
Abstract
Although empirical research is limited, researchers and clinicians have repeatedly invoked the construct of control to understand the epistemologically and clinically intriguing illness of anorexia nervosa (AN) [1–4]. This is unsurprising because a ‘control’ theory may unify a plethora of formulations of the illness, be they psychobiological [5], psychodynamic [1], feminist [6], cross-cultural [7], or cognitive [3] in nature. The concept of control also promises to shed light on the outcome of AN [3], [4], [8] but, again, empirical work is lacking.
Control is a complex construct with different levels of abstraction. Generally, eating disordered patients perceived themselves as having less personal control and being controlled by others [9]. Those with bulimic AN and bulimia nervosa exhibited less control than patients with restrictive AN [1], [2], [10]. In contrast, eating-disordered patients maintained similar or even more control than normal individuals in ‘uninfected’ areas. They also had more ‘negative control’ mechanisms – being overcontrolling on one hand and letting go of control too easily on the other [11].
Existing locus of control scales did not accommodate the complex nature of control [12] and failed to distinguish eating disorders from other psychopathologies [9], [13], [14]. Likewise, rating scales about eating disorders have focused principally on weight control. A potentially useful tool that captures the multidimensional construct of control is the Shapiro Control Inventory (SCI). The SCI has been used in normative, medical and psychiatric populations with satisfactory reliability and validity [15–17].
The present study used the SCI to examine the relationship between control and the intermediate term outcome of Chinese patients with typical and atypical AN in Hong Kong.
Method
Subjects
A consecutive number of 88 female Chinese AN patients who had received treatment at the psychiatric and eating disorders clinic of a university-affiliated general hospital in Hong Kong were contacted from January 2000 to June 2001. This contact was made at an average period of 9.0 years after the onset of illness. The latter was defined as the point in time when patients exhibited weight loss of 15% or more of the expected weight and the absence of three consecutive menstrual cycles. Since 3 patients died, and 11 patients did not complete all rating scales, 74 (restrictive, n = 51 and bulimic, n = 23) patients were studied. Their mean age at the onset of illness, clinical presentation, and time of this study was 18.1 (SD = 3.9), 20.4 (SD 5.4), and 27.0 (SD = 6.9) years, respectively. Their mean body mass index was 19.6 (SD = 2.4) kg/m2 before the onset of illness and 14.6 (SD = 1.9) kg/m2 at clinical presentation. The general outcome findings of these patients were reported separately [18].
Patients had been diagnosed as typical AN (n = 56) or atypical AN (n = 18) according to DSM III-R criteria [19] by an eating disorder specialist (SL). The interrater reliability (kappa for agreement) for the Structured Clinical Interview for DSM-III-R [20] between him and the research assistant (YYLC) was 0.90. Atypical AN patients differed from typical patients by attributing their poor intake to reasons other than the fear of fatness, such as stomach bloating, but resembled typical patients in terms of other diagnostic features [21].
Instruments
The outcome of AN was assessed with the Chinese version of the Morgan–Russell Outcome Assessment Schedule (MROAS) [22] with a high level of interrater reliability (kappa for agreement = 0.99, SL and YYLC). Patients were grouped into three Morgan–Russell categories (MRC) according to their nutritional status, menstrual function, mental status, sexual adjustment and socio-economic status: good (MROAS scores < 8 and ≤12), intermediate (MROAS scores < 4 and ≤ 8), and poor (MROAS scores = 0–4) outcome.
The SCI consists of 187 self-report items and 9 scales that measure domain-general and domain-specific perceived control, positive and negative control mechanisms, and motivation for control [15]. Scale 1 reflects an overall domain-general sense of control. It is obtained by combining Scale 2 (positive sense of control), which measures perceived self-efficacy and self-control, and Scale 3 (negative sense of control), which measures loss of control, feelings of passivity and helplessness. Scale 4 examines an overall domain-specific sense of control according to 7 domains of experience. The latter include body, mind, interpersonal relationships, self, career, environment, and other impulses (e.g. drug and alcohol consumption, smoking, violent behaviour, gambling and time management). Scales 5–8 capture ‘modes of control’ that refer to the cognitive and/or behavioural styles of attaining and maintaining a sense of control. They are presented in two positive and two negative modes, namely, Scale 5 (positive assertive – taking active control), Scale 6 (positive yielding – letting go of active control), Scale 7 (negative assertive – having excessive active control) and Scale 8 (negative yielding – having insufficient active control). Finally, Scale 9 examines the general desire for control. The SCI was translated (by SL and LKGH) into Chinese, pilot tested among 6 patients with AN, and revised until it exhibited reasonable face validity. It is scored using a 7-point Likert scale for Scales 1, 2, 3 and 9, a 6-point Likert scale for Scale 4, and a 4-point Likert scale for Scales 5–8.
Statistical analysis
Simple t-test and ANOVA were used to compare control profiles in two-group and multiple-group comparisons, respectively. Post-hoc Bonferroni t-test was applied to delineate group differences. All p-values were two-tailed. The reliability and validity of the SCI were examined by computing the Cronbach alphas and Pearson correlation coefficients among its scales and with the control-related subscales of the Chinese Eating Disorder Inventory-I (EDI-I) [23], [24].
Results
Reliability and validity
The mean Cronbach's alpha of the 9 scales was 0.83 (range: 0.71–0.91), being highest for Scale 5 and lowest for Scale 8 (15]. Apart from an expectedly high correlation between Scales 1 and 2 (r = 0.93, p < 0.001), the interscale correlations were small (Scale 4 and 9, r = −0.24, p = 0.037) to moderate (Scales 1 and 3, r = −0.79, p < 0.001) and in expected directions.
Internal consistency of SCI scales and their correlation matrix
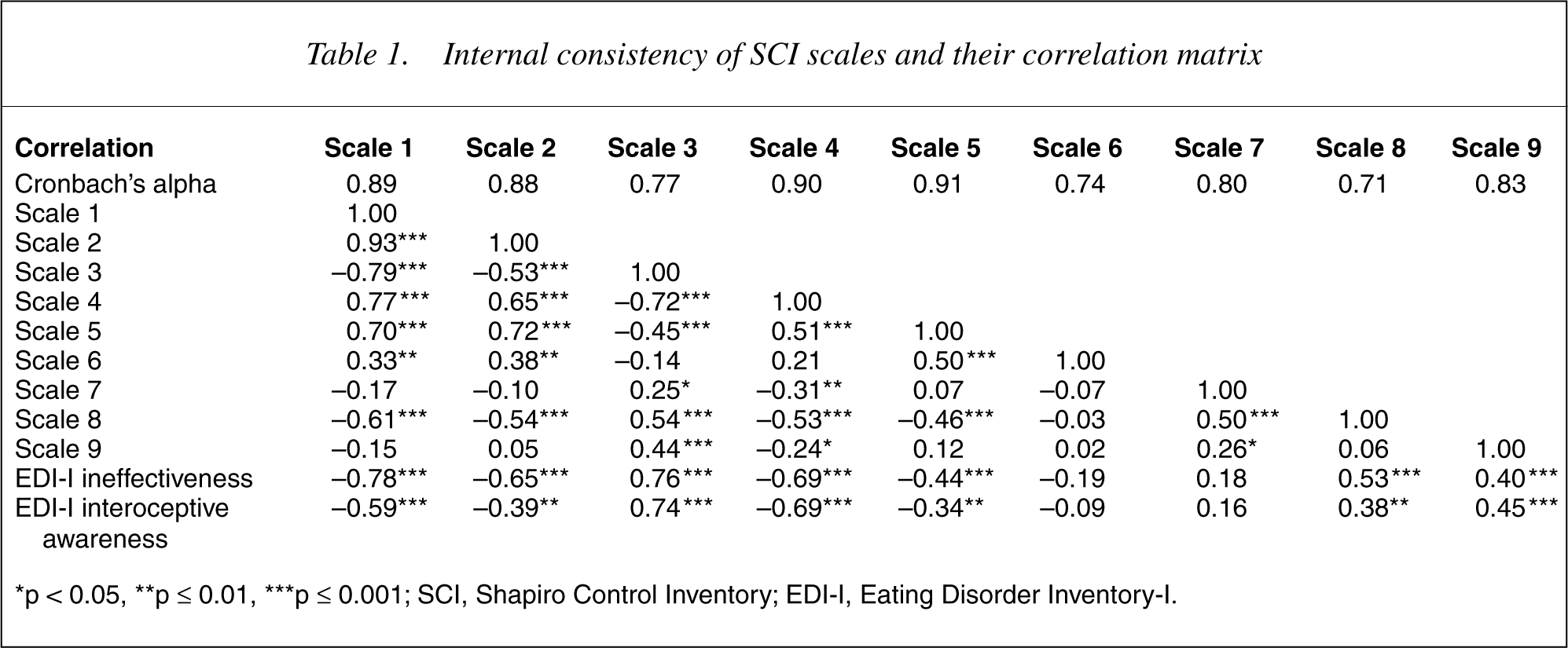
∗p < 0.05, ∗∗p ≤ 0.01, ∗∗∗p ≤ 0.001; SCI, Shapiro Control Inventory; EDI-I, Eating Disorder Inventory-I.
The ineffectiveness (reflecting feelings of deficient control and worthlessness) and interoceptive awareness (reflecting inadequate control of affective and bodily functions) subscales of the EDI-I were significantly correlated with six SCI scales in expected directions. They were negatively correlated with Scales 1, 2, 4 and 5 (rs = −0.44 to −0.78 and rs = −0.34 to −0.69, respectively), and positively correlated with Scales 3, 8 and 9 (rs = 0.40–0.76 and rs = 0.38–0.74, respectively). Their correlations with Scales 6 and 7 were non-significant.
Relationship of control and eating disorders outcome
Overall sense of control
62.2% (n = 46), 32.9% (n = 24) and 5.3% (n = 4) of the 74 patients had good, intermediate, and poor outcome, respectively [18]. The three outcome groups differed significantly on all the four SCI scales that measured sense of control in expected directions (F = 3.86–13.78, df = 2,71, p-values range = 0.001–0.026) (Table 2). The good outcome group reported a significantly higher score than the intermediate and/or poor outcome groups in overall sense of control (Scale 1), positive sense of control (Scale 2) and overall domain-specific sense of control (Scale 4). In contrast, the good outcome group reported a significantly lower score than the other groups in negative sense of control (Scale 3).
Comparisons of SCI profile of the three outcome groups of patients with anorexia nervosa†
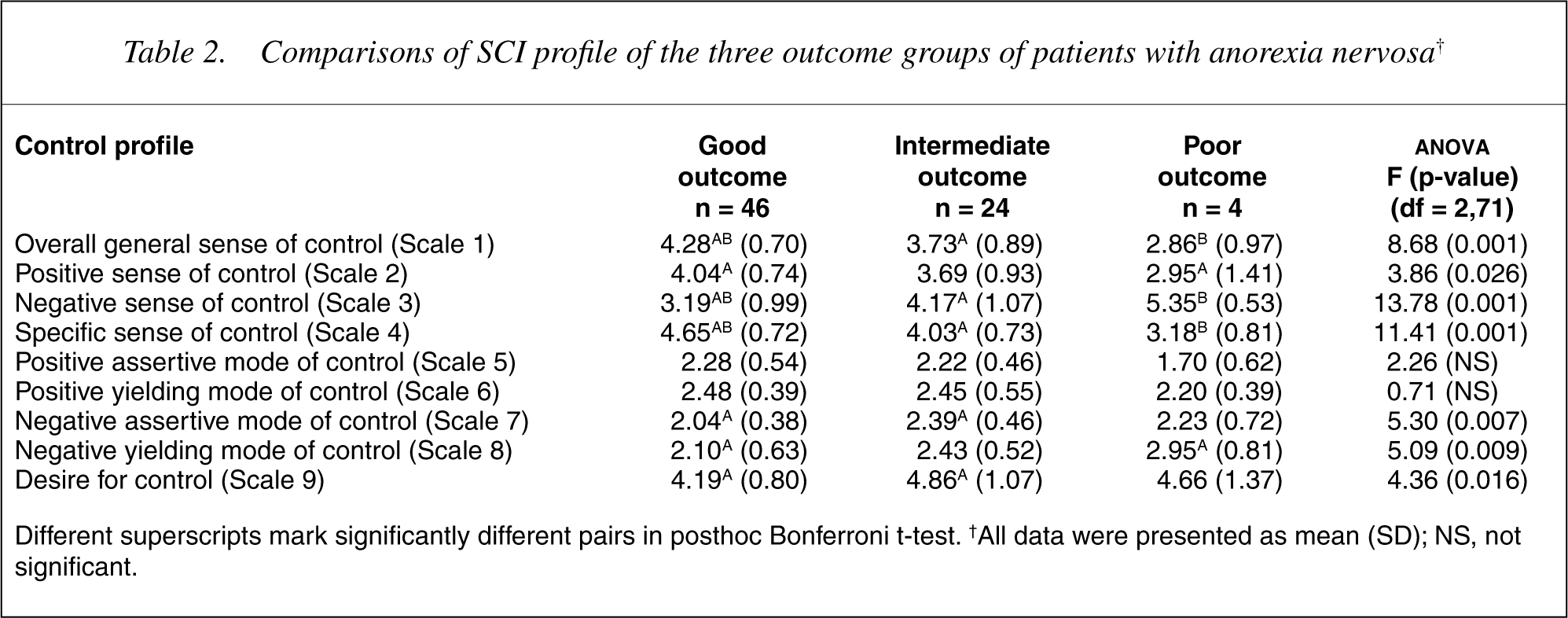
Different superscripts mark significantly different pairs in posthoc Bonferroni t-test. †All data were presented as mean (SD); NS, not significant.
Specific domains of control
Significant group differences were found in five of the seven specific domains, with patients having good outcome reporting significantly higher levels of control than those with intermediate and/or poor outcome. The greatest difference was in the domain of self (F = 15.04, df = 2,70, p < 0.001), followed by interpersonal relationships (F = 11.43, df = 2,71, p < 0.001), body (F = 7.13, df = 2,71, p = 0.002), career (F = 5.03, df = 2,71, p = 0.009), and mind (F = 4.90, df = 2,71, p = 0.01).
Modes of control and motivation for control
The three outcome groups exhibited significant differences in negative assertive (Scale 7) (F = 5.03, df = 2,71, p = 0.007) and negative yielding (Scale 8) (F = 5.09, df = 2,71, p = 0.009) modes of control. Being the lowest scorers on both Scales 7 and 8, patients with good outcome were significantly less negatively assertive than those with intermediate outcome. They were also significantly less negatively yielding than those with poor outcome. The three groups had significantly different scores on Scale 9 (F = 4.36, df = 2,71, p = 0.016), with patients of the intermediate outcome group reporting the strongest motivation to attain and maintain control.
Typicality of AN and control
No difference was found between typical and atypical AN patients with respect to sense of control and mode of control. The two groups only differed significantly in two specific domains, namely, body and mind, and with respect to the desire for control (Scale 9). Typical patients reported a significantly lower sense of control in the domains of body (t = −2.18, df = 72, p = 0.033) and mind (t = −2.14, df = 72, p = 0.036), and a significantly stronger desire for control (t = 2.52, df = 72, p = 0.014) than atypical AN patients.
Discussion
The high reliability coefficient of each SCI scale and the satisfactory correlation matrix supported the reliability and validity of the SCI for determining the multidimensional nature of control in Chinese AN patients. The convergent validity of the SCI was supported by the meaningful correlations of some of its scales with the EDI-I subscales that measured control related phenomena. The non-significant correlation of Scales 6 and 7 with the EDI-I subscales added to the divergent validity of the SCI because they measured additional dimensions of control that were not examined in the control-related EDI-I subscales. The differentiating power of Scales 1–4 and 7–9 among the 3 outcome groups demonstrated the sensitivity of the SCI in measuring sense of control in AN patients.
This preliminary study had several limitations that called for further research. First, it was correlational and did not ascertain whether healthier control was the cause or effect of better outcome in AN [2], [15]. Second, the relatively small sample number could have precluded other meaningful statistical differences from being found. Third, since the study compared control across groups of AN patients with different outcomes, it did not confirm that problems of control were specific to eating disorders. Finally, because the SCI is relatively lengthy, its simplification and further exploration using a prospective design and a larger sample of patients with both AN and other psychiatric disorders including bulimia nervosa will help bridge the empirical gap between theories of control and eating disorders.
With these caveats, our findings provided empirical support for the view that, compared to normal or recovered individuals, AN patients were less assertive, less able to take control of their life, and more likely to perceive themselves to be controlled by others [3], [8], [9], [11], [14]. The consistent differences in the nature, sense, and mode of control among the three outcome groups suggested that control may mediate the mechanisms of the anorexic illness.
Patients with good outcome reported the highest level of overall domain-general, positive and domain-specific sense of control. This tallied with studies showing that a higher level of control was associated with better physical and psychological health in people with medical illnesses [12], [14], [16]. That the greatest discrepancy occurred in the negative sense of control (Scale 3) indicated that a strong sense of loss of control over self or environment, helplessness, and passivity could be useful indicators of poor outcome in AN.
The relationship between control and anorexic outcome was not linear. Thus, patients with good outcome exhibited the lowest level of negative assertive (having excessive active control) and negative yielding (having insufficient active control) modes of control, and the least desire for control. Those with intermediate outcome exhibited the highest negative assertive mode of control and the most desire for control, whereas patients with poor outcome demonstrated the highest negative yielding mode of control and an intermediate desire for control. Prospective research is needed to delineate how an examination of SCI profiles can shed light on the course and outcome of AN.
Our findings may have relevance for the treatment of AN. Experienced clinicians have long recognized that anorexic patients' readiness to let go of pathological control and not imposing excessive control on them is crucial to treatment success [1]. Modern treatment methods, such as cognitive behavioural and motivation enhancement therapy, present patients with alternative evidence and/or re-motivate them to recover by mastering self-control over both eating and noneating related domains of their lives [3], [25].
The concept of control may help resolve controversies over the ontology of anorexia nervosa. Historical and cross-cultural researchers have suggested that an intense fear of fatness, which is a mandatory diagnostic feature of contemporary AN, is not essential to the illness. Patients without such a fear used rationales such as gastric bloating, no hunger, or fear of food to explain food refusal, but resembled typical AN patients in terms of rigid control of food intake, amenorrhea, and general psychopathology [21]. Our findings indicated that typical and atypical AN patients differed from one another with regard to the body and mind domains of control and the desire for control. Such differences might explain the smaller tendency of atypical AN patients to develop bulimic dyscontrol over time [18]. On the other hand, the largely similar control profiles of the two forms of AN indicated their resemblance when they are reconceptualized using the construct of control. In this regard, Katzman and Lee suggested that ‘no-control phobia’ could substitute ‘fat phobia’ during the psychological treatment of both typical and atypical AN patients [7]. This alternative mode of understanding AN may contribute to the development of a culture-flexible formulation of AN that is clinically applicable across different contexts.
Footnotes
Acknowledgements
This study was supported by a grant from the Research Grant Council, Hong Kong (CUHK4029/98L).