
Abstract
Harris and Barraclough claim that excess mortality in persons with serious mental disorders has been ‘known from English vital statistics for 150 years’ [1]. The theories, and the evidence, concerning the possible causes of this excess are succinctly reviewed by Lawrence, Holman and Jablensky [2] who reported (inter alia) that, in Western Australia (WA) from 1985 to 1998, the overall mortality of persons with mental illness was two and a half times higher than that of the general population, the rate of deaths from ischaemic heart disease in the mentally ill was over twice that in the general population, and deaths from suicide in the mentally ill increased over time and represented about a half of all such deaths. As these findings have major implications for service delivery to persons with mental illness, and imply that ‘mortality’ could become an important outcome measure for mental health services, replication of their study is required in other jurisdictions.
The availability of a computerized record of all persons who had contact with the Australian Capital Territory (ACT) Mental Health Service (MHS) since 1985, and access to the National Death Index maintained by the Australian Institute of Health and Welfare (AIHW), allowed a study of mortality to be undertaken for the ACT. The computerized data system of the MHS was initiated in 1985 and was repeatedly upgraded until 1995.
Method
Approval for this study was obtained from the ethics committees of the ACT Department of Health and the AIHW.
People aged 14 years and younger were excluded from all consideration.
Following the approach used in WA, a list of all persons (identified by name, sex and date of birth) who contacted the MHS between 1985 and 2000 was compiled from the computerized data collection maintained by the MHS. This list was matched by AIHW staff with the National Death Index. AIHW supplied the author with the name, sex, date of birth, date of death, cause of death, and location of death, of all of the persons on this list who died in Australia from 1990 to 2000. For each year from 1990 to 2000 the age at death, sex, and cause and place of death of all deaths among the mentally ill were tabulated. Data for the period 1996–2000 were aggregated.
After amendment (by removing probable duplications, names added after 1996, and persons dying before 1996) ‘the list’ was used to represent the mentally ill population of the ACT (the mentally ill) for 1996. The mentally ill population in 1996 was categorized by age and sex.
Similarly, using Australian Bureau of Statistics data, the age, sex, and cause of all deaths occurring in the ACT for the period 1996–2000, and the age and sex of the total population of the ACT in 1996, were tabulated.
Following Lawrence et al. [2], data were processed for all deaths (deaths from all causes), deaths from ischaemic heart disease, and deaths from suicide.
Using aggregated data on deaths for the period 1996–2000, and using population data for 1996, age standardized mortality rates (for the causes listed above) were calculated for the mentally ill and the total populations of the ACT.
Results
The number of deaths among the mentally ill increased dramatically from 1990 to 1995 (a period of continuing development of the system) but then leveled out.
Results are reported for the period 1996–2000.
A total of 19 059 persons were recorded as having contacted the MHS between 1985 and 2000. In 1996 the mentally ill population of the ACT was 16030 (see Table 1), and the total population of the ACT (the total population) was 237 798. Relative to the total population the mentally ill population included more females, more persons aged < 35 years (55.6% cf 45.6%) and < 45 (77.2% cf 65.1%), and only about half as many persons aged 65 years or more.
Characteristics of (a) the mentally ill population and the total population of the ACT in 1996, and of (b) persons who died from all causes and (c) of persons who died from suicide in the mentally ill population and in the general population of the ACT from 1996 to 2000
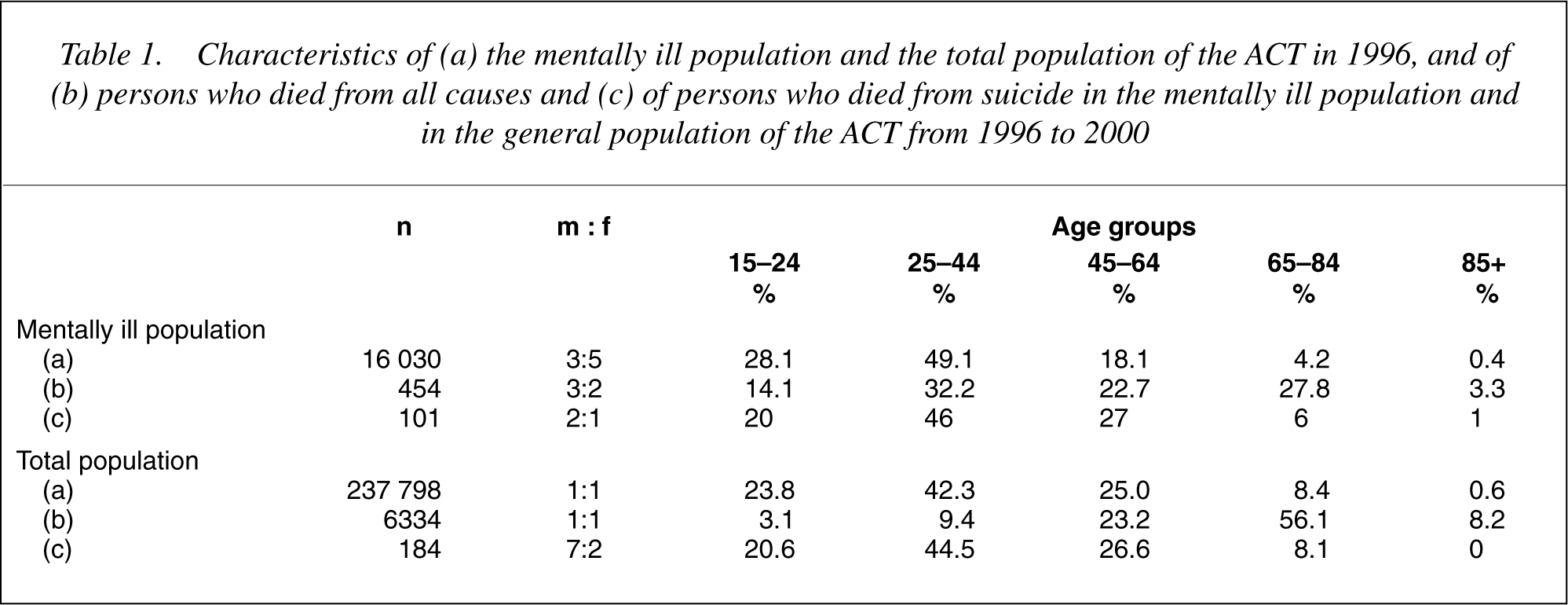
There were 454 deaths (deaths from all causes) reported in the mentally ill (see Table 1), of which almost a third (145) occurred outside of the ACT. The numbers per year were less in 1996–1998 than in 1999–2000. The male: female (m: f) ratio (3:2), and the age distribution, did not vary significantly over the period. There were 6334 deaths reported in the total population (see Table 1), there being no significant variation from year to year over the period in either the numbers, the m: f ratio (1:1), or the age distribution. The age distribution of deaths in the two populations accentuated the differences present in the populations. In the mentally ill 46.3% of all deaths occurred before age 45 compared with 12.5% for the total population. Comparable figures for persons aged 65+ were 31.1% and 64.3%, respectively. The age standardized mortality rate (ASMR) for all deaths for the period was 48.1 for the mentally ill population and 44.7 for the total population. The rate for the mentally ill was 1.08 times that of the total population. These figures were 46.0, 35.5, and 1.30, respectively, when persons aged 85 or more are excluded.
There were 48 deaths from ischaemic heart disease in the mentally ill (ASMR = 7.7) compared with 1350 in the total population (ASMR = 5.6).
There were 101 deaths from suicide (including 41 occurring outside the ACT) in the mentally ill (ASMR = 10.3) and 184 deaths from suicide in the total population (ASMR = 0.9) (see Table 1). The numbers per year were variable but there was no time trend. The rate for the mentally ill was 11.4 times that of the total population.
Discussion
This study did not confirm the findings, reported by Lawrence et al. [2], of a grossly excessive mortality for deaths from all causes and for ischaemic heart disease among the mentally ill. In the ACT (for the period 1996–2000) the mortality rates for deaths from all causes and for ischaemic heart disease in the mentally ill population (including deaths occurring outside of the ACT) were found to be only marginally greater than those of the general population. However, in the ACT as in WA, there was a great excess of deaths in the mentally ill from suicide (even when those deaths occurring outside of the ACT are excluded).
The disparity in the results from WA and the ACT was not expected. However results of other mortality studies in the mentally ill also show considerable variation. Baxter [3] reported the results of nine previous studies, in which excess mortality varied between 1.6 and 7.5. There was also variability in reported excess mortality in the results of more recent population studies by Corten et al. [4] (5.05 males & 5.63 females), Baxter [3] (1.65 males & females combined), and Hansen et al. [5] (3.2 males & 2.4 females).
Baxter [3] identified and discussed ‘five potential problems associated with this type of study’: quality of diagnosis; choice of comparator population; completeness of case ascertainment; bias from loss to follow-up; generalisability of results.
But there are many other problems that need to be considered in interpreting the results of studies which use persons registered in a data bank as a proxy for the mentally ill population. Data banks vary in the level of accuracy in recording names and dates of birth (compromising the match with death data and resulting in some duplications), rarely include persons who seek private specialist care or treatment from general practitioners so that no allowance can be made for that large proportion of persons who have a psychiatric illness but seemingly make no contact with mental health services [6], [7], and vary in their inclusiveness (including all people for whom there is even a tenuous contact with the service, only those who make contact and receive a psychiatric diagnosis, or only those who are formally treated for a serious mental illness). The diagnostic categories and the age groups included in data banks vary considerably. Retention criteria vary (people may never be removed from the data bank, or they may be removed five or 10 years after their last contact or when they move out of area). Mortality rates may be calculated for all people on the data bank (the historical cohort method) or only for those people added in the period for which mortality rates are calculated (the inception cohort method) [2].
The disparity in results between the WA and ACT studies is probably explained by three major differences in method. Firstly, the coverage of the data banks differed markedly. The WA data bank included 18.2% of persons aged 0–14 years of age, 5.5% of persons diagnosed with dementia (the excess mortality rate for dementia was 5.5 for males and 7.6 for females), 9.7% of persons with drug/alcohol problems, and 7.2% of persons in general wards because of self-injury. Whereas, in the WA study, 15.4% of persons had no diagnosis registered (suggesting minimal contact) at least a third of the persons in the ACT database had, at most, one significant personal interaction with members of the mental health service. Persons with dementia or drug/ alcohol problems were rarely included as the ACT mental health service does not service these populations, and persons aged 0–14 were excluded from this study.
Secondly, whereas interstate migration was ignored by Lawrence et al. almost a third of the deaths in our mentally ill population occurred outside of the ACT. Interestingly, if the 40% of our deaths from suicide which occurred outside of the ACT are included, our excess mortality rate for suicide (11.4), was greater than that reported by Lawrence et al. (6.7 males, 7.5 females).
Thirdly, we used an historical cohort, determining the mortality rates for the period 1996–2000 for a mentally ill population consisting of all surviving persons registered from 1985 (including people who had been in the system for many years prior to 1985). Because most deaths occur within the first few years after the first contact with mental health services [1–5] (i.e. many deaths would have occurred before 1996) our results significantly underestimated the real mortality rates in our population. By contrast, Lawrence et al. used (preponderantly) an inception cohort and, thus, determined mortality rates only for those persons added to the data system within the period for which mortality rates were calculated. This means that the very long-term mentally ill (first in contact with services prior to 1980) were excluded. This exclusion is important, both because small variations in deaths in the very elderly population (e.g. those over the age of 85 years) have major effects on age standardized mortality rates (as shown in our results), and because concern with mortality in the mentally ill includes concern about their long-term physical health and longevity.
Taken together, the problems outlined above mean that the validity of measuring the size of the excess mortality in the mentally ill using population studies is questionable.
Conclusions
This study did not confirm the excessive mortality rate in the mentally ill reported by Lawrence et al. [2], except for suicide. Whilst the contention that mortality in the mentally ill is increased was not disproved, many methodological issues in using population studies to attempt to measure the size of such a possible increase were identified.
It is proposed that results of all population based mortality studies must be interpreted cautiously – particularly in relation to the evaluation of services, the need for change, and the determination of public policy.
Footnotes
Acknowledgements
Costs of data processing were met by the Private Practice Fund of The Canberra Hospital. I thank the staff of AIHW (especially John Goss) for their assistance.