
Abstract
Rapid cycling (four or more affective episodes per year) occurs in approximately 20% of patients with bipolar disorder. It is a distinct course modifier [1], and is associated with high rates of treatment resistance [2].
It has been repeatedly demonstrated that tests of hypothalamic-pituitary-adrenal (HPA) axis function are abnormal during relapse in patients with mood disorders. Whether this dysfunction is a trait marker or simply a marker of relapse can, in part, be considered by examining the axis in different mood states. Studies in unipolar depression suggests that the axis normalizes with symptom resolution [3]. In bipolar disorder, while the HPA axis is abnormal when patients are unwell, results from studies in recovered patients are more equivocal [4–6].
We hypothesized that glucocorticoid receptor (GR) dysfunction is a persistent abnormality in rapid cycling bipolar patients, and predicted that the response to the dexamethasone/corticotropin releasing hormone (dex/ CRH) test would remain unchanged between relapse and remission.
Method
Subjects
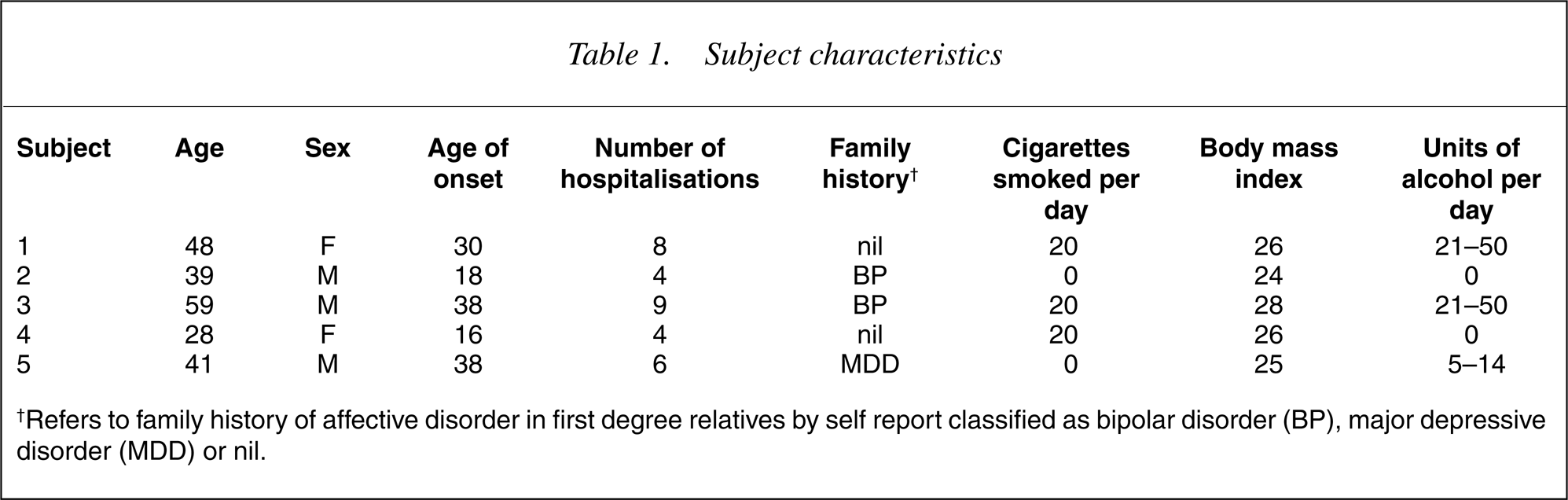
Five patients with rapid-cycling bipolar I disorder, recruited from out-patient clinics in the North-east of England, underwent the dex/ CRH test when in relapse and when in remission. Diagnosis was confirmed using the Structured Clinical Interview for DSM-IV (SCID). Clinical and demographic date are reported in Table 1. Exclusion criteria for the study consisted of a neurological or medical condition, prescription of corticosteroids or antihypertensive medication or a history of substance or alcohol abuse. The local ethics committee approved the study. All subjects gave written informed consent.
Subject characteristics
Neuroendocrine testing
The dex/CRH test and subsequent biochemical tests were performed following the standard protocol [6]. Inter and intra assay coefficients of variance for this laboratory for cortisol assays are less than 8%.
Statistical analysis
The response to the dex/CRH test was determined by delta (Δ) cortisol (the difference between peak cortisol response and the cortisol level at 1500 h, immediately prior to CRH infusion). Δ cortisol was normally distributed, tested by Levine's statistic. An independent samples t-test was used to compare responses in remission and relapse and Pearson's correlations were used to compare Δ cortisol between visits 1 and 2 (SPSS 9).
Results
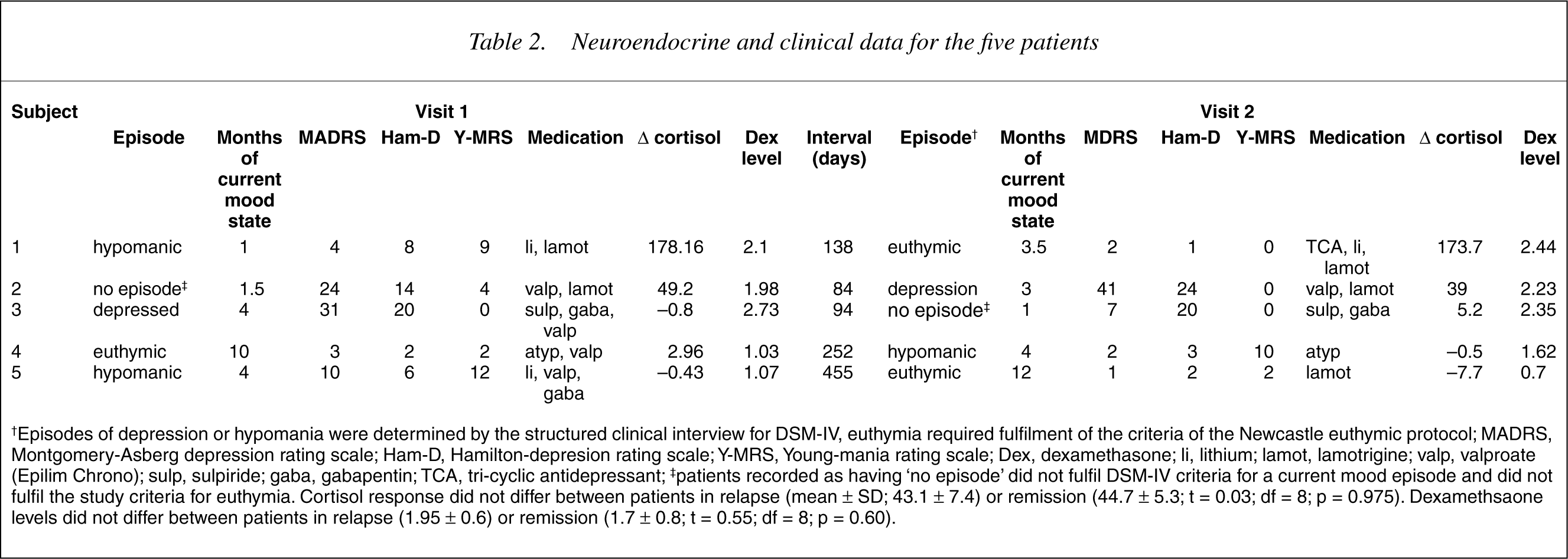
Δ cortisol correlated between visit 1 and visit 2 (r = 0.997; n = 5; p < 0.0005). Within each patient there was 2% difference in Δ cortisol values between the two visits. See Table 2 and Fig. 1.
Graph showing the temporal stability of the dex/CRH test.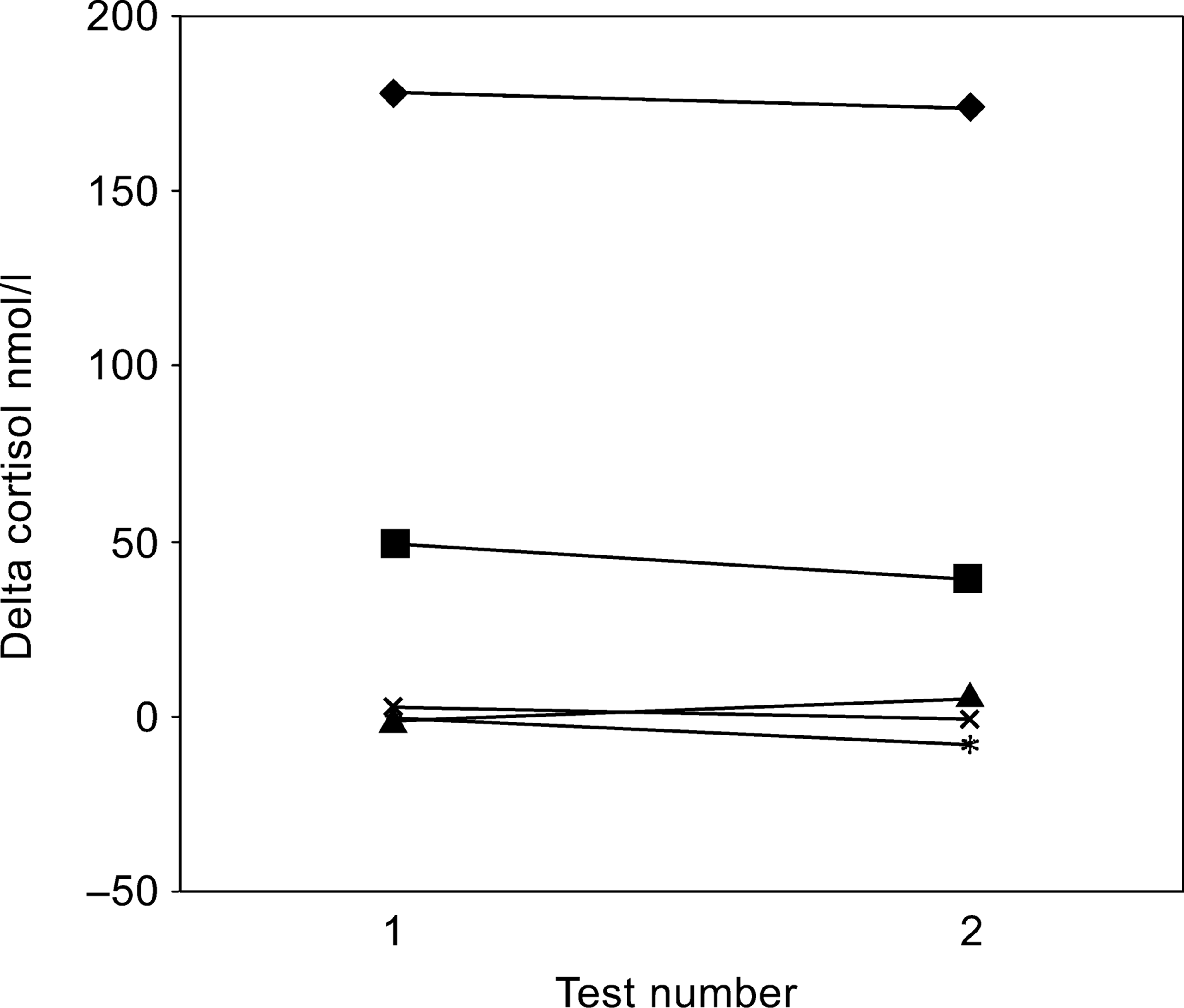
Neuroendocrine and clinical data for the five patients
Discussion
The cortisol response to the dex/CRH test was stable over time in rapid-cycling bipolar patients regardless of their mood state.
Previous studies have demonstrated that, in patients with unipolar depression, normalization of the response to the dex/CRH test is associated with symptom resolution [3], [7]. In patients with bipolar disorder, two separate groups have shown that the response to the dex/CRH test returns towards normal on symptom resolution [4], [5]. In contrast to this, in a cross sectional study on a population recruited largely from tertiary care (in which over a third of the patients fulfilled criteria for rapid cycling), we have demonstrated that the cortisol response to the dex/ CRH test did not differ between prospectively verified euthymic patients and patients in relapse [6].
There remains a paucity of data on HPA axis function in patients with rapid-cycling bipolar disorder. In a case study, Seifritz demonstrated stability of the dex/CRH response over time by testing one patient on four occasions in different mood states [8]. In previous prospective studies in rapid cycling patients, cortisol response to the dexamethsone suppression test (DST) was greater during relapse [9], similarly basal cortisol levels were found to be higher during and immediately preceding depressive episodes [10]. Our results support the hypothesis that GR function is persistent across different mood states in rapid cycling disorder. The discrepancy from the above prospective HPA studies may reflect differences in the clinical sample or the different time periods since the last episode. Schmizu and colleagues [11] describe a case in which the DST response normalized after 2 years of remission in a previously rapid-cycling patient, suggesting a long lag between symptomatic recovery and normalization of the HPA axis. In our study, three patients satisfied the criteria of the Newcastle euthymia protocol [12] and had therefore been in prospectively verified remission for at least the 4 weeks preceding the endocrinological investigation.
Three of the five patients in this study had delta cortisol levels within the normal range (95% confidence interval of the median) of healthy controls previously examined in this centre [6]. This shows that whilst GR function was stable in this study it was not always abnormal, suggesting that if GR dysfunction is, as has been hypothesized [6], a vulnerability factor, it may be valid only for a subgroup of patients.
The dexamethasone/corticotropin releasing hormone (dex/CRH) test measures HPA axis function, specifically glucocorticoid feedback sensitivity and the capacity of the HPA axis to respond to CRH drive [13]. Current opinion on the pharmacological treatment of rapid cycling disorder emphasizes treatment of the underlying disorder rather than the episode [2]. Glucocorticoid receptor antagonists have been shown to improve depressive symptoms and neurocognitive performance in patients with bipolar and unipolar disorder [14–16], particularly in patients with GR dysfunction [15]. The data in the present study supports the continuation of successful treatment with psychotropics (many of which impact on GR function [13]) in rapid cycling disorder across the spectrum of mood states.
This study has only 5 patients tested on 2 occasions and can be considered only to be a pilot study. Three of the patients fulfilled our criteria for euthymia [12] and 2 did not fulfil DSM-IV criteria for an illness episode (see 3], [17] and is a potential confounder. However, the stability of the response suggests that the medication changes between visits have not influenced the cortisol response.
In summary, this pilot study suggests stability of the cortisol response to the dex/CRH test that is independent of mood state in patients with the rapid-cycling form of bipolar disorder.
Footnotes
Acknowledgements
This study was supported by the Stanley Medical Research Institute. Margaret Smith performed the neuroendocrine tests. Anne Maule assisted in preparation of the manuscript.