaps [19], as a framework to identify disability and the associated level of restriction. Each interview commenced with a series of screening questions about activity restrictions, impairments, and long-term health conditions, before the level of disability and the underlying health condition were identified. Individuals had a disability if they had an impairment or restriction in everyday activities that was likely to last for 6 months or more. It was possible for people to have a disorder as a long-term health condition, but without activity restrictions and hence, without a disability. Disability and employment restrictions were assessed at four levels of severity (profound, severe, moderate and mild). ‘Profound’ was defined as unable to perform employment or a core activity, or always needing assistance. ‘Severe’ was defined as needing assistance to perform employment or a core activity. ‘Moderate’ referred to not needing assistance, but having difficulty. ‘Mild’ referred to having no difficulty, but using aids or equipment because of disability. Postschool educational qualifications were coded according to the ABS Classification of Qualifications. Further descriptions of terms and variables are available from the ABS [20].
Statistical analysis
The sample was restricted to people aged 15–64 years with anxiety as the primary ICD-10 condition in the household component of the survey (those with anxiety disorders aged 15–64 years living in private or-non-private dwellings, n = 716). A control group of people aged 15–64 years without activity restrictions, disability or long-term health conditions (n = 20 366) provided reference points for comparison. Population weights were provided by the ABS as an individual level variable within each respondent's record [16], allowing expansion of estimates to apply to the Australian population within the scope of the survey. SAS version 8.0 [21] was used to follow the methods recommended by the ABS [16]. The tables shown provide population prevalence estimates per 10 000 people. Standard errors (SE) of population prevalence estimates were calculated. Differences among population estimates of interest were examined using standardized two-tailed Z-scores [16] adjusted for multiple comparisons by the Bonferroni procedure to a 99% confidence level. Population prevalence estimates with standard errors less than 25% of the estimate value are considered by the ABS as sufficiently reliable for most purposes. Estimates with standard errors greater than 25% of the estimate value are marked accordingly.
Results
The life time prevalence of intellectual disability was 1.3%. Of these people 1.3% had a psychotic disorder, 8% a depressive disorder and 14% an anxiety disorder that had been present for at least 6 months and of such severity that it too was disabling (Table 2).
Prevalence per 10 000 population† of intellectual disability (ID) and comorbid mental illness
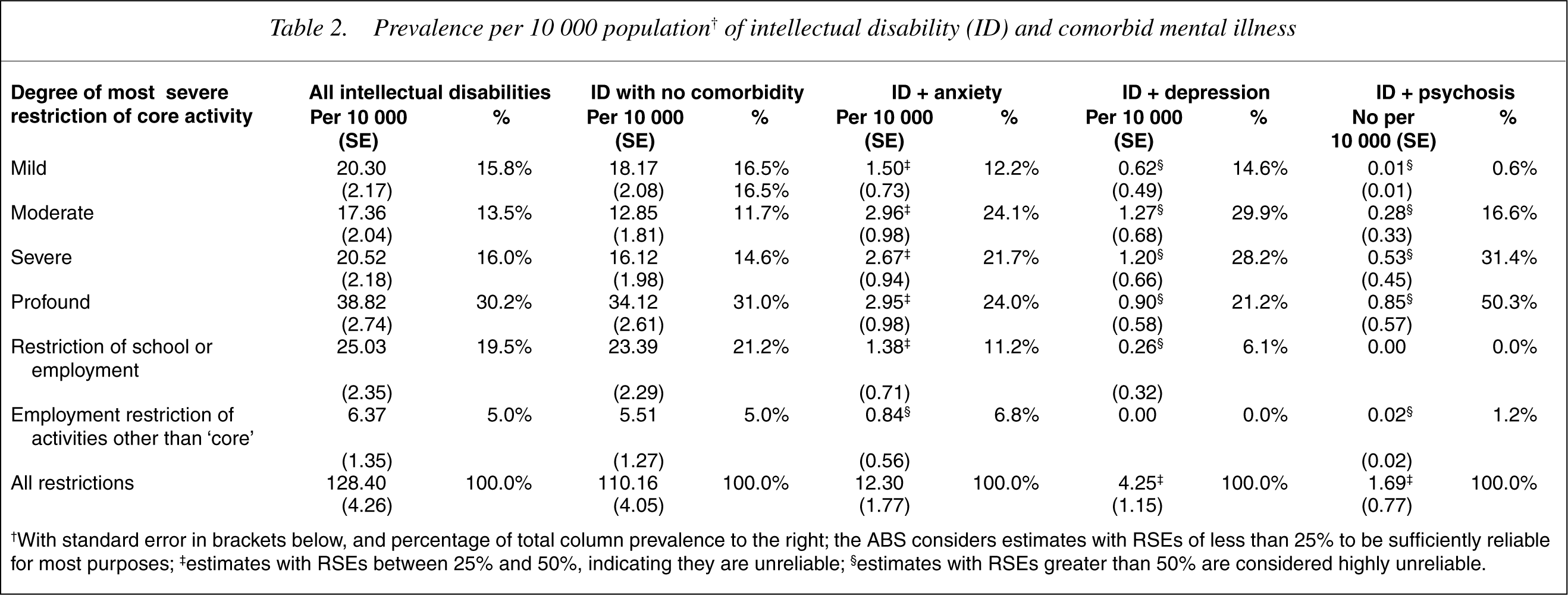
†With standard error in brackets below, and percentage of total column prevalence to the right; the ABS considers estimates with RSEs of less than 25% to be sufficiently reliable for most purposes; ‡estimates with RSEs between 25% and 50%, indicating they are unreliable; §estimates with RSEs greater than 50% are considered highly unreliable.
Patterns of disability are presented as within column percentages. Small cell sizes prevented further statistical analyses between columns. Patterns of distributions of within-column prevalence suggest high level of disability across all diagnostic categories. However, clinical or syndromic diagnoses do not appear to discriminate patterns of disability or need. Dual diagnosis or dual disability implies an additivity of disability which is not contradicted by the data presented here.
Discussion
Intellectual disability commonly affects Australians. There is a high risk to people with intellectual disability of also developing a serious mental illness Some studies have suggested that disability may be discriminated by levels of symptomatology. Lindsay and Morrison [22] found mildly disabled people who were anxious showed impaired performance for tasks, short-term memory, incidental learning and attention. Anxiety was shown to decrease the short-term memory, attention span and incidental learning of those with and without intellectual disability. Davis et al. [12] found the literature reinforced that adaptive behaviour skills were commonly affected by depressive illness. This appears to be supported by the findings reported above. Accurate assessment, diagnosis and analysis of the presenting mental disorders are fundamental prerequisites for the treatment and management of dual diagnosis. Effective treatment and support will be contingent upon appropriate diagnosis and assessment that addresses both the physical and mental health needs of adults with an intellectual disability. There can be major difficulties in establishing a diagnosis of a mental disorder in people with an intellectual disability, particularly when the capacity to participate in the clinical assessment is compromised.
Many adults with an intellectual disability can describe complicated, internal feelings but those with more severe disabilities will have difficulty describing such phenomena. When an individual is unable to verbalize or describe psychiatric symptoms, there is increased reliance upon the observations of carers and substitute decision makers. Diagnosis and assessment must therefore adopt a practical approach. The clinician must draw upon different sources of information including carer reports, direct observations of behaviour and careful consideration of history [23],[24].
More severely disabled people may respond to psychological distress by becoming aggressive to others, harming themselves, pacing and disturbed physical and verbal behaviour. Anxiety and anger are both states of increased physiological and psychological arousal, and both trigger the ‘fight or flight’ response. Anger and anxiety are particularly closely related in the intellectually disabled; in the profoundly disabled, it may be prudent to simply consider the presence or absence of a state of increased arousal.
The rigorous sampling methods of the ABS gave this study a strong data set from which to draw its conclusions. However using this methodology makes comparisons with other studies difficult, most notably because it employs self-report for diagnosis of mental disorders [19].