
Abstract
Few topics have attracted the amount of attention and controversy as the prediction of risk of violence. Psychiatrists were once said to owe more to magic or art than to science in predicting dangerousness [1]. Despite this, they were expected to assess the risk of violence in their patients [2], [3] and were cautioned not to ‘use the mantra of unpredictability’ [4]. Assessment of risk is now seen as a specialized skill [5], [6] that has moved from the traditional province of forensic psychiatrists [7] to general psychiatrists who assess risks as frequently as forensic psychiatrists [8]. Over the last decade in forensic psychiatry, risk prediction has given way to risk management [9–11] whereas many general psychiatrists may still be preoccupied with risk prediction. The literature on risk assessment originated from forensic settings, has been written by forensic psychiatrists and is applicable to forensic patients. It may not apply to general psychiatric setting. The patient population clearly differs between forensic and general adult settings, approaches to risk assessment differ and so does the nature of risk assessed. Forensic patients will have already offended and most general psychiatric patients will not.
Two broad types of approaches for risk assessment are described in forensic psychiatry, the actuarial (a risk factor based ‘league table’ approach) and the clinical (a ‘formulative’ approach which, although informed by risk factors, attempts to define patterns of risk behaviour for that person). They have been compared as ‘climate’ vs ‘weather’ approaches to prediction (the former longterm, the rather short-term and specific) [12]. An actuarial risk assessment tool such as the Violence Risk Assessment Guide (VRAG) [13] was developed in a forensic population and aims to give a risk of re-offending over long time periods. It may be helpful for a forensic psychiatrist making a disposal recommendation. Most general psychiatrists, on the other hand, are interested in assessing the risk of violence say 1 month after discharge from the hospital. Similarly, psychiatrists working in secure forensic settings tend to assess assault risk within the hospital setting versus long-term risk of violence in the community by general psychiatrists [9]. Furthermore, violence is less common in general psychiatric population compared to the forensic population.
General adult psychiatrists need to develop a system of risk assessment specific to their needs and context. For instance, take the case of a 29-year-old man who presents with a first episode of schizophrenia, with no past history of criminal conviction but is hearing voices commanding him to shoot children in a local primary school. The assessing general psychiatrist will find using an offender based risk assessment tool such as the VRAG [13] unhelpful, because it was not developed to assess this type of risk. Yet a formulation of the particular experience of the patient including affect, motivation and delusion driven behaviour will be of much more assistance. It is from this type of context that we set out to summarize the current state of knowledge of risk assessment and adapt the information to meet the needs of a general adult psychiatrist.
This paper will examine the way risk has been conceptualized in different disciplines, the impact of safety culture on psychiatric thinking, and the methods of risk assessment in forensic psychiatric literature, with a view to apply relevant principles in general psychiatry. We define the risk we are referring to as the probability that a person may commit a violent act against another person in the future, in certain circumstances. Topical issues from forensic psychiatry including the benefits of shifting from risk prediction to assessment, management and reduction of risk, communication of risk and the need to involve patients in the process of risk assessment are examined.
Method
We searched the Medline database [1993–2003]. The following key words were used: violence and risk management and risk assessment (narrowed to human and English language, prevention and control = 709 papers). Key articles were identified and the search was supplemented by cross-referencing. SK, a general psychiatrist, examined their appropriateness and relevance to general psychiatry. AS, a forensic psychiatrist with a special interest in risk management of violence in forensic psychiatric population identified the forensic literature on the subject. Essentially while one author identified good quality studies on the assessment, management and prediction on risk of violence, the other author identified those papers that had relevance to general psychiatry but both attempted to find approaches relevant to general adult psychiatry.
Risk conceptualization
Risk assessment is not unique to psychiatry and by no means within psychiatry is limited to the assessment of risk of violence alone. We found similarities in the principles of risk assessment between as divergent disciplines as environmental science and psychiatry. Take for instance the way Dwivedi [14], an environmental scientist, defines risk as ‘the possibility of beneficial and harmful outcomes and the likelihood of their occurrence in a stated time scale’. This definition has at least three key features: Uncertainty: Risk is assessed only when there is uncertainty about possible outcome(s) or to ascertain the probability of different outcomes occurring. The exercise of risk assessment would cease to have any meaning should one be absolutely certain about the outcome. Weighing up the likelihood of different outcomes arising: In assessing risk one contemplates either to act or not to act or even compares the possible outcomes of one course of action versus another. Possibility of benefits as well as harm: There is a general tendency to focus on the harmful consequences only while assessing risk, which prompts us to intervene. Not all interventions are safe and sometimes harm secondary to intervention may outweigh the risk of non-intervention. Before any interventions are introduced such risk benefit analysis should be carried out carefully. In this paper we restrict ourselves with the assessment of risk of violence by people with mental illness. General psychiatrists are often concerned about the assessment of several types of risk including risk of suicide, damage to property, being a public nuisance, of relapse of illness, side-effects or adverse reactions to psychotropic medication, etc. Such risks are beyond the scope of this paper and will not be discussed.
The occurrence of any adverse event including risk of violence requires the presence of three factors: a perpetrator, a potential victim and an environment or opportunity for the event to occur. Any attempt to manage the risk of all adverse event aim to alter one of these three and where efforts are directed largely depend on the discipline and of the ability to intervene. An environmental scientist may have limited control over the perpetrator (e.g. a tornado occurring) and may choose to focus on removing the potential victims (e.g. people living in that area). A psychiatrist on the other hand is very often expected and required to focus on the potential perpetrator of violence (the patient) while also juggling with the potential victim's right to be informed and protected as well as manipulating the environment. Furthermore, once a psychiatrist assesses a situation as having unacceptable risk he/she also introduces certain interventions, which lead to a modification in the original level of risk [10], [12].
Safety culture
Safety culture is the collection of beliefs, norms, attitudes, roles and practices one uses while going about daily activities, including management decisions in a broader context [15]. This construct is concerned with how risk and danger are perceived. Recognition of the safety culture of an organization is easier than defining it and unfortunately it is easier to understand when it is violated rather than adhered to. There are similarities between the causation of accidents in general and homicides committed by mentally ill patients and one such similarity being the breakdown of safety culture of the organization where an accident or homicide takes place. In other words, any disaster is seen as failure of safety culture [15]. Attributes commonly associated with violation of safety culture include lack of concern, poor morale, violation-condoning norms, a ‘macho attitude’ and poorly expressed rules [16]. These factors, or their parallels, are commonly reported in homicide inquiries committed by people with mental illness [4], [5], as are more general issue in relation to the structure of the mental health services as a whole, including resourcing, organization and appropriate legislation [17], [18]. The general adult psychiatrist needs to be aware of the construct of safety culture, its maintenance, detection of violation and the consequences of nonadherence. A safety culture in mental health systems provides a matrix of infrastructure and expectation of performance of the systems and the individual practitioner [4]. This trend underscores the need to involve multidisciplinary clinical teams in risk assessment and management.
Risk assessment: general principles
Assessment of risk, in most disciplines, is a two-stage process: identification of risks and risk estimation (of the probability and severity of harm associated with them) [14]. We prefer these terms to risk-prediction which has often been the focus in psychiatric literature. We like them because they focus on the process rather than the outcome. As we will discuss later outcomes of risk prediction in psychiatry is likely to be unreliable. Identification of risks has been seen by others as the first step in the assessment of risk and involves recognizing the existence of a particular hazard and the definition of its characteristics. The second step in the process of risk assessment is risk estimation, which involves the use of scientific or technical tools to quantify the nature and characteristic of the hazard under investigation into measurable terms. Results from steps 1 and 2 (risk identification and risk estimation) are recommended to be used to evaluate the significance and acceptability of risk in question. In environmental sciences specifically, risk is seen as assessing the magnitude of adverse consequences of an event or exposure, and risk evaluation refers to the process of evaluating the acceptability of risks, or what constitutes ‘safety’. We believe most good psychiatrists who strive to select the least restrictive method of treatment for patients while also attempting to protect society take such an approach.
In our view risk identification and risk estimation are carried out by examining three aspects of risk: probability, imminence and severity of outcome [11]. Severity is the context of the incident that has brought the patient into attention and is always considered after an adverse incident has occurred. Probability on the other hand is concerned with the chances of violence being repeated and typically actuarial methods are used to evaluate probability. Actuarial methods concentrate on identifying sets of risk factors associated with violence based on prospective or retrospective studies [19]. Finally, imminence is defined by the pattern of violence in the per-son's prior career as well as their statements, plans, target availability and life circumstances. It is our opinion that clinical or descriptive methods are often used to explain imminence, including the contextual factors necessary to understand risk emergence. The clinical approach is described as ‘a theoretically based decision making process which proceeds by posing and testing clinical hypotheses derived, at least implicitly, from a theoretical model of human personality and behaviour’ [19], pp. 97]. Both (actuarial and clinical) approaches form the cornerstones of risk assessment in psychiatry and will be described in greater detail.
Risk assessment in forensic psychiatric literature
Actuarial approach
Several studies have attempted to identify ‘predictors of violence’ in mentally ill populations. Variables described as ‘actuarial’ are defined as variables that can be measured with little, if any, expert judgement [9]. They are largely considered ‘static’ because they refer to personal variables (age, gender, past behaviour, age at first offence) that change little, if at all, over time or in response to interventions [20]. They have been considered superior predictors of violence by Quinsey et al. [13] who recommended not simply ‘the addition of actuarial methods to existing practice, but rather the complete replacement of existing practice with actuarial methods’ as being the only valid approach to risk assessment. It has also been said that when clinical judgements are incorporated into actuarial predictors, their accuracy decreases [11].
The utility of actuarial tools is restricted by their limited generalisability. They are best suited for the populations who have characteristics similar to those on whom they were originally validated [11]. Some actuarial tools, e.g. VRAG [13]; Macarthur Guided Decision Making Scale [21] have been developed on forensic (offender) populations or on very diverse clinical populations. They also make predictions of limited clinical validity. For instance the VRAG [13] makes ‘accurate’ predictions of the percentage risk of re-offending that a person is at in the next 7 years. Further, the VRAG was developed in offender populations, not general adult psychiatric populations. A different approach to guided clinical judgement is the Iterative tree model developed from the McArthur Risk data [21]. This approach allocates a person to a category of risk, but doesn't assist the psychiatrist understand the origin of those risks in a manner that informs intervention.
The clinical approach
Clinical variables are defined as ‘dynamic factors that can change’ [20], pp. 155] or personal factors or variables that require the use of human judgement to measure including clinical and mental state attributes [9]. Most actuarial tools designed to assess dangerousness rely on the clinical assessment of clinical variables. When evaluating clinical data psychiatrists follow a logical process of reasoning, which is often summarized in clinical reports. In this process, psychiatrists also use subjective evaluation and clinical experience. As subjectivity enters risk assessment the outcome may be dependent on the individual psychiatrist's skills and acumen. Sarbin [22] differentiates between the organizing principle or thought used in the actuarial (outlined above) and the clinical approach used in the assessment of risk of violence. Risk factors are variables associated with an outcome but make no assumption regarding causation. A statistical mode of thought is used in the actuarial approach whereas a narrative model of thought is used in the clinical approach. The latter model of thought involves the process of organizing or integrating happenings and actions into a comprehensible story. The narrative approach is thought to be ideally suited to providing the explanation in order to satisfy the need of understanding motives in the ascription of culpability [19]. This approach has proven effective in developing the understanding of ‘what went wrong’ in several recent inquiry reports of violent incidents committed by the mentally ill in the UK [5]. In contrast to actuarial methods, the clinical approach considers the seriousness of possible harm and is often reliant on team perspective as opposed to individual psychiatrist's assessment, rather than the statistically derived, atheoretical basis of strict actuarial assessment, clinical risk assessment is formulative, integrative and develops a causal hypothesis for risk of violence in this person. The hypothesis is of course tested and reviewed as time goes on. It must be informed by, but not limited to, risk factor research, identifying factors that are relevant for this person and their circumstances.
Litwack [9] in an excellent review comparing actuarial and clinical methods of risk prediction found that the evidence to say one is superior to the other is lacking, and noted that actuarial assessments also actually require clinical judgement.
Toward integration
One tool that has been developed from more clinically, informed models has attempted to use the information from actuarial information, and combine it with clinical and situational data to make a more clinically meaningful rating system. This tool, the HCR 20 violence risk assessment scheme [23], employs risk factors derived from studies on violence and mental disorder, and helps direct clinician attention to these areas in conducting a comprehensive assessment. It has been developed on forensic and civil populations. We summarize these factors in Table 1. The HCR 20 aligns risk markers into past (historical), present (clinical) and future (risk) circumstances to guide the clinician to relevant considerations. Its 10 historical factors concern those from the past, which are largely unchangeable, five clinical items reflect current dynamic changeable factors, whereas five risk items are those that may either mitigate or aggravate risk. The HCR authors have more recently added a final overall judgement entitled a ‘Structured Professional Judgement’ which is guided by but not limited to the items, but represents the clinicians overall synthesis of the risk. This item has been shown to improve the predictive properties of the HCR 20.
HCR 20 violence risk assessment scheme [24]
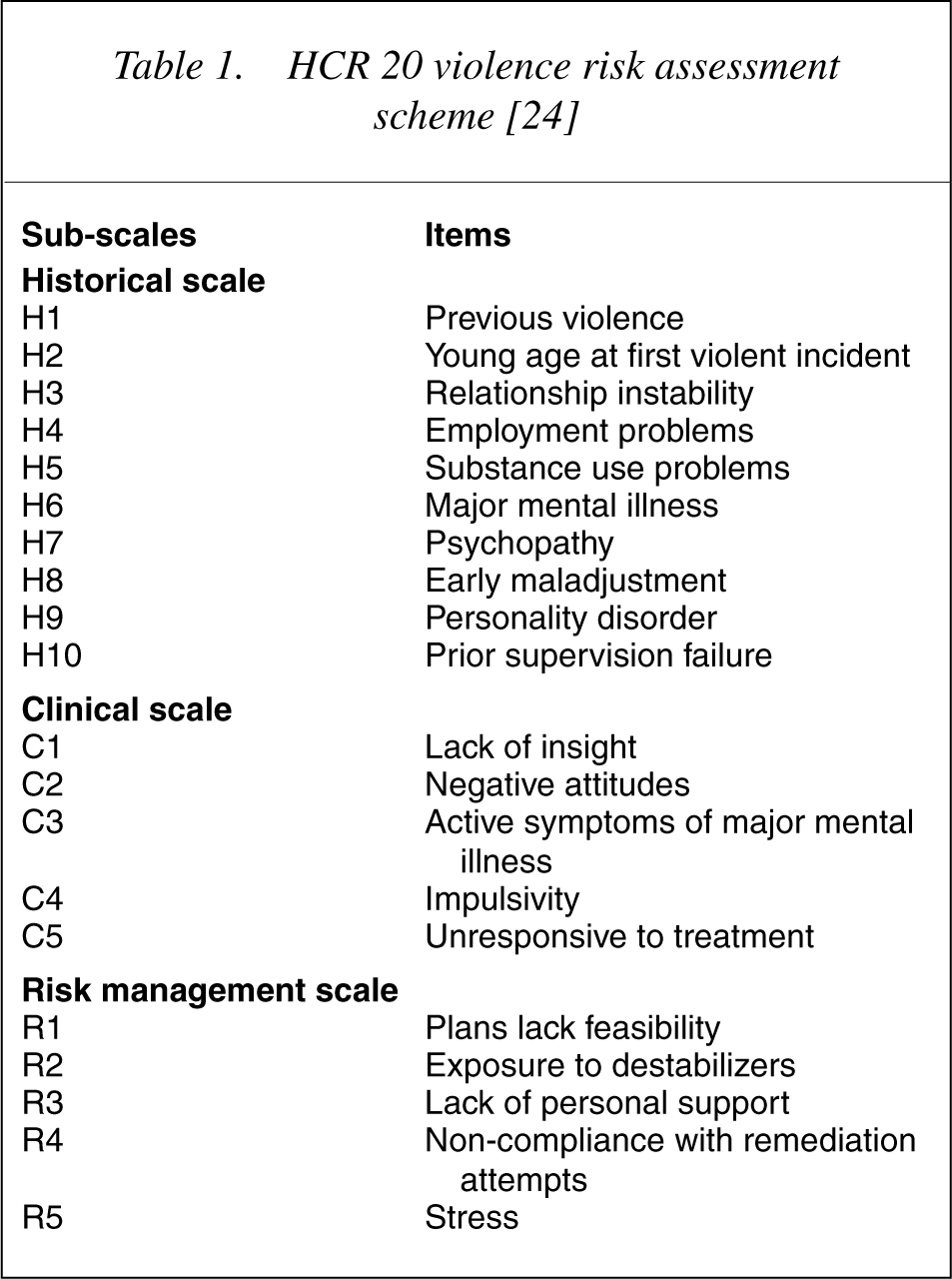
We believe that these 20 factors serve as a valuable ‘aide memoir’ for busy psychiatrists as these factors have strong face validity and the HCR 20 has been tested on general adult psychiatric population. These factors may assist busy general psychiatrists who may not be familiar with the actuarial tools and be constrained by time restriction. The item for psychopathy is very unlikely to be measured in routine clinical use in general population, but other historical factors overlap with this concept.
What is needed for general adult psychiatrists?
Merge actuarial and clinical approaches
In our view, the best approach appears to be developing in the structured clinical judgement approach to risk assessment, where a psychiatrist, informed by the risk factor literature, considers the presence and meaning of particular risk factors relevant to this person, and formulates the risk on that basis. In this way actuarial tools serve as ‘aide memoir’ while clinical methods elucidate the dynamic nature of long-term risk relevant for an individual patient, leading to an overall, structured clinical judgement.
Shift from risk prediction to risk assessment and management
Clinical practice and discourse is at risk of becoming too risk focused. Perhaps under pressure from the combined effects of media's preoccupation with the infrequent but severe cases of violence committed by mentally ill patients, we face impossible pressures to anticipate all such events. What we are, are treating clinicians. Our task is, as always, to relieve suffering consequent on serious mental illness. To do this, we must understand how illness may lead to violence in a manner that informs intervention.
If psychiatrists are preoccupied with predicting violence they are likely to be wrong two out of three times [10]. If they develop the skill of assessment of risk by risk formulation [10] and risk management [11] they are likely to achieve better results. The distinction between these tasks is subtle but significant. A clinical determination that a patient presents sufficient risk to justify intervention is the goal of risk assessment. On the other hand the task of prediction of violence is essentially concerned with predicting that the patient will be violent if some form of legal action is not taken. A classic study in this regard was conducted by Lidz et al. [24] who reported that clinicians were reasonably accurate in assessing dangerousness because the patients who did prove to be violent on follow up over 6 months were detected with reasonable sensitivity. On the other hand, many patients who were rated as dangerous by clinicians did not prove to be more violent than the other patients. In contrast, a clinical determination that a patient presents sufficient risk to justify intervention is the goal of assessment of risk. Risk assessment must identify clinical or situational factors that can be modified to reduce risk. It is noteworthy that inquiries into homicides by persons with mental illness have consistently found that only a minority of incidents were predictable, whilst the majority are preventable with good quality clinical assessment, communication and intervention [17], [25]. We ought to use our psychiatric training to introduce interventions according to the needs of an individual and master the art of risk management by constantly considering the dynamic nature of risk and paying attention to the needs and deficits of an individual.
The issue of shifting focus from risk prediction to risk management becomes more relevant when one considers the ethical implications of the two. Very often and unwisely, the outcome of risk assessment is that a given patient with a history of violence is identified as ‘potentially violent’ which easily gets distorted as ‘violent’. These adjectives accumulate in the file and are of little utility unless ways are identified to manage risk. Our responsibility as psychiatrists will not and should not end with stating that a given patient is potentially dangerous. The only ethical justification for risk assessment by a treating psychiatrist is risk reduction through risk management. Risk identification and risk estimation should be integrated with risk management to reduce the risk under consideration. This will serve as a reminder that risk changes with time and circumstance and therefore risk of violence needs to be assessed and reviewed regularly. As a corollary, if the person is not reviewed after a certain period then ‘the label’ should also cease to have any meaning. In this way the stigma associated with the label can be minimized.
Involve the patient
In the work of both forensic and general adult psychiatrists is the need to involve patients in their own risk assessment, if they are to be expected to understand why interventions are necessary. Too often this is not done well. Bowden [26] refers to this failure by noting ‘perhaps we do not listen to what our patients are saying because we can not bear to hear; we do not seek feedback because we may be challenged and be forced to defend our position…’ Patients not only perpetrate violence but they also witness and sustain violence and suffer the consequences. Yet their experiences as victims and witnesses of violence has been little explored [27], [28]. For patients who perpetrate violence questions about their personal risk of becoming violent again or how they feel about having been violent, and what triggers lead to violence are critical. Further their views of the assessment process and its outcome should be sought.
Significant differences are reported between staff and patient's perceptions of the precipitants of violence. There is a greater concordance between patients' and victims' perception of the precipitants of violence for items designated as objective or factual information but a substantial lack of congruence between their reports of subjective information about the precipitants of violence has been reported [29], [30]. Given the knowledge of triggers for violence in a patient, specific strategies can be developed to avoid or reduce them in the risk reduction plan. Asking direct questions about fantasies of violence, plans to harm, familiarity and access to weapons, motivation for self-control and stress management and empathy towards others especially potential victims have been recommended [10]. Monahan [31] suggested direct questions about indices of violent behaviour (e.g. arrest or hospitalization for danger to others). Being open and non-judgemental regarding these issues are likely to help establish a relationship based on partnership between the patient and the psychiatrist. They are often best asked after you have asked the patient if they have previously been a victim of threats or assault, followed by whether they have ever perpetrated threats or violence. The person's description of the circumstances, motivation, planning and outcomes of the actions needs to be carefully explored.
Communicate effectively and widely
In order to manage risk effectively the outcome of risk assessment needs to be communicated widely and effectively. The stakeholders in this regard include the patient, their family and agencies involved in the care of the patient. The need to have clear communication between all agencies involved in patient care and yet respecting the tenets of patient privacy and confidentiality has been emphasized time and again [5], [6]. We feel that risk communication should go one step further and examine the impact of risk assessment and its outcome on patient's lives. When communicating risk the language should be non-technical, understandable and words should ‘reflect, integrate, and convey the decision making rationale’ [11]. While communicating about the potential risk breaching confidentiality is justified if the risk is imminent, sufficiently specified, and disclosure leads to means to avert the danger [32]. In the specific context of risk of violence by mentally ill people, Heilbrun et al. [33] recommended three dimensions that clinicians need to consider while communicating risk (i) risk model (prediction versus management); (ii) risk level (high versus low risk of the individual being assessed); and (iii) risk factors (the predominance of static versus dynamic risk factors). Psychiatrists will need to acknowledge the status of knowledge about the actuarial factors used in the assessment and emphasize the dynamic and changing nature of risk. Ethical challenges may arise not only in identifying risk factors but also in communicating them to different agencies involved in the patients' care.
Conclusion
Prediction of risk of violence by mentally ill patients is a probabilistic activity, and one with major consequences for the patient, potential victims and the clinician. There are difficulties in applying actuarial techniques from forensic psychiatric populations to the general adult psychiatric population although clinically informed tools and formulative approaches are of most value. General adult psychiatrists need to combine actuarial and clinical approaches into structured clinical judgements and to shift from risk prediction to risk management. Emphasis needs to be given to the management and reduction of risk, by merging actuarial and clinical approaches, and to communication of risk. Patients need to be involved in the process of risk assessment. We will no doubt struggle to find a compromise between the competing needs to act in the interest of the community as agents of control, safety and custody while holding foremost the interest of the patient's health and welfare. The label of ‘violent mentally ill’ can have disastrous effects on the lives of patients, as can a failure to appropriately manage risk. Patients' involvement in the process of risk formulation is likely to improve the value of the assessment. Particular care needs to be taken while communicating the outcome of risk assessment. We need to balance the need to protect patient confidentiality and the need to share information in the interest of our duty to protect society and care for our patients.