
Abstract
Delineation of psychiatric comorbidity in children and adolescents is essential for clinical assessment, treatment planning, monitoring of treatment response and aetiological studies [1]. The study of comorbidity in attention deficit hyperactivity disorder, combined type (ADHDCT) over the past two decades has established that disruptive behaviour disorders, oppositional defiant disorder (ODD) or conduct disorder (CD) [2–5], and internalizing disorders (anxiety and depressive disorders) [1], [4],[6–9] co-occur greater than chance.
ADHD-CT and mood disorders co-occur in 15% to 75% of cases in both epidemiological [10], [11] and clinical [12–15] samples of children and adolescents and their co-occurrence may be associated with a worse outcome [16–18]. Dysthymic disorder (DD), in children and adolescents, is a mood disorder characterized by chronically depressed and/or irritable mood for more days than not, over a period of 1 or more years, with no remission longer than 2 months [19]. The clinical validity of early onset DD as a diagnostic construct has been established [20] and high rates of co-occurring externalizing disorders have been reported [21]. Early clinical and epidemiological studies in children and adolescents found rates of co-occurrence with ADHD-CT from 0% to 57.1%, and with ODD/CD from 21% to 83% [22]. According to Kovacs et al. [23], in a group of 55 children with DD, ADHD (predominately ADHD-CT) was the most prevalent pre-existing condition (24%). DD lasts almost 2.5 years longer in the presence of a cooccurring externalizing disorder [24].
Both ADHD-CT and DD frequently co-occur with other internalizing disorders. Epidemiological studies report anxiety disorders in 30% to 75% of children and adolescents with DD [22], while Kovacs et al. [23] report anxiety disorders at a rate of 40% in a clinical DD sample. The co-occurrence of depressive and anxiety disorders in children and adolescents has been associated with an increase in severity of depression [25], anxiety [26], and both syndromes [27]. Similarly, clinical studies report a prevalence of between 43% [28] and 63% [29] of children with ADHD-CT (DSM-III/DSM-IV diagnostic equivalent) and anxiety, while large-scale epidemiological studies report rates of approximately 25% [6]. Evidence is emerging that a subgroup of these children have a lesser response to psychostimulant medication in the short- and longer-term [29–31] and their anxiety (parent-reported) may not decrease with increasing age [32], [33]. To date, the characteristics of specific internalizing and externalizing disorders associated with DD and ADHD-CT have not been systematically investigated in a child and adolescent sample.
The aim of this pilot study is to examine the patterns of co-occurrence of specific internalizing and externalizing disorders in clinically referred samples of children and adolescents in three diagnostic groups: (i) ADHDCT without DD (ADHD-CT); (ii) ADHD-CT with comorbid DD (ADHD-CT + DD); and (iii) DD without ADHD (DD). Both categorical and dimensional diagnostic approaches will be used, and as dissonance between parent and child report of anxiety symptoms has been previously noted [29], [32], [34], [35], anxiety data will be collected from both the parent and the child perspective. Our hypothesis is that the ADHD-CT and DD group will have increased rates of both internalizing and externalizing disorders compared to both the ADHD-CT and DD alone groups.
Method
Subjects
Medication naïve children and adolescents aged 6–17 years were consecutively referred for a comprehensive psychiatric evaluation to either a specialized clinic for ADHD-CT or for depressive disorders (dysthymic disorder and major depressive disorder) because they were not responding to usual clinical psychological management approaches delivered at a community primary care level. Forty-five children consecutively identified with ADHD-CT (n = 15), DD (n = 15) or both ADHD-CT and DD (n = 15) according to DSM-IV criteria were included in the study. ADHD-CT (DSM-IV criteria), was defined through a semi-structured clinical interview with the child's parent(s) and by the parent and/or teacher report of the subscale scores of the core symptom domains of ADHD-CT being greater than 1.5 standard deviations above the mean for a given child's age and gender (Abbreviated Connors' Rating Scale [ACRS] [parent] 22.20 [5.24]). DD and anxiety disorders diagnoses were defined by a semi-structured clinical interview with the child's parent(s) and/or the child and by the parent and/or child report of total respective depression (Child Behaviour Checklist [CBCL] anxiety/depression subscale [parent T-score] 71.34 [10.10]; CDS total depression subscale [decile] 8.19 [1.83]-DD group) and anxiety (CBCL anxiety/depression subscale [parent T-score] 68.21 [(11.31]; RCMAS total anxiety subscale [T-score] 53.98 [11.88] Anxiety disorders group) scores being greater than 1.5 standard deviations above the mean for a given child's age and gender. The children met the inclusion criteria of living in a family home (and not in an institution) and attending normal primary schools. All had Intelligence Quotients above 70 and none had overt neurological disease, psychotic symptoms, conduct disorder or current major depressive disorder. There was no refusal and parent(s) gave informed consent. Ethics committee approval was obtained for the study. The three groups were compared for age, gender, verbal, performance and fullscale IQ, parental psychopathology, general family functioning and social adversity factors (Table 1). One-way analysis of variance (ANOVA) was used for this comparison with the posthoc Scheffe test to determine the source of a significant omnibus F statistic. The three groups did not significantly differ except for the ADHD-CT alone group, which had a significantly lower verbal and full scale IQ than the other two groups.
Subject characteristics
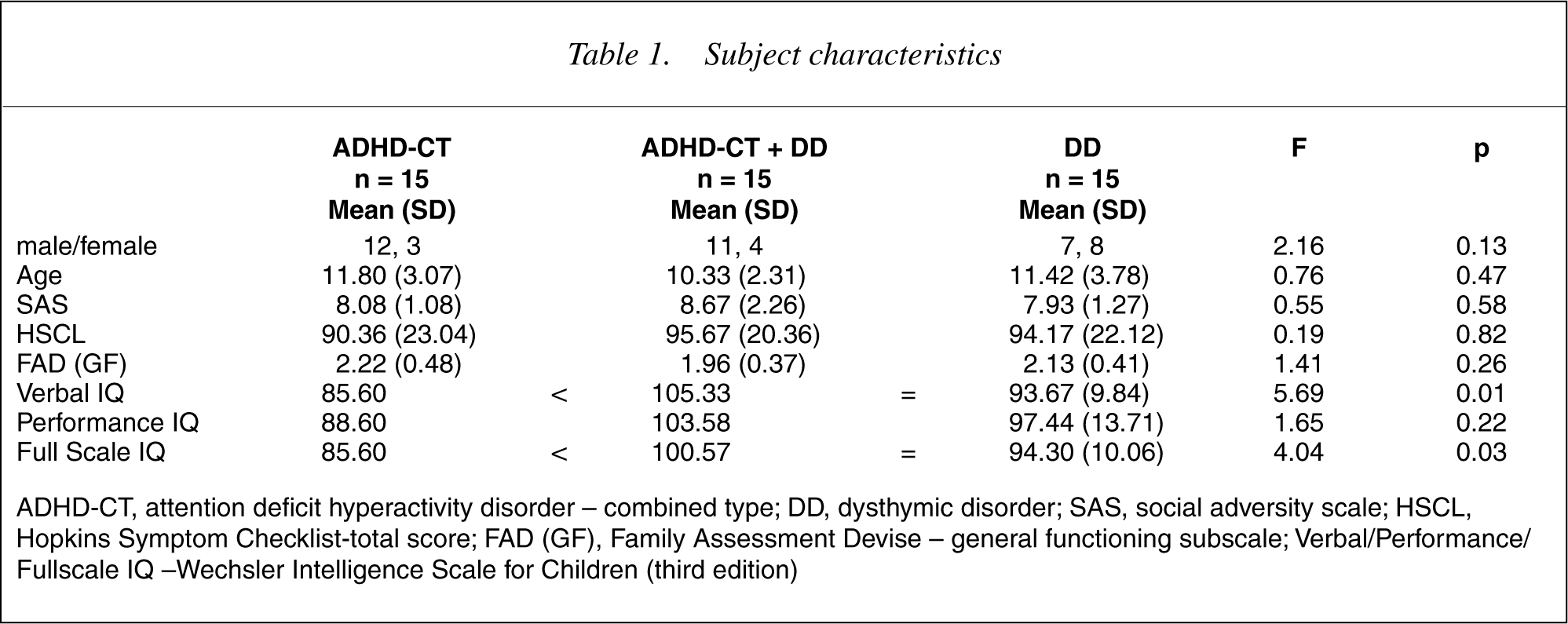
ADHD-CT, attention deficit hyperactivity disorder – combined type; DD, dysthymic disorder; SAS, social adversity scale; HSCL, Hopkins Symptom Checklist-total score; FAD (GF), Family Assessment Devise – general functioning subscale; Verbal/Performance/ Fullscale IQ –Wechsler Intelligence Scale for Children (third edition)
Measures
All measures used in this study are noted in the References section of this paper [36–44]. They have been described in detail in prior papers from our group [29], [32].
Procedure
The ACRS parent and teacher forms and CBCL parent forms were completed prior to the child's assessment. A Fellow in child and adolescent psychiatry interviewed the child and completed the Anxiety-Disorders Interview Schedule for Children (A-DISC-child version). The child also completed the Child Depression Scale (CDS) and the Revised Children's Manifest Anxiety Scale (R-CMAS) during this assessment. Parents concurrently completed the Hopkins Symptom Checklist (HSCL) and the Family Assessment Devise (FAD). At a separate session, the fellow in child and adolescent psychiatry administered the A-DISC-parent version and the Parental Account of Childhood Symptoms (PACS) while a registered psychologist administered the Wechsler Intelligence Scale for Children, third edition (WISC-3).
Data analysis
The Statistical Package for the Social Sciences (SPSS/SC) [45] was used to compare total reported comorbidities (dimensional variable of disorder present on parent and/or child report) of anxiety disorders, major depressive disorder, ODD, CD, and parent report of externalizing symptoms across the three groups using one-way ANOVA. Where the omnibus F was significant, the posthoc Scheffe procedure was conducted to determine the source of this significance. Statistical significance was set at the 5% level (p < 0.05) without bonferroni correction for multiple comparisons, given the hypothesis generating aim of this preliminary study.
Results
The rates of anxiety disorders across the three groups are presented in Table 2. Rates of these comorbidities on parent report, child report and total cases (disorder present on parent and/or child report) are shown. Generalized anxiety disorder and separation anxiety disorder were more frequently reported in the ADHD-CT + DD and the DD alone groups than the ADHD-CT alone group.
Parent-reported, child-reported and total comorbid diagnoses
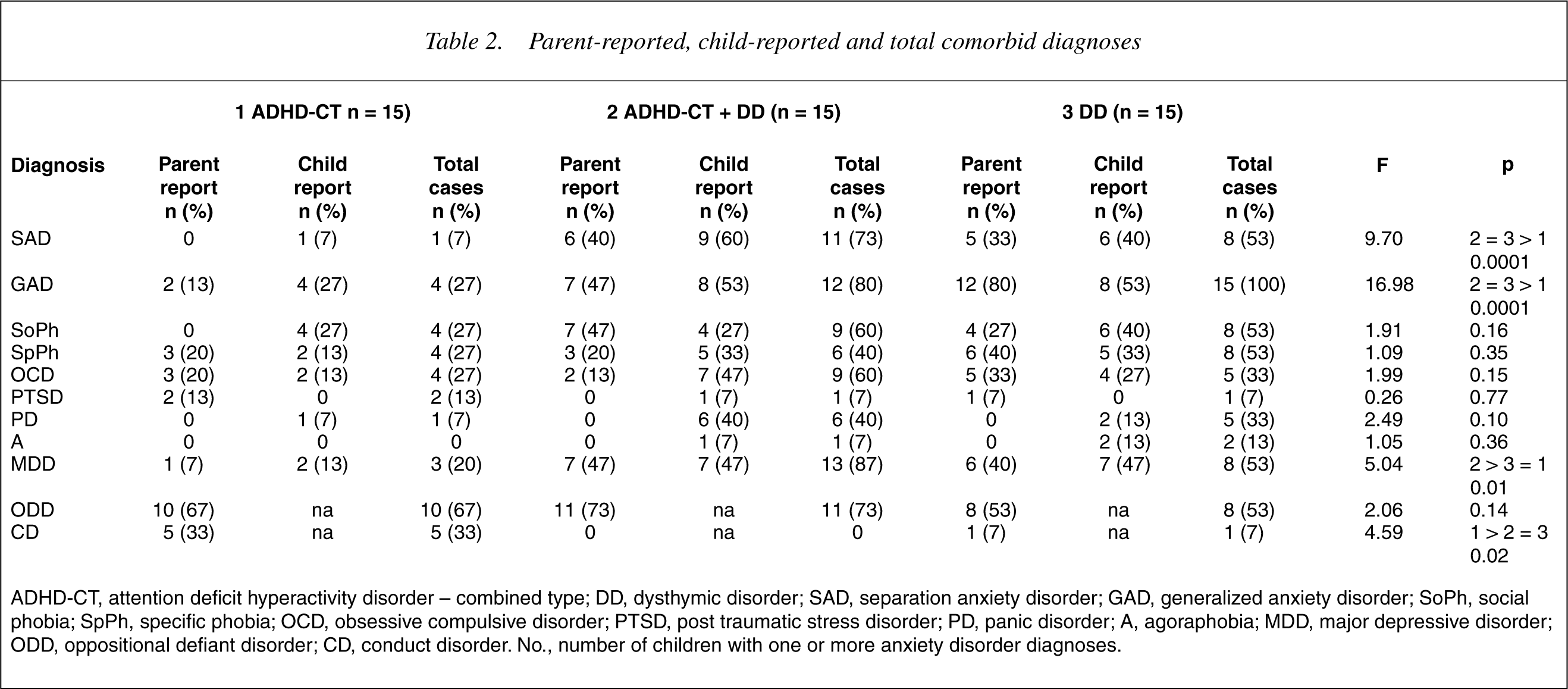
ADHD-CT, attention deficit hyperactivity disorder – combined type; DD, dysthymic disorder; SAD, separation anxiety disorder; GAD, generalized anxiety disorder; SoPh, social phobia; SpPh, specific phobia; OCD, obsessive compulsive disorder; PTSD, post traumatic stress disorder; PD, panic disorder; A, agoraphobia; MDD, major depressive disorder; ODD, oppositional defiant disorder; CD, conduct disorder. No., number of children with one or more anxiety disorder diagnoses.
Major depressive disorder was significantly higher in the ADHDCT + DD group compared to the ADHD-CT alone and DD alone groups. The rate of parent reported externalizing symptoms and ODD were not significantly different across the three groups. However, CD was significantly higher in the ADHD-CT group when compared with the other two groups.
Discussion
The group of children with ADHD-CT alone had lower verbal and full scale IQ when compared with the other two groups. This is consistent with previous studies demonstrating that children with ADHD-CT perform more poorly on standard measures of intelligence and particularly have a lower verbal IQ: performance IQ ratio than control subjects [46–48]. Interestingly, DD comorbid with ADHD-CT was associated with a significantly better verbal and fullscale IQ, suggesting that comorbid DD may confer a protective effect.
Our data show that the rate of anxiety disorders in children and adolescents with DD, with and without ADHD-CT, is high, a finding supported by previous clinical [23], [24], [49] and community-based studies [50], [51]. Further, ADHD-CT does not increase the risk of anxiety disorders. In this study, in both the ADHD-CT + DD and the DD groups, generalized anxiety disorder (80–100%) was the most commonly reported anxiety disorder diagnosis, followed by separation anxiety disorder (53–73%). These findings are higher, but consistent with, the literature. Masi et al. [49] report, in children and adolescents with DD, co-occurring generalized anxiety disorder at rates of 55% and 67%, respectively, and separation anxiety disorder at rates of 33% in the 7–11 years age group. A community-based study of adolescents with DD by Flament et al. [51] reported rates of generalized anxiety disorder of 23.8%, and separation anxiety disorder 14%. Both of these studies aimed to delineate the specific profile of symptoms in ‘pure’ DD, and thus excluded those with co-occurring major depressive disorder (i.e. those with ‘double depression’). A communitybased study by Goodman et al. [50] comparing children with ‘pure’ DD and ‘double depression’ found rates of generalized anxiety disorder of only 9% in the DD only group and 44% in the group with ‘double depression’. The present study utilized a clinically referred sample and did not exclude those with co-occurring past MDD, which may account for the higher rates of anxiety disorder seen. In addition, a recent study of clinically referred children with ADHD-CT [32] found co-occurring diagnoses (parent report) of generalized anxiety disorder at a rate of 50% and separation anxiety disorder 17%, which are higher than our rates of 27% and 7%, respectively, in the ADHD-CT alone group. However, if our ADHD-CT and ADHD-CT + DD groups are combined, these previously reported results are consistent with the current findings.
The rate of children and adolescents with DD, who had a ‘double depression’ was between 53% (DD only group) and 73% (ADHD-CT + DD group). This is consistent with rates reported in three previous studies [21], [23], [24], but higher than the rates of 17% and 30% in more recent reports [50], [51]. This higher rate of ‘double depression’ in the ADHD-CT and DD group is important clinically because young people with ‘double depression’ are more impaired, less socially competent, more likely to have comorbid anxiety [50], and have higher rates of suicide attempts and pathological behaviours (e.g. rule violation and pathological lying) [51], [52] than those with one diagnosis only (pure DD or pure major depressive disorder). Also, the course of both depressive and ADHD-CT symptoms is prolonged in this clinical group of young people [24]. Therefore, early recognition and future trials of more specific medication and psychological treatments for this group are needed. Further, these data suggest that comorbid ADHD-CT and DD may have an additive effect for the occurrence of major depressive disorder, which may be associated with particular additive biological and/or environmental vulnerabilities.
The presence of co-occurring ODD and CD are well described in children with ADHD-CT [2], [3], [6], [32], [22], [23]. In the present study, the ODD rates were increased in all groups (53%-87%). This is somewhat higher than previously reported rates in ADHD-CT (30%–50%) [6], but is not inconsistent with previous literature of depressive disorders [22]. The rate of ODD was not significantly different between the three groups. This is further evidence that suggests the need for careful clinical assessment of oppositional defiant patterns of behaviour and conduct problems in young people, given the importance of identifying early and treating cooccurring ADHD-CT and/or DD.
The rate of CD in the ADHD-CT only group (33%) was within the expected range of 30%–50% [6], while the absence of CD in the ADHD-CT + DD group was much lower than the previously reported minimum rate of 22% [53]. The rate of CD in the DD group (7%) was within the range of 6% [17] and 40% [54] previously reported. Thus, the rate of CD in our sample of patients with ADHD-CT + DD is much closer to those reported for pure DD, rather than ADHD-CT. This may be explained in part by the clear distinction of ODD and CD in this study, rather than considering these two diagnoses as one dimension of conduct problems [6]. Importantly, it does suggest that comorbid DD may confer a protective effect.
In summary, we have demonstrated the preferential association of anxiety phenomena with DD compared to ADHD-CT in a small sample of clinically referred children and adolescents. Currently, there is emerging evidence that DD and anxiety may represent different phenotypic expression of a common underlying aetiological process [55], while the co-occurrence of ADHDCT and anxiety disorders remains unclear [56]. Our data are consistent with this emerging evidence. Only the ADHD-CT and DD group is significantly associated with major depressive disorder, which suggests an additive effect. In contrast, conduct disorder and decreased verbal and fullscale IQ are only associated with the ADHD-CT group, which may suggest a protective effect of DD when comorbid with ADHD-CT. From a research perspective, it is important to confirm these found associations in larger samples derived from epidemiological populations, using a longitudinal study design. In addition, from a clinical practice viewpoint, systematic investigation of further clinical correlates of ADHD-CT and DD and more specific psychological and/or medication treatments that may lead to better clinical outcomes are needed.