
Abstract
Definition and key features
What is schizophrenia?
Schizophrenia, like most psychiatric diagnoses, is a purely descriptive term for the clinical phenotype of a heterogeneous group of psychotic disorders, which result from a substantial disturbance in brain function and also (in at least some cases) more subtly, brain structure. The causes remain unclear. Despite controversy and limited research progress, the term has persisted tenaciously over the past hundred years, originating from the Kraepelinian concept of dementia praecox. This origin created the principal flaw in the concept, namely the intermingling and confusion of diagnosis and prognosis. After some earlier debate, the current DSM-IV definition of the syndrome attempts as did Kraepelin to capture a group of psychoses with a uniformly poor prognosis. This is an impossible task on the basis of clinical features alone, as Kraepelin himself discovered, and the course of schizophrenia has turned out to be heterogeneous and strikingly different from its prototype, Alzheimer's dementia [1], [2]. Schizophrenia now refers to a group of disorders characterized by positive psychotic symptoms at some stage of illness, where mania and major depression are not prominent or persistent features, and where negative and cognitive symptoms are likely to be prominent and associated with a variable level of disability. Comorbidity is extremely common yet frequently overlooked. The boundaries of this artificially constructed entity with normality [3] and with other major psychiatric disorders [4] are naturally blurred. It provides an excellent example in psychiatry of the need to re-evaluate clinical phenotypes for both clinical and research purposes [5]. Despite this, the schizophrenia concept has found a way to persist, because so far no superior candidate has been found to replace it. Nevertheless, its flaws continue to impede treatment and the interpretation and conduct of research, and should be kept firmly in mind.
How common is schizophrenia?
Schizophrenia has a lifetime prevalence of approximately 1% [6]. The recent low prevalence study in Australia suggests that the prevalence of psychotic patients in treatment in a one-month period is 4.7 per 1000 [7]. However, the total prevalence may be significantly higher, if currently untreated and never treated cases were more completely ascertained [8]. Prevalence rates also increase in relation to the degree of urbanization and social disadvantage [3], [9], [10]. It has recently become clear, after decades of debate, that the incidence (as well as the prevalence) is higher in males and in disadvantaged communities [11], [12]. The prevalence in indigenous communities is unknown but elevated rates of hospitalization, as well as pervasive social disadvantage affecting indigenous communities provide indirect evidence that the prevalence rate may be higher than in the wider society. (According to the Australian Institute of Health and Welfare Hospital Morbidity Database for 1998–1999, standardised morbidity ratios were 1.8 and 2.0 for indigenous versus non-indigenous males and females respectively for the ICD-10 diagnoses of schizophrenia, schizotypal and delusional disorders.)
Cost of schizophrenia
The SANE/Access Economics report into the economic costs of schizophrenia in Australia [13] showed that the annual direct costs of schizophrenia were $661 million, or $18 000 per person with schizophrenia. Indirect costs were calculated to be $722 million. The report also estimated the transfer costs of the illness, which included $190 million of lost tax revenue of patients and carers and $274 million in welfare payments. Thus the total economic cost to Australia in 2001 of schizophrenia was $1.85 billion. Forward projections indicate that, by 2001, the direct cost of schizophrenia will be over one billion dollars annually. This will probably be an underestimate as new (and presumably more expensive) medications become available. The direct costs, while substantial, remain well below what is expended in other developed countries, and, arguably, what is genuinely required for optimal care [14]. It is heavily skewed towards acute care, though even this has come under extreme pressure and reveals increasingly unacceptable quality. The avertable burden, although claimed to be less than in other disorders [15], could be still be substantially addressed with improved coverage and quality of care. The avertable but currently nonaverted burden may well be much greater than has been estimated; better research on this question is urgently required [16], [17].
Clinical presentation
Symptoms of schizophrenia represent the consequences of disordered cognition and emotion. These manifest as disturbances in language, thought, perception, affect and sense of self. Symptoms are typically divided into two main syndromes, known as positive and negative symptoms because of the clinical appeal of this distinction. Positive symptoms include hallucinations and delusions. Negative symptoms include the loss of initiative, social, personal or sexual interests, anhedonia, and blunted or inappropriate emotions. Negative symptoms even occur when the more dramatic positive symptoms are in remission, though they may be secondary to other factors, such as depression. A third syndrome, disorganization, features disorganized thought, speech and behaviour. All three syndromes are seen in other psychotic disorders, including psychotic mood disorders, and despite earlier views, there are no pathognomonic features of schizophrenia as it is currently defined. It is a polythetic construct built up through a variable blend of symptoms and disability. Comorbid mood, anxiety, substance use, and personality disorders are extremely common and require a therapeutic response.
Schizophrenia cannot be diagnosed without the presence at some stage of positive symptoms. However, many see it as predominantly a disorder of cognition, with neurocognitive deficits featuring prominently and strongly influencing functional recovery [18], [19]. A fundamental conceptual problem with schizophrenia has been the confounding since the time of Kraepelin of clinical syndrome with course of illness. The term has thus been skewed towards the treatment-resistant and poor outcome subset of psychotic patients. Current diagnostic criteria uphold this tradition, hence clinical trial data underestimate the efficacy of treatment for the full spectrum of cases. This diagnostic artefact continues to fuel therapeutic nihilism and perpetuates the myth, actively nurtured by some in the present era, that schizophrenia is more or less untreatable [15].
Diagnosis is complicated in cross-cultural settings. For instance, in Aboriginal and Torres Strait Islander populations positive symptoms must be differentiated from certain culturally informed experiences and negative symptoms from the corrosive effects of unrelenting social disadvantage, which is often complicated by substance use. These difficulties are compounded by miscommunication, emphasizing the importance of informed indigenous collateral informants.
Course of illness
Schizophrenia is a syndrome with a highly variable presentation and course [2]. DSM-IV criteria require 6 months of continuous symptoms, including an active phase with at least 1 week of psychotic symptoms. Not seen in other definitions, this duration criterion censors the schizophrenia concept in a chronic direction and hampers early intervention. One architect of the DSM definition has proposed the removal of the 6 month criterion [20]. The ICD-10 definition conflates both DSM IV categories of schizophreniform disorder and schizophrenia since it requires a duration of only 1 month and is more useful on these grounds.
The active (positive symptom) phase is usually preceded by a prodromal phase in which there is clear deterioration from previous functioning, including social withdrawal, impairment in role functioning, and a range of low grade positive and negative symptoms. The duration of this phase is extremely variable, and its onset may be difficult to date accurately, especially when there is a slow insidious onset over several years, which is often confused with ‘premorbid personality’. Much of the loss of function in social, academic and occupational roles emerges during the prodromal phase of the illness prior to onset of diagnostic specific frank psychotic features [21]. Ultimately, it may be possible to engage and treat a proportion of people during the prodromal phase before they became frankly psychotic. However, methods of prediction need to be improved to reduce the number of false positives [22]. A greater capacity to engage and treat young people in this phase also needs to be developed. Engagement during a potential prodrome allows for early engagement, building of rapport with clinicians and trust in the health system prior to a crisis or full loss of contact with reality, all of which is likely to lead to less traumatic and better tolerated intervention, even if frank psychosis does ensue. Delay or reduction of risk of transition may also be possible [23–25] and underlying neurobiological changes averted [26].
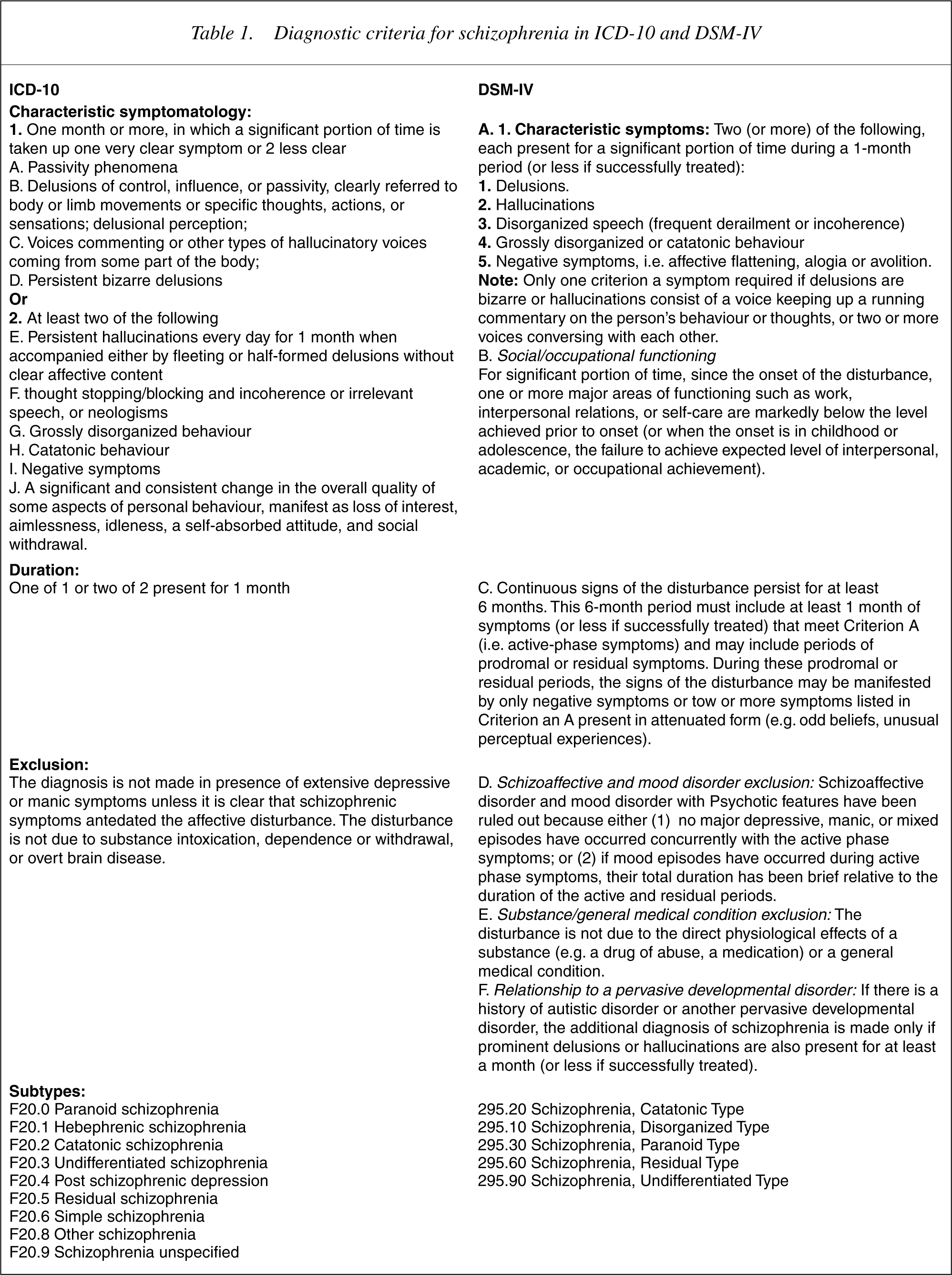
Psychotic symptoms required for diagnosis are noted in criterion A of the diagnostic criteria (Table 1 DSM [27] and ICD [28] diagnostic criteria).
Diagnostic criteria for schizophrenia in ICD-10 and DSM-IV
Psychosocial stressors may occur before the onset of an initial or recurring episode of psychosis. Duration of the active phase varies. People often have active psychosis for a prolonged period (average of over 12 months even in developed countries) before seeking and obtaining help [29]. A longer duration of untreated psychosis (DUP) is related to poorer outcome [30]. Because of the collateral psychosocial damage during this period of delay, and the possibility that neurobiological changes are actively occurring [26], people with psychosis need to be identified and treated as promptly as possible after the onset of frank psychotic symptoms. Treatment of the first episode results in full or partial symptom remission in up to 90% of cases and hence is highly effective [31–33].
A residual or stable phase often follows the acute and stabilization phases. Features of this phase resemble the prodrome, however, affective blunting or flattening and impairment in role functioning is more common. Some psychotic symptoms, such as delusions or hallucinations, may persist, but their intensity attenuates. Residual symptoms may also attenuate over time. A typical course is a pattern of acute exacerbation, possibly precipitated by stress, illicit drug use, non-compliance with maintenance treatment, or some combination of these, with residual impairment between episodes. However, the degree and quality of intervention tempers this substantially. Unfortunately, real world problems, notably inadequate service quality and resources, adherence problems and poorly treated comorbidity, cause the effectiveness of interventions to fall well short of their potential efficacy [7].
Early functional disability tends to stabilize within 2 years [2]. Rates for longer-term remission are controversial, with large variation in outcome. Approximately 50% of people with a first episode of ICD schizophrenia are in fact socially recovered 5 years later [2]. However for a subgroup of patients, complications and global impairment do increase between episodes during the initial years [34–36]. Delayed and inadequate treatment is a malleable variable responsible for a quarter of the explainable outcome variance in the early years after diagnosis [37]. This has supported early detection and engagement [38], [39], even though DUP may be partly confounded with other predictors [29], [37]. Finally, quality of treatment exerts a very positive impact on short-term outcome [40–43], particularly if the full range of patients with schizophrenia and not merely multiepisode and treatment resistant samples are studied [44]. Treatment quality means addressing all the health needs of patient and family, such as depression, suicide risk, substance use, smoking, general medical care, family needs, vocational recovery, stigma and social relationships. Evidence demonstrates that the Kraepelinian premise that schizophrenia is inevitably a deteriorating illness, which intervention will do little to curb, was never really true [45], [46] and is today less tenable than ever.
Violence
Violent acts performed by people with schizophrenia often attract disproportionate public attention. Wallace et al. have found that while they (particularly males) commit more violent offences than matched controls, the rate of increase of these acts has been consistent with that in the general community [47]. However, a subset of patients do manifest an increased risk under certain conditions [48]. This is not an intrinsic feature of the illness, though some symptoms patterns pose more risk. The combination of untreated or poorly treated positive symptoms and substance abuse is a major and reversible contributor. This highlights the scope for preventing violence in schizophrenia as well as the consequences of the deficiencies in continuing community care and the limitations of our predominant focus on acute care.
Comorbidity with substance abuse
Rates of drug and alcohol abuse are higher in people with schizophrenia than the general population. A review of the evidence regarding management of such comorbidity is beyond the scope of this guideline. However, substance use in patients with schizophrenia, particularly its role in onset and in precipitating relapse or exacerbation, should be a specific area of attention in assessment and treatment.
Mortality and physical morbidity
The life expectancy of people with schizophrenia is shorter than that of the general population because of an increased rate of completed suicide (approximately 10%, mostly in the early years post diagnosis) and premature death from various medical causes. With better treatment this mortality could be reduced. Medical care for people with schizophrenia is poor even with mainstreaming of mental health services [49–52].
Indigenous and ethnic perspectives
The past two decades have seen increased awareness of ethnicity and culture in mental health services. In both New Zealand (Mäori) and Australia (Aboriginal) the perspectives of indigenous peoples as well as migrants have been important for clinical services, not only because those peoples are often over-represented, but also because outcomes are frequently worse than for the general patient population. Clinicians should therefore be mindful of the impact of cultural difference and indigeneity in terms of the broad understandings of health and sickness, assessment, clinical presentations and treatment.
Aetiology
Schizophrenia is a complex syndrome which overlaps with other psychotic disorders phenotypically and in terms of underlying risk factors and biomarkers. It probably arises from a combination of risk factors, mainly in genetically vulnerable people. The genetic vulnerability is complex and is now regarded as involving a variable combination of multiple genes of small effect. Genetic risk as expressed through family history is the most potent individual risk factor but has a much lower population attributable risk, so sporadic cases are very common. Some risk factors may operate early in life, for example, during the perinatal period, creating a state of neurodevelopmental vulnerability. Until recently this was thought to be sufficient for later onset, which would emerge after a long latent period – the so-called ‘doomed from the womb’ notion. Increasingly however, it is becoming clearer that additional risk factors and pathophysiological processes operating closer to the onset of the syndrome are probably required. This has been termed the second ‘hit’ (or ‘hits’) model, linked to onset of the clinical disorder. The first set of risk-factors includes perinatal birth complications and intrauterine viral infections. The second set putatively involves either endogenous CNS processes, operating late in the neurodevelopmental cycle, such as increased neuronal or glial dysfunction with reduced connectivity and a subtle increase in the loss of neuropil, and/or extrinsic factors such as substance abuse, viral infections and developmental stress. How specific these putative risk factors are for subtypes of serious mental disorder is not clear. Further, how necessary and/or sufficient specific vulnerabilities and causal risk factors may be in the aetiological mix remains totally unclear. With advances in neuroscience, there is now extensive evidence of mild structural and significant functional abnormalities in the CNS of people with schizophrenia, though it is safe to state that none are specific to schizophrenia. While they confirm that schizophrenia is associated with brain dysfunction and can be therefore be regarded as a brain disease, there is still no laboratory test to confirm the diagnosis of schizophrenia.
Other replicable risk markers include gender and urban birth. Women tend to develop schizophrenia 3–4 years later on average than men and the risk is almost double for men during the peak period of onset. Women do show a second peak of onset around menopause, however, it is questionable whether the total incidence is truly equal over the lifespan, as traditionally believed [11], [53]. More women than men experience late-onset schizophrenia. Oestrogen is hypothesized to raise the vulnerability threshold in women until menopause, and may ameliorate the symptomatology in acute episodes [54–58].
Schizophrenia is more common in the lower socioeconomic strata. The reasons are unclear, but at least partially involve downward social drift, lack of upward socioeconomic mobility, and high stress. However, there is some important recent evidence that urban birth and socioeconomic disadvantage are associated with an increased risk [10], [59].
Method
This guideline was developed as part of the Royal Australian and New Zealand College of Psychiatrists (RANZCP) Clinical Practices Guidelines (CPG) Project. The overarching development process has been described [60]. The schizophrenia CPG team were clinical and research experts from psychiatry, clinical psychology, psychiatric nursing and epidemiology drawn from across Australia and New Zealand. The team also drew extensively upon the experience of consumers and carers for review and input and consulted with international experts and guideline teams.
The development process
The development of the guidelines was guided by the process detailed in the ‘APA Practice Guideline Development Process’ (available from the American Psychiatric Association Office of Research). Key features of the process included the following:
A comprehensive literature review, automated and hand searching methods 1990–2004. Key foci involved scrutiny of all Cochrane reviews (up until 2004 – i.e until the final revision of this document), all recent review articles (1995–2004), and the Clinical Practice Guidelines produced by the APA [61], the various Scottish Guidelines [62–64], the NICE (National Institute of Clinical Excellence) guidelines [65], the Canadian Guidelines [66], and various others, including the draft PORT (Patient Outcomes Review Team) update (Anthony Lehman, personal communication 2003). Production of multiple drafts reviewed by the CPG team and incorporating comments submitted by individuals and groups through the national consultation process. Dissemination and review of drafts. Consumer and carer involvement and review was sought through advertisements in carer and consumer publications. Commentaries were received via facsimile, E-mail, letter or telephone interview. Consumer and carer representatives were included in the development team.
Evidence was assessed and graded according to the convention reported in Boyce et al. [60].
Current treatment evidence
Schizophrenia is treated in a particular context with a range of interventions, and which can be usefully characterized by stages [39],[67–69]. Four stages, which cover the whole course of the illness, can be defined. These are the prepsychotic or prodromal phase, first episode psychosis, the recovery phase and prolonged or persistent schizophrenia. The treatment evidence is presented in two ways. The first section deals with the context and content of interventions in general. The second section deals with the evidence for treatment according to stage of the illness. Finally, the CPG reviews the evidence and offers guidelines for responding to treatment refractory schizophrenia and acute psychotic emergencies.
Fundamental guideline: the therapeutic role of optimism
In the UK the first clinical guideline in the recently published guidelines on schizophrenia from the National Institute of Clinical Excellence (NICE) is:
Health professionals should work in partnership with users and carers, offering help, treatment and care in an atmosphere of hope and optimism [65].
The authors have recognized that the very first step in improving the quality of treatment for schizophrenia is stemming the tide of therapeutic nihilism which still flows far too strongly, with iatrogenic consequences. Evidence-based optimism is one obvious strategy and these guidelines document current evidence-based knowledge and recommendations. The degree of consensus across the various guidelines produced in the developed world in recent years is both striking and reassuring, not only concerning the need for optimism, but across the entire range of recommendations.
Section 1: the context, structure and content of intervention
The service system and models of intervention
Following a decade of reform, the service system has been transformed to a substantial yet variable degree from stand-alone psychiatric hospitals to a system of community-based care with many fewer inpatient beds than other developed countries, and a relatively stronger, but still inadequate, community-orientated psychiatric system. There are several components of this new model of care, only some of which have been evaluated [70]. These generally include:
Community mental health or continuing care teams which provide case management to a subset of patients with schizophrenia; Assertive community treatment teams (ACT) which provide mobile intensive case management to a more complex subset of patients; Crisis teams or community assessment and treatment teams (CATT) which provide acute phase community based assessment and treatment; Acute inpatient units; Subacute inpatient care for treatment-resistant patients; Intensively supervised community-based clinical care residential units; A range of NGO (non-government organization) residential and day care facilities; Primary care; and Private specialist psychiatric care.
The effect on practice of this still incomplete wave of reform has been profound, yet very little health services research has been carried out to assess the impact on patients and families. For schizophrenia, the main disorder targeted by these reforms, the results do not look particularly positive so far in that most people with schizophrenia remain marginalized with a poor quality of life, and are receiving suboptimal treatment [7], [14]. Accessing public services is extremely difficult [71], [72], while one study found that only 7.5% of people with schizophrenia used private inpatient facilities in 2001, and only 13.5% had private health insurance (compared to a national average of 32%) [13]. Only a quarter of people with schizophrenia accessed private psychiatrists [13]. Guidelines based on evidence and experience are as follows.
Guidelines
Assertive community treatment is strongly supported as a model of care. This line of evidence provides support for both the crisis/home treatment model and the intensive mobile case management model of intervention [73], [74]. [I] Early intervention models are supported by a growing evidence base [39], [44],[75–78]. [I] Continuing care teams and case management are a fundamental building block of the system of care. Evidence is inconclusive and the quality of research is suboptimal [79–86]. Assertive case management based on an appropriate skill base, and moderate case loads to enable flexible outreach, is strongly endorsed as a mechanism for better coverage. [III-2] Furthermore, most people with schizophrenia should be provided with secure access to specialist continuing care teams in partnership with general practitioners and private psychiatrists. [V-2] Other elements of the service system have not been adequately evaluated despite a degree of face validity. There are serious questions of quality, resourcing and mutual integration of the various service elements. The location and permeability of the key boundaries, e.g. specialist versus NGO, public versus private, primary versus specialist, child and adolescent versus adult versus aged mental health services have never been evaluated.
Pharmacological interventions
Psychopharmacological treatments form the cornerstone of both acute and maintenance therapy for schizophrenia. Following their introduction in the 1950s, they revolutionized treatment, producing dramatic improvements in short-term outcome. However the first generation of antipsychotic agents proved only partially effective for positive symptoms and they had little impact on or even worsened the negative symptoms and cognitive deficits. In recent decades there has been a worldwide trend for markedly excessive doses to be used both in the acute and maintenance phases, and for them to be also used for behavioural control instead of more targeted use in treating core positive symptoms. This trend has resulted in a great deal of unnecessary suffering. Excessive use of depot antipsychotics as a crude response to the widespread lack of adherence to oral medications has been another unfortunate feature of the landscape of care, especially in Australia. The under-investment in quality systems of care, and the failure to routinely provide intensive and comprehensive psychosocial interventions to complement drug therapies, has resulted in a very limited improvement in functioning and quality of life for patients in the real world. This is abundantly clear in the starkly disappointing findings of the low prevalence study [7].
The emergence of the novel antipsychotic agents in the wake of the renaissance of clozapine has changed this scenario fundamentally. Expectations for recovery and reintegration are now much higher. There is minimal evidence that the novel agents are more efficacious than the conventional antipsychotic medications in the acute treatment of positive symptoms, though they do seem to be more effective in relapse prevention [87]. Furthermore there are data suggesting, but not yet proving, greater efficacy for negative and neurocognitive symptoms [88]. More importantly, novel antipsychotic drugs are much better tolerated and produce fewer motor sideeffects, including tardive dyskinesia – a decisive advantage. This may mean that because patients are more likely to take these medications than the older drugs, their real world effectiveness is much greater [89]. However some of the newer drugs have potentially serious side-effect of their own, especially endocrine and cardiac side-effects, weight gain and impaired glucose tolerance, which will temper especially their long-term use. These effects are of particular concern in Aboriginal and Torres Strait Islander populations where the prevalence of obesity, diabetes and cardiovascular diseases are significantly elevated. Another problem is the tendency for combined use of typical and atypical medications in routine care, which limits the advantages of the latter and magnifies the risk of adverse reactions.
Until recently there had been some debate as to whether conventional or novel antipsychotic drugs should be used as first-line in first episode psychosis or in continuing care of multiepisode patients [90–92]. However, the risk of tardive dyskinesia is higher with the conventional drugs and the levels of extrapyramidal symptoms (EPS) also remain higher even with low dose conventional agents [93–95]. The most definitive meta-analysis to date favours atypicals over typicals on efficacy and tolerability grounds [96], though some authorities remain unconvinced [97], [98].
There still may be a place for conventional antipsychotic drugs when all novel options have been exhausted, especially for the time being, in the minority of cases where depot use can be justified, however, even here longacting atypical agents are now available. In developed countries such as Australia and New Zealand, the better tolerated alternative seems fully justified as first line treatment on clinical and humane grounds despite its higher cost.
Guidelines
Patients and families should be fully informed regarding the benefits and risks of drug therapy and consulted in the choice of antipsychotic agent; interpreters or cultural facilitators should be utilized where necessary. Where it is not possible, such as in many acute episodes, to fully discuss the choice of agent, the oral atypical agents should be the treatment of choice in view of the lower risk of EPS. [V-1] Antipsychotic medication should be prescribed wherever possible in a non-coercive manner in combination with psychosocial interventions including adherence-promoting strategies. [I] Oral atypical medications – risperidone, olanzapine, quetiapine, amisulpride and aripiprazole – should be prescribed as first and second line treatment in first episode psychosis. Initial dosage should be low and increased slowly at spaced intervals only if response is slow or incomplete. Secondary distress, insomnia and agitation should be treated initially with benzodiazepines. Other symptom dimensions such as mania and severe depression require specific treatment with mood stabilizers and antidepressants. [I] Patients currently receiving conventional antipsychotic medications in whom there are persistent positive or negative symptoms, or who are experiencing distressing side-effects, should be switched to oral atypical antipsychotic medication under close specialist supervision. This may be done in the context of an acute relapse or in a stable but not optimally remitted patient. [I] While other reversible causes of relapse need to be considered, patients who relapse despite good adherence to typical antipsychotic medication should be switched to atypical medication. [I] Clozapine should be confidently introduced at the earliest opportunity if evidence of treatment-resistant schizophrenia is present. Treatment refractory schizophrenia is defined as the failure of full remission of positive symptoms or the lack of satisfactory clinical improvement despite sequential use of recommended doses of two or more antipsychotic medications for 6–8 weeks. Treatment refractory schizophrenia may be obvious early in treatment (within 6 months) or emerge later, following a series of episodes. [I] Depot medication should be reserved for two groups. Firstly those who clearly opt voluntarily for this route of administration. Atypical injectable agents are preferred because of better tolerability and reduced risk of tardive dyskinesia. Secondly, those who despite a series of comprehensive psychosocial interventions aimed at promoting adaptation and adherence, repeatedly fail to adhere to necessary medication and relapse frequently. This is more urgent where the consequences of relapse are serious and involve substantial risk to the patient or others. In this second group, depot will be unfortunately utilized within a more coercive model, usually involving involuntary community treatment. However, this should be seen as a temporary model of treatment and be reviewed periodically to assess whether oral therapy can be substituted (subject to patient preference). [V-2] Emergency situations are covered later, but the key principle is to avoid first line use of agents likely to undermine future adherence through the production of aversive subjective side-effects. The immediate aim is not only to reduce aggression, agitation and risk but also to make the patient feel subjectively better and calmer. Typical agents should be used as a last resort in this situation, particularly haloperidol, which stiffens rather than sedates. [V-2] Multiple antipsychotic agents, such as combinations of typical and atypical medications, should not be used except during transitional periods when switching is in progress. [III] Polypharmacy of other kinds, such as combinations of an antipsychotic agent, a mood stabilizer and a benzodiazepine or an antidepressant, may be fully justified by comorbid symptom dimensions, which are extremely common in psychotic disorders. [V-2] Weight and BMI should be measured at the start of treatment, then monthly for 6 months and 3 monthly thereafter. Consultation with a dietician is advisable as is encouragement of regular exercise. Finally it may be necessary to consider a medication with a lower risk of weight gain if this does not respond or is marked. The pros and cons should be discussed with the patient and psycho-social support provided [67]. [V-1] Fasting plasma glucose (or HbA1c) and lipid profile should be measured at baseline and at regular intervals during the course of treatment, along with other investigations as indicated [99].
See Table 2 for a summary of the efficacy of antipsychotic treatment of schizophrenia.
Efficacy of antipsychotic treatment
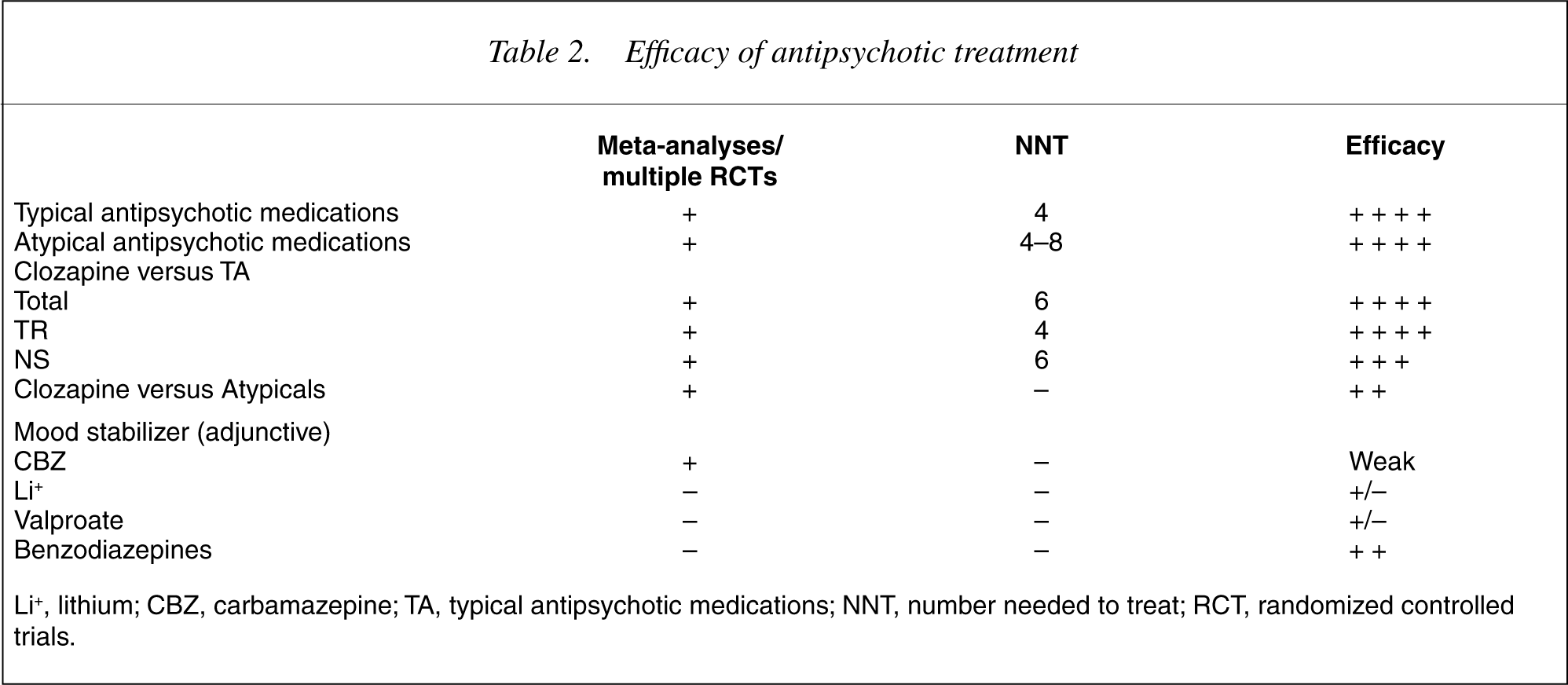
Li+, lithium; CBZ, carbamazepine; TA, typical antipsychotic medications; NNT, number needed to treat; RCT, randomized controlled trials.
Psychosocial interventions
Since the introduction of neuroleptic medication in the 1950s, the mainstay of treatment for schizophrenia has been pharmacotherapy. Prior to that psychoanalytic psychotherapy was regarded as the gold standard [100], though few patients had access to this and most were treated with a combination of crude biological therapies and custodial care. The advent of antipsychotic medication led to greater improvement for a far higher proportion of people than did psychoanalytic intervention. However, while biological interventions revolutionized the treatment of people with schizophrenia, many of these people did not make gains in personal occupational, social or self-care domains of their lives. At the same time, they were increasingly located in the community [101], where they desperately needed the very skills in which they were deficient, and which medication could not hope to fully address. Thus in the 1960s, behavioural interventions emerged, followed by psychoeducation and family interventions. In the last 15 years, cognitive behaviour therapy, cognitive remediation and vocational rehabilitation have been developed and are showing positive results in targeting the symptoms of schizophrenia, as well as addressing the wider psychosocial consequences. It is now accepted that treatment of schizophrenia cannot be a one dimensional biological approach [102], but that for optimal outcome, the psychosocial domain needs to be addressed [103]. Further, despite recent discoveries, when one considers that antipsychotic medications have often been used in a crude and inexpert manner for much of their existence, that they have proved only partially effective, and that they are poorly adhered to in the real world, it becomes obvious why medication is only part of the spectrum of interventions [104], [105].
Guidelines
People with schizophrenia should be provided with psychosocial interventions, relevant to their needs and informed by an understanding of the social and cultural context. [I] When these are provided quality of life and functioning is improved, and there is a positive effect on negative symptoms, readmission rates and recovery levels. [I] Families feel more supported and informed, and better able to look after their relative when offered education, support and appropriate involvement. [V-1] Psychosocial interventions work best in a system not wholly occupied with managing the acute episodes of illness and then discharging people to minimalist care (especially where the GP is the sole clinician). [V-2] Psychosocial intervention will need to be tailored to the individual and phase of illness, and focus on issues of specific relevance to that person. [V-2] Psychosocial interventions require well-trained clinicians with specific expertise. [V-2]
Family interventions
Families, broadly defined, represent the major support system for many patients. They are a vital resource and need to be nurtured as such. Wherever possible and as appropriate, family members and others connected to the person should be involved in the treatment. Families may not only care for their relative, but also inevitably experience substantial psychological and social effects themselves following the onset and during the course of schizophrenia. Families benefit from an intervention that offers knowledge about the illness, its effects on the person with it, and on the family, and provides an avenue of support for them. Families can also help each other. Psychosocial family interventions have a number of aims, including developing an alliance with carers, reducing emotional distress, creating or recreating a positive family atmosphere, problem solving, maintaining realistic expectations of patient performance, helping to set limits and appropriate relationship boundaries.
There are generally three components of family intervention (FI). The first is to build an alliance with the family. This is best done early in the first episode. It is more likely to be successful when support is provided to the family in the acute phase when they usually have a myriad of questions and concerns. Parents and siblings are likely to have different issues. The second component is a relatively structured component that aims to educate the family about the illness. Several studies have found psychoeducational multifamily interventions to be effective. This often needs to be supplemented with individual interventions, specifically designed for each family to address their own set of circumstances. This third component may for example include more specialized family therapy [106].
A Cochrane review [107] of 13 studies of FI in schizophrenia found that it has no effect on mortality, that patients' mental state improves, especially if the level of therapeutic skill is higher, and drop out rates are low, suggesting that FI is an acceptable form of therapy to patients. There are no clear effects in the domain of social functioning, but there are positive trends towards employment and independent living. The effect on families is to reduce the burden of illness, increase knowledge and decrease expressed emotion. FI reduces total costs by about 20%. The Cochrane reviewers found that the number needed to treat (NNT) to produce remission using FI was 6.5. Family therapy has been shown to reduce relapse rates by over 50% compared to medication and case management alone. Another review of 6 RCTs [108] found that FI reduced relapse at 6 and 9 months but not 24 months with a NNT of 2–5. There were also significant effects on expressed emotion and hospital admission but not compliance.
Evidence and recommendations for the use of FI are as follows.
Evidence
FI is effective in reducing relapse [101], [105],[107–109]. [I] FI is effective in reducing problems in families with difficulties [110]. [II] There is evidence that multifamily groups may be better than single family groups [101], [109],[111–116]. [II] Local and national support groups are effective in supporting the family. [III-3]
Recommendations
Psychoeducation
Psychoeducation (PE) programs for people with schizophrenia improve adherence to treatment, and lead to better outcomes, better management of subsequent relapse, lower readmission rates and a greater sense of well being.
Psychoeduction can be conducted separately, but also as part of other interventions such as FI. In the early phases PE tends to focus on supporting and educating the patient or the family about the illness, using a biopsychosocial perspective. As the patient recovers, the subject matter may evolve to more general topics, such as life skills and adapting to the changes necessary to manage their illness.
Information should also be given to others, who although not primary carers, are in contact with the patient. These may include staff of community agencies, local government and supported accommodation residences as well as the general public. The term for this process is mental health literacy (MHL) rather than PE, which incidentally is not a popular term with consumers. MHL should be extended to the whole population [117].
A Cochrane review of PE [118] found that compared to standard care alone, the addition of PE was worthwhile. The number needed to treat (NNT) with PE in addition to standard care was 9. However the recent National Institute for Clinical Excellence guidelines were more equivocal in their evaluation of the evidence, while supporting PE as good clinical practice [65].
Evidence
Recommendation
PE should be offered as a core intervention. [II]
Cognitive interventions
Cognitive behaviour therapy (CBT), developed over the last 50 years for the treatment of non-psychotic disorders, has, in the last 10 years been applied to the treatment of schizophrenia, and has shown very positive results in a number of controlled trials.
A Cochrane review [119] of CBT for schizophrenia found that the average number needed to treat for one person to become symptom free was six. It also found that CBT added to standard care was better at reducing relapse than standard care alone. It is generally believed that those who provide CBT need to be highly skilled. In Australia and New Zealand this would currently mean those who have completed postgraduate training in CBT, or for whom CBT was a central part of their basic training (e.g. clinical psychologists). However a recent study by Turkington et al. has indicated that less highly trained clinicians in real world conditions can also effectively use this approach [120].
Another cognitive intervention, cognitive remediation (also called cognitive rehabilitation) [121], aims to address cognitive impairments, such as distractibility, memory problems, lack of vigilance, attentional deficits, and limitations in planning and decision making. Since these deficits correlate more closely with functioning than do symptom levels, addressing them may enable the patients to be able to engage in and benefit from other interventions, and consequently function better in social and other domains. So far results in controlled trials of cognitive remediation have been equivocal [122].
Evidence
Individual CBT is highly effective in improving mental state and global functioning and is associated with reduced risk of relapse compared to standard care alone [119], [120], [123], [124]. [I] CBT in the acute phase, added to standard care can accelerate recovery and hasten hospital discharge [125], [126]. [II] CBT is effective in reducing symptoms in treatment refractory schizophrenia [127]. [I] Cognitive remediation warrants further research although evidence so far is equivocal [122]. [II]
Recommendation
CBT should be routinely available especially when positive symptoms are slow to respond or refractory to drug treatment. [I] CBT should be utilized to target distress and comorbidity. [III-2] Further improvement of CBT and related psychological interventions is required and should be the focus of further research. [V-2]
Social skills training (SST)
Since schizophrenia most commonly occurs for the first time in young people, they often miss out on engaging in many of the developmental tasks of late adolescence and early adulthood. These include developing social skills, intimate relationships, occupational skills, and independent living skills. SST (also called life skills training), a widely practiced intervention, seeks to address this. The capacity to function in social roles has been linked more specifically to the presence of cognitive deficits than symptoms [19], [128].
Social skills training improves social adjustment, enlarges and enhances the person's social network and contributes to the development of independent living skills [129]. The APA guidelines also point out that skills taught in programs do generalize, although this aspect is in need of more research [61]. Penn and Mueser found that SST was associated with symptom improvement but not with better social functioning [130]. While the benefit of SST has been demonstrated in a number of studies, a Cochrane review failed to find conclusive evidence of benefit [131]. Further well planned and conducted studies are clearly required.
Social and life skills training may not be linked to symptoms. When the cognitive deficits experienced by people with schizophrenia form the basis for a cognitive adaptation therapy program, outcomes across a range of social domains are improved compared to controls [132–136]. This seems a more sophisticated way to approach teaching people skills to live in the community.
Evidence
SST improves independent living skills. [II] SST can generalize to situations outside the inpatient setting. [I] SST in association with longer term group psychotherapy improves symptoms. [I] SST improves medication and symptom management skills. [I] Activities groups improve social interaction. [II] Cognitive adaptation therapy is a new approach with potential. [II]
Recommendation
SST should be available for patients who are having difficulty with tasks of living and occupation. Cognitive adaptation therapy should be considered where neuropsychological testing is available since it addresses cognitive difficulties that impede the learning of life skills.
Vocational rehabilitation
Schizophrenia is associated with low socioeconomic status (SES), but it remains uncertain to what extent this is a cause or effect. It is possible that low SES results from people drifting downwards socially because of the impact of the illness and a consequent inability to hold employment. In the USA unemployment rates among the severely mentally ill are estimated at 75–85%, and in the UK 61–73% [137]. Rates are very similar in Australasia [7], [13]. In addition, of those who could work, over half lost significant numbers of days to illness annually [138]. Apart from being a fundamental right, being occupied in a paid or voluntary capacity can increase selfesteem, alleviating psychiatric symptoms and reducing dependency and relapse [139–141], although it has been questioned whether working increases self-esteem [142]. Vocational rehabilitation (VR) aims to improve economic and social participation.
There are two main models of VR. These are prevocational training (where a period of preparation is engaged in prior to seeking competitive employment) and supported employment (in which people are placed in competitive employment with the provision of on-the-job support [143], [144]. A Cochrane review of VR found that supported employment was more effective than prevocational training [137]. The NNT for supported employment was 4.5 and in this form of VR, 34% of people were working at 12 months as opposed to 12% in the prevocational training conditions. Several other studies and guidelines support this finding [61], [143], [145–147].
Evidence
Becoming vocationally involved is likely to have positive psycho-social consequences. [II] People with mental illness, including schizophrenia want to find work, but are highly disproportionately unemployed. [V-1] Various models of vocational rehabilitation have shown different levels of success in placing people in competitive positions. [I] Supported employment is much more successful than other programs. [I] VR reduces rehospitalization II, and improves insight. [V-2] VR enhances vocational functioning. [I]
Recommendations
People with schizophrenia should be encouraged to find a meaningful occupation, either paid or voluntary. This should be actively facilitated by the clinician and specific programs to deliver this intervention need to be widely established. [I] People should be linked into agencies which provide such services early in the illness. [V-1] Liaison is essential with agencies to encourage them to be informed by research and to adopt (and evaluate) models shown to work elsewhere. [V-1] In planning new services, or developing of existing ones, vocational recovery staff should be included in the treating team. [V-2]
Case management
Since the move to community care of the mentally ill occurred in the 1960s and 1970s, in Australasia and other countries case management (CM) has steadily become the dominant model of care for patients. Models of CM [73], can, in theory, be divided into those in which services are brokered and those in which the case manager provides the treatment themselves. In reality, however, a case manager is often expected to perform both functions.
The outcome of research into CM is mixed. A review in the American practice guidelines for schizophrenia reported that controlled studies revealed inconsistent findings [61]. This was mainly attributed to methodological weaknesses, and the issue of defining and measuring CM. Marshall also found poor results in reviewing CM as an intervention [148], [149]. However, he acknowledged that CM in clinical services is often not implemented in the manner that its designers intended. Yet he concluded that there is no evidence base for retaining CM ‘as the cornerstone of community mental health care.’ [148]. However, Marshall's Cochrane Review has been strongly criticised as being flawed by unexamined bias [80].
CM in fact is not an intervention per se, but a model or a way of delivering services and treatments. Whether the model is successful or not also depends on the quality of the content of the model, i.e. the actual treatments. This has not been adequately controlled for in studies comparing CM with standard care. Another crucial issue is the modus operandi of CM, particularly whether the model is outreach or office-based.
Kopeliwicz and Liberman point out that a pure brokerage case management model is not effective [129]. Clinical CM (the therapeutic model) however, receives modest support. The Cochrane review [148] found that it increased the numbers remaining in contact with the system (one extra person for every 15 treated), but increased the numbers requiring hospitalization, and did not lead to improvements in any psychiatric or social variables in contrast to standard care. There was also some evidence of a lack of cost benefit for CM in that there was actually an increase in inpatient care rather than the forecast reduction. The Prism study [150] was interpreted as showing limited support for case management. Both the Prism study and the Cochrane review have been controversial and provoked an often intense debate about the value of case management [79–81]. Critics contend that studies such as Prism did not accurately test the questions as claimed [80], [151] and that a number of factors have conspired to prevent accurate and unbiased assessment of case management as a model of care.
A more specific type of CM is called Assertive Community Treatment (ACT). ACT differs from standard case CM, but shares the same goals of keeping people in contact with services, reducing frequency and extent of inpatient treatment, and improving outcome. The main difference is that ACT is a team-based approach. To run effectively and with fidelity, ACT needs to be conducted according to the model defined by an international expert panel. ACT leads to fewer hospital days compared to standard care, has a positive effect on outcome and facilitated contact is maintained. ACT teams are multidisciplinary, within which the skills of each discipline can used, rather than lost, as often occurs in officebased, generic CM. The ratio of clients to team members is around 15:1 and no more than 20:1 [74]. The modus operandi is one of outreach, which is precluded in most Australasian contexts by high caseloads and an officebased work practice.
Kopeliwicz and Liberman [129], argued that CM does not function well when clinicians have caseloads in excess of 20. However the UK 700 study [152], which examined alternative models of CM, found that reducing caseloads alone does not improve outcomes for hospital admission, clinical or social functioning. Instead the authors emphasized the importance of the quality and content of case management. However, this study had a number of methodological flaws, which tempers the interpretation of the results.
Although CM is a central component of the system of care for people with schizophrenia in many countries, it is relatively uncommon in many others, particularly in Europe. Where ACT is implemented according to wellestablished protocols, it produces significant benefits. More generally, because of the central importance of CM and multidisciplinary teams (MDTs) to the mental health system, and because of a number of complexities, large trials have been difficult to conduct with sufficient rigour. Despite these, it is important that such trials are carried out in a scientific manner [153].
Evidence
ACT is an effective service delivery model in schizophrenia. [I] There is insufficient evidence to unequivocally support standard, office-based CM models at present, however, no alternative model has to date demonstrated superiority to this approach. [III-3] Recommendations: ACT based CM should be developed in a comprehensive and routine manner for a substantial subgroup of patients. [I] Standard CM and CMHT models should continue and be enhanced. However further research should be carried out in the Australasian context to determine the most appropriate mix of CM and specialist multidisciplinary (MDT) interventions. [III-3, V-2] Lowering caseloads, setting standards for frequency, intensity and quality of contact, and a routinely available assertive outreach capacity are crucial enhancements urgently required. [III-3]
Compliance therapy
It is known that nonadherence with treatment is predictive of poor outcome in schizophrenia. Compliance therapy (CT) increased compliance with treatment in one randomised control trial [154]. CT uses motivational interviewing and cognitive behavioural techniques to help patients explore compliance issues [155].
Recommendation
CT may be usefully applied both in early and later phases of recovery. However, further research is needed to confirm its value. [II]
Psychodynamic therapy
Psychodynamic therapies were the original psychological approaches used to work with patients with schizophrenia [100], [156], [157]. Pioneering analysts laid the groundwork for modern psychotherapeutic interactions, however, their therapies were developed in the preneuroleptic era, and arguably were never sufficiently modified to fit within a biopsychosocial model [157]. Psychodynamic therapy (PT) declined because it was unable to demonstrate efficacy or effectiveness compared to supportive therapy [158]. New studies are underway in which PT has been adapted and integrated into services for first episode psychosis. However, the results of these services, while encouraging, need to be replicated [159]. While studies into psychodynamic approaches to psychopathology are complex to carry out, a Cochrane review of the area supports the following [160].
Evidence
Insight orientated psychotherapy is not superior to supportive therapy on key outcome variables in schizophrenia. [II] Insight-orientated therapy does not add anything to drug therapy alone. [II] Psychodynamically informed supportive therapy may be beneficial in combination with drug therapies. [V-2]
Recommendation
Psychodynamic knowledge and adjunctive supportive PT may enhance the understanding and management of the recovery process in people experiencing schizophrenia. However, there is no evidence to support the recommendation of insight-orientated PT as an effective stand-alone therapy for people with schizophrenia. [I]
Electroconvulsive therapy
Evidence
The evidence for the use of ECT in schizophrenia is not reviewed here. Despite earlier widespread use, more modern treatments have proven superior and more acceptable for most patients, and it holds only a residual place in management.
Recommendations
Electroconvulsive Therapy (ECT) may be considered in patients refractory or intolerant to medication. ECT may occasionally be useful when a distinct psychotic episode exists and the illness is characterized by catatonic or affective symptoms. [V-1] Patients with unremitting, chronic, neurolepticresistant schizophrenia are unlikely to respond to ECT. Nevertheless, there is evidence that ECT in conjunction with antipsychotics may be beneficial for at least some of these patients; therefore, this group could be considered for a trial of ECT. [V-2] When patients with schizophrenia develop severe depressive episodes, unresponsive to antidepressants, ECT may be the most desirable or effective treatment. [V-1]
Summary
A summary of the efficacy of psychosocial treatments may be found in Table 3.
Efficacy of psychosocial treatments for schizophrenia
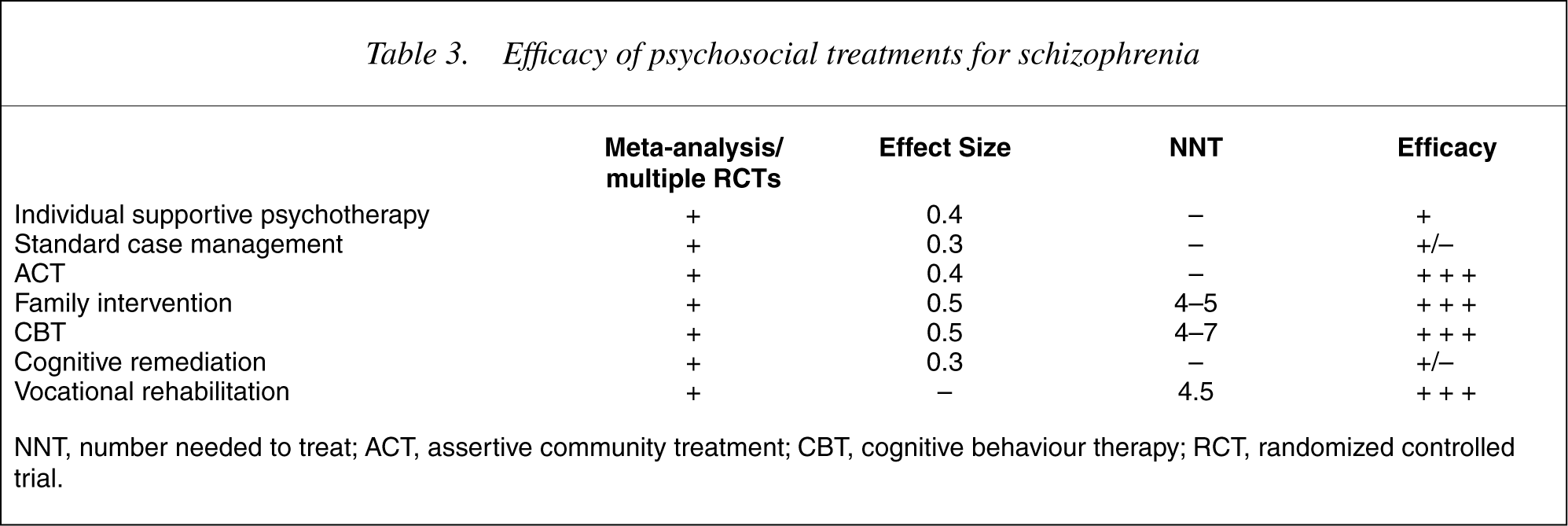
NNT, number needed to treat; ACT, assertive community treatment; CBT, cognitive behaviour therapy; RCT, randomized controlled trial.
Section 2: the stages of schizophrenia: a framework for clinical care
General considerations
As with other complex medical disorders, the management of schizophrenia is best considered in stages or phases. These stages of treatment are the prepsychotic or prodromal phase, first episode psychosis, recurrent or persistent psychosis including treatment of relapse and relapse-prevention, maintenance therapies, and treatment refractory schizophrenia.
The diagnostic flux which characterizes the early period of illness means that a broad symptomatic and syndromal focus is necessary in the first psychotic episode and especially the prodromal stage. There are a number of pathways into a schizophrenia diagnosis [161], and while a first psychotic episode with positive symptoms above a certain threshold and duration are necessary at some stage, for a substantial proportion of cases, this will be an earlier feature than the assignment of a schizophrenia diagnosis. Also some people will relinquish a schizophrenia diagnosis by transitioning to another one or remitting.
The prepsychotic or prodromal stage
Background
A prolonged period of symptoms and increasing disability, commonly termed the ‘prodrome’, occurs in most people prior to the emergence of sufficiently severe and persistent positive psychotic symptoms which then allows a diagnosis of schizophrenia or first episode psychosis. Distinguishing this ‘ultra high risk mental state’ from other disorders is difficult but becoming more feasible [22]. This phase is also associated with evidence of changes in brain structure, probably reflecting active neurobiological change during this period [26]. Much of the psychosocial disability is difficult to reverse even when the core symptoms remit with effective antipsychotic treatment as they do in up to 90% of people with first episode psychosis.
The ultra-high or at risk mental state involves:
Young people, usually aged 14 and 35 years. A change in subjective experience and behaviour in recent months or within the past 5 years (which may fluctuate but is persistent and often progressive). EITHER subthreshold positive symptoms (not severe or persistent enough to be regarded as evidence of sustained frank psychosis sufficient for a diagnosis of a DSM-IV psychotic disorder – other than brief psychosis, OR a family history of psychotic disorder or schizotypal disorder in a first degree relative plus a significant yet non-specific decline in psychosocial functioning within the past year or so which is not resolving. Or any patient the psychiatrist feels may be at an increased risk for early transition (other risk criteria may emerge with further research). Advantages of prepsychotic intervention are: Identifying people during a phase in which subtle yet tenacious disability is laid down (even before the first psychotic episode). Engagement can occur while the patient is not too out of touch. People usually will accept medication and outpatient care if indeed progression to frank psychosis or schizophrenia does occur [23]. Less trauma and less stigma is involved, because there is less risk of acute or embarrassing behaviour, and less need for hospitalization. This needs to be balanced against the potential risk of self-stigmatization especially for the false positives [162]. Reduction of duration of untreated psychosis (DUP), since first episode psychosis (FEP), if it occurs, can be recognized rapidly in well-engaged patients. Transition to FEP may be prevented or delayed in a subset [23]. The prepsychotic phase is an active focus for treatment research [163] and more evidence is required before definitive recommendations can be made. However there is increasing evidence that transition to psychosis can be delayed. CBT, antipsychotic medication, and neuroprotective agents are the strategies being studied in a number of controlled trials [23], [164], [165].
In the meantime the following recommendations can be offered.
Recommendations
The possibility of psychotic disorder should be carefully considered in any young person who is becoming more socially withdrawn, performing more poorly for a sustained period of time at school or at work, behaving in an unusual manner for them, or becoming distressed or agitated yet may be unable to explain why. [V-1] If subthreshold psychotic features combined with the onset of disability [22] indicating ultra-high risk are present, the young person and their relatives should be assessed and mental state and safety monitored regularly (every 2–4 weeks) in a context of ongoing support. This should be carried out in a home, primary care or office-based setting to reduce stigma, and with Aboriginal, Torres Strait islander or Maori patients the involvement of an indigenous health or mental health practitioner is recommended. [III-1] Current syndromes such as depression and substance abuse, and problem areas such as interpersonal, vocational and family stress should be appropriately managed. [III-3] Many such young people and their families are already aware of the risk of a more serious problem, such as psychosis, schizophrenia or severe mood disorder, developing. Information about the level of risk should be carefully provided taking into account social, educational and cultural factors. This should be done with therapeutic optimism, confirming that current problems can be alleviated and that progression to frank psychosis is not predetermined, nor would it be catastrophic, since effective and welltolerated treatments are readily available. The patient can be reassured that if a fully fledged psychotic disorder were to develop, the outcome would be better and treatment less disruptive, since they would be well engaged and informed and there will be minimal treatment delay. [III-3] Antipsychotic medications should not normally be prescribed unless at least 1 week of frank positive psychotic symptoms have been sustained. The exception may be where briefer or milder positive symptoms are directly associated with risk of self-harm or aggression.
First episode psychosis (FEP)
Background
The two key issues here are timing – the reduction of treatment delay (DUP or duration of untreated psychosis) [29], and quality – the provision of comprehensive phase-specific treatment of the first psychotic episode [38], [39], [65], [76], [166].
Early identification combined with optimal treatment for however, long it is required is very likely to reduce the burden of disease while it is active [168]. In any event, as recognized in the UK [65], [75] and many developed countries [169], long-term outcome improvements should be seen as a bonus not a prerequisite for improved clinical standards during the critical onset period.
Recommendations
Improved mental health literacy, primary care quality and accessibility of public and private psychiatry to potential first episode psychosis are obvious strategies. Community wide and culturally informed education systems should be established to increase public understanding of how psychotic disorders emerge in a previously healthy person, and how to go about seeking and obtaining relevant advice and effective treatment [170–172]. [II] A high index of suspicion and a low threshold for access to expert assessment should be set for any person suspected of developing a psychotic disorder for the first time. [V-1] Entry to and retention within specialist services is usually based on reaching and maintaining a threshold of behavioural disturbance or risk, disability or chronicity. This reactive, crisis-orientated model is not only risky, but also contributes to unnecessary demoralization and therapeutic nihilism among clinicians, and creates a traumatic environment for people with schizophrenia, their families and for clinicians. Active retention of patients throughout the critical period of the first 3–5 years of illness, combining developmental (youth) and phase-specific perspectives, should be a priority for all specialist mental health services. Specialized early psychosis services are an increasingly widespread response to this need [76]. [III-3] Initial treatment should be provided in a community or home setting if at all possible [173] and draw on relevant cultural expertise. This usually minimizes trauma, disruption and anxiety for patient and family, who will be at best poorly informed and harbour fears and prejudices concerning inpatient psychiatric care. However, inpatient care is clearly required if there is a significant risk of self harm or aggression, if the level of support in the community is insufficient, or the degree of crisis is too great for the family to manage. [V-1] Inpatient care should be provided in the least restrictive environment. Ideally this means units which are streamed by phase of illness and developmental stage, relatively small in size and adequately staffed, so that 1:1 nursing of highly distressed, suicidal or agitated young people is feasible without locking the unit or secluding the patient. The use of traditional psychiatric ‘intensive care’ has been demonstrated to be especially traumatic for these patients [174–177]. Where streaming is not possible, a special section may be created in a general adult acute unit for young recent-onset patients. [III-3] Pharmacological treatments should be introduced with great care in drug-naïve patients with the overriding principle of doing the least harm while aiming for maximum benefit. This means the graded introduction with careful explanation of low dose antipsychotic medication [178–180] along with antimanic or antidepressant medication when these syndromes are present. I. Such doses will probably not have much early effect (within the first few days) on distress, insomnia and behavioural disturbances secondary to the psychosis, so skilled nursing care, a safe and supportive environment, and regular and sufficient doses of benzodiazepines are all essential interim components of management. [V-1] The first line use of atypical antipsychotic medication is well justified on the basis of better tolerability and reduced risk of tardive dyskinesia. This is supported in the most recent guidelines from the developed world [65]. [I] In the longer term the risk-benefit ratio may change for some patients, for example if weight gain, impaired glucose tolerance or sexual side-effects associated with the atypical agents develop. Alternative atypical and typical antipsychotic medications may then be reconsidered. Baseline MRI scan, neurocognitive assessment, neurological examination for neurological abnormalities and movement disorder, ECG, height and weight (BMI), illicit drug screen, lipid profile and fasting serum glucose (and/or HbA1c) are all part of optimal initial assessment [99], [181]. [V-1] Psychosocial interventions, especially CBT, have a fundamental place in initiating treatment, in providing a humane basis for continuing care, in preventing and resolving secondary consequences of the illness, and in promoting recovery. CBT may also be helpful for comorbid substance use, mood and anxiety disorders and for improving treatment adherence [182]. [II] Families, and whenever possible and appropriate, other members of the person's social and cultural network, such as friends, teachers and employers, should be actively supported, progressively informed and educated about the nature of the problem, the treatment and the expected outcomes. Families need an individualized response as well as the opportunity to meet other families in the same predicament. A combination of individual and multifamily approaches is therefore best. If there are frequent relapses or slow early recovery, a more intensive and prolonged supportive intervention for families is required. An optimistic and patient approach is vital for both families and patient especially if the early course is stormy or there are additional family problems or secondary consequences of untreated illness. [I] If recovery is slow and remission does not occur despite sustained adherence to two antipsychotic medications (at least one of which should be an atypical) for 6 weeks each, early use of clozapine and intensive CBT should be seriously considered [33]. [I] Early clozapine use should also be considered if suicide risk is prominent or persistent, despite treatment for depression, if such treatment is ineffective, or if depression is not prominent [183]. [II]
See Table 4 for a summary of the interventions in the pre-psychotic and first episode phases of schizophrenia.
Interventions in the pre-psychotic and first episode phases
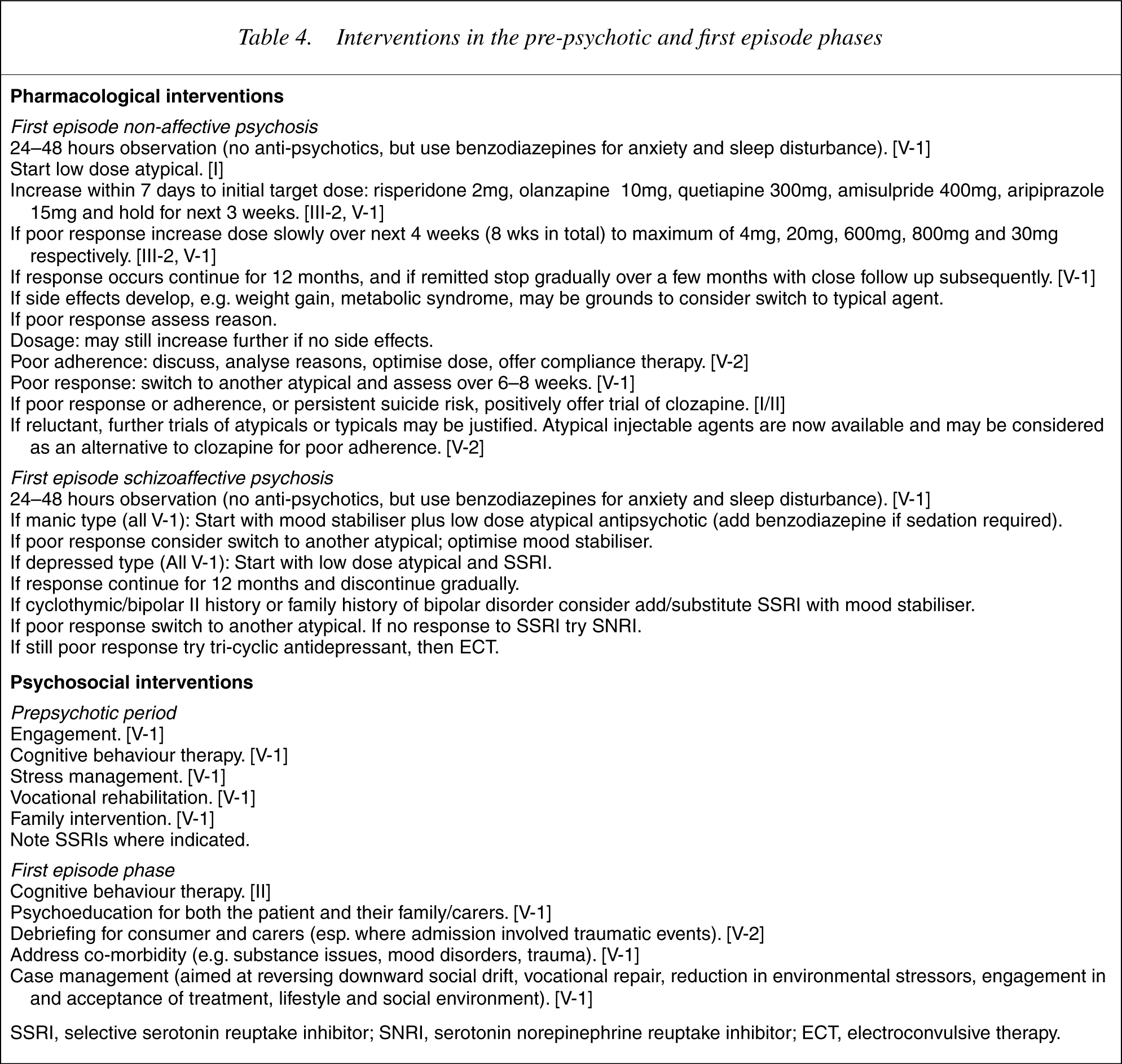
SSRI, selective serotonin reuptake inhibitor; SNRI, serotonin norepinephrine reuptake inhibitor; ECT, electroconvulsive therapy.
Recovery and relapse: treating schizophrenia in the critical period
Background
A substantial number of people who have one episode of psychosis will go on to have more episodes or continuing disability and may come to fit the conventional picture of schizophrenia. Naturalistic follow-up studies show the early years after entry to treatment are characterized by an often fulminant early course which can reduce the ceiling for ultimate levels of recovery [39], [184]. Relapses are common during the first 5 years and the vulnerability to relapse persists in up to 80% of people [34]. Young people in particular naturally find it difficult to accept the lifestyle change of taking daily medication, especially if they have substantially recovered, and usually need to be convinced through personal experience of symptom recurrence that they have an ongoing need for medication and other interventions.
Unfortunately this often results in one or more relapses, which confer an increased risk of self-harm, victimization, aggression, lifestyle disruption and accumulating treatment resistance. A substantial minority of patients experience this stormy early course of illness with the risk for suicide peaking during this period [185]. Secondary consequences such as persisting and worsening substance abuse and dependence, vocational failure, and family stress and breakdown are all common. Marginal lifestyles and homelessness are also a serious risk. It is essential that high quality and intensive biopsychosocial care is continuously provided in an assertive way during this critical period. However in practice, patients are rapidly discharged to primary care and must experience acute relapse, a suicide attempt, or manifest severe disability before care is made available in a reactive, ‘too little, too late’ manner. Thus services tend to disengage at precisely the time when they are most needed. An ‘episode of care’ model is not consistent with true shared care and is inappropriate for most patients. This scenario supports the introduction of the following recommendations.
Recommendations
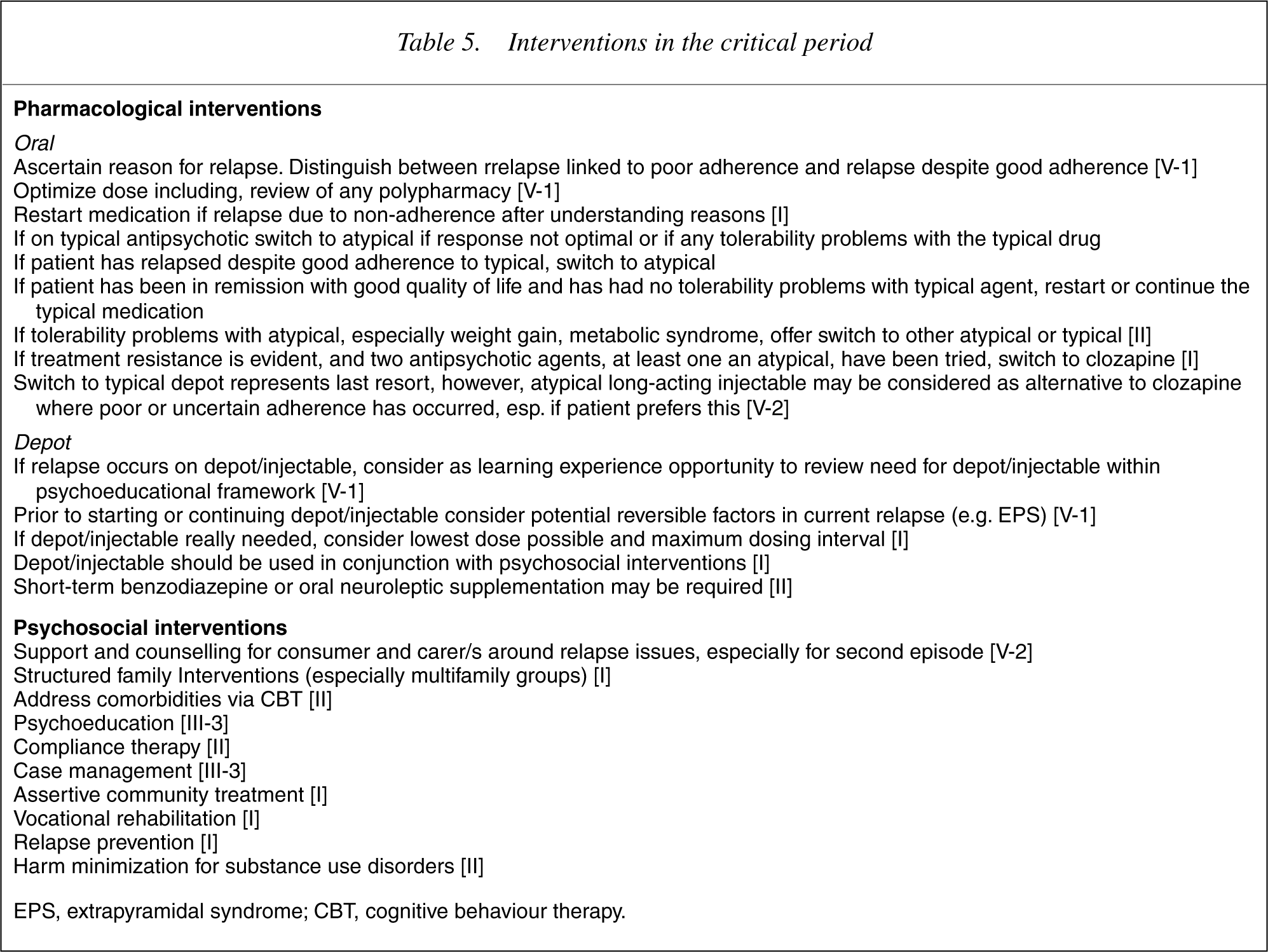
In fully remitted patients, antipsychotic medication should be continued for at least 12 months if possible and then an attempt made to withdraw the medication over a period of at least several weeks. Close follow up should be continued with specialist review for a further period of 12 months beyond this and any relapse rapidly identified and treated. Patients should not be discharged to sole primary care during this phase, though shared care is optimal at all stages. [V-1] Partially remitted patients (approximately 20% of FEP) should be considered, after a trial of 2 antipsychotic medications, as manifesting treatment resistance and should follow the specific guidelines for this subgroup. [III-3] Even in fully remitted patients a range of psychological, family and vocational issues will need to be addressed, as well as substantial comorbidity, especially substance abuse, depression, PTSD and social anxiety. Treatment should be actively offered for all these aspects. [V-1] Every patient has the right to a safe and secure home environment. [V-1] Family support and intervention should be consistently provided [186], [187]. [I] Suicide risk must be actively monitored and responded to [183], [185], [188]. [II] Vocational recovery interventions, especially in vivo supported employment [141],[143–147],[189–192], should be offered once a stable clinical state has been achieved. [I] Most patients should continue to be seen primarily within specialist mental health care throughout the early years of illness and not be discharged to primary care upon improvement of acute or more florid symptoms, following each ‘episode of care’. This phase of illness is complex to treat well, confers high levels of risk of many types, and is also the phase with maximum potential for cost-effectiveness [193]. However, ‘shared care’ arrangements driven by clinical rather cost factors should be actively developed. [V-2]
Interventions in the critical period
Prolonged schizophrenia: maintenance treatment and care
Background
The main issues over the longer term involve a blend of lifestyle problems and the physical and mental sequelae of chronic illness. Poverty, poor housing, a strained relationship with family members, social isolation and unemployment are frequent serious handicaps flowing from persistent schizophrenia, particularly in the deinstitutionalized context. Clinical foci include continuing relapse prevention, reducing the demoralizing effects of persistent psychotic symptoms, depression and suicide, substance abuse, smoking, family relationships and vocational rehabilitation. Disturbingly high physical morbidity and premature mortality reflects the impact of these factors and closely resembles the pattern seen in other highly disadvantaged groups within the society.
In addition to quality social and psychiatric care, the longer term treatment of schizophrenia therefore involves increased vigilance regarding the general medical care of the patient [52], [99], [196], which has been shown to be seriously inadequate, and the related issue of changing risk-benefit ratios for medication. Atypical agents are now known to variably produce obesity, lipid abnormalities, cardiac abnormalities and impaired glucose tolerance. These risks, superimposed upon those arising from an impoverished, inactive lifestyle and smoking, demand a preventive approach targeting known malleable risk factors, as well as regular monitoring of risk and disease. The emergence of obesity, impaired glucose tolerance, tardive dyskinesia, hypertension, cancer and cardiovascular disorders should be regularly considered, particularly with Aboriginal, Torres Strait Islander and Maori patients, where mental health interventions should be integrated with chronic disease management at the primary care level. While the risk of tardive dyskinesia has been reduced with the atypicals, the risk of obesity, diabetes mellitus, dyslipidaemia and sexual side-effects has been increased. Preventive health care for these potential problems should also be offered earlier on. Lifestyle (exercise, smoking cessation, etc.), the social environment and vocational rehabilitation are increasingly being seen as crucial.
Recommendations (All V-1)
Within a CM framework, the patient's social environment and social capital should be actively maintained and enhanced. This requires ready access to paid work or financial support and acceptable housing quality. Social relationships need to be encouraged and key clinical foci must be proactively addressed, especially medication adherence, depression and suicide, substance use, family relationships and vocational roles. Since this cannot normally be done in primary care settings, a specialist multidisciplinary team is usually required. Ideally in conjunction with the patient's GP, full physical check-ups, including weight, blood pressure, lipid profile, ECG, and fasting blood glucose should be done at least annually [see 99,181]. Routine screening for cervical and breast cancer should be carried out in females. In patients over 40, it is important to enquire for any new symptoms, and conduct accepted screening tests for common forms of cancer. If it is not certain that primary care will guarantee physical health monitoring of this type, then it should be carried out by the psychiatrist [99]. Encouragement and intervention should be offered to cease smoking, to reduce or cease illicit drug usage, and to exercise and adopt a healthy diet. Sexual function and side-effects should be reviewed regularly and backed up by measurement of prolactin levels where indicated. 6 monthly examination for signs of tardive dyskinesia should be carried out. Relapse prevention strategies, such as promotion of adherence, family intervention and monitoring for early signs of relapse should be continued. The possibility of late remission should be kept in mind and the need for continuing antipsychotic medication reviewed. Meaningful social role development and maintenance should be facilitated, especially via vocational rehabilitation.
Treatment refractory schizophrenia
Background
In a substantial minority of people with schizophrenia, symptoms will persist despite comprehensive treatment and this phase has been termed treatment refractory schizophrenia. Clinicians should continue to be hopeful of positive change, and not view such patients nihilistically. Treatment resistance should be a trigger for renewed efforts to improve the clinical response. Furthermore, late remissions are not uncommon in treatment resistant patients [2] and even in the presence of disability, as with all other illnesses, health and good quality of life can coexist. About 10–15% of first episode patients will develop early treatment resistance [33], however, with sample selection and the passage of time this proportion cumulatively increases to around 30–50% in standard services [197], which has had the effect of creating a biased perception of the level of chronicity in schizophrenia.
Treatment resistance can be defined narrowly in terms of persistent positive symptoms poorly responsive to antipsychotic medication or broadly to include persistent negative symptoms and disability of various kinds. The latter is more prevalent than the former. Only a minority of patients in Australasia meeting even the narrower definition have been offered clozapine or CBT.
Other factors that may produce a similar clinical picture should be excluded. These include: marked yet subtle EPS, unrecognized depression, inadequate psychosocial rehabilitation, poor adherence, differential drug behaviour, therapeutic windows, substance abuse, drug interactions and inappropriate drug therapy.
Recommendations
Poor adherence, EPS, depression, substance abuse, polypharmacy, and the quality of the social environment should be considered and addressed. [V-2] Two adequate trials (at least 6 weeks of 300–1000 mg in CPZ equivalents) of antipsychotic medication, of which at least one agent should be atypical, should have been conducted. If not this should be done. [V-1] Clozapine is the treatment of choice for clearcut treatment resistance. [I] If there has been poor or uncertain adherence, depot/ long acting injectable medication could be considered, but clozapine may be preferable since the monitoring linked to this often enhances adherence. Now that long acting injectable atypicals are available this recommendation may warrant reappraisal. [V-1] CBT should be offered either in conjunction with clozapine or as an interim alternative to it if the patient is unwilling to consent to clozapine. In this situation, especially if CBT is unsuccessful, every effort should be made to persuade the patient and family to try clozapine. CBT should always be provided should there be no response to clozapine and vice versa. [I] Family, personal and social support, and a safe and decent lifestyle are critical for this group of patients, who are at risk of being marginalized and demoralized, along with their relatives. [I] If treatment resistance persists despite clozapine, the most effective prior drug should be reinstated and an appropriate adjunctive therapy, such as lithium, added. There is little evidence that combining antipsychotic medications is useful; conversely this increases the side-effect burden. No patient should be regarded as a ‘lost cause’, even though symptoms are unremitting. Symptoms may persist but often wax and wane, and can still be compatible with good quality of life even if they are at times severe. [V-2]
The management of acute emergency in schizophrenia
The quality of the evidence to guide the management of emergencies in schizophrenia is extremely poor, resulting in highly variable and often iatrogenic clinical practices. For this reason and to conserve space, a brief summary only of the key guidelines is provided here. The latter are based on clinical logic, expert consensus and an overriding desire to manage risk in a humane and non-iatrogenic manner. [V-1]
Key goals and principles
Primary prevention of emergency situations and restraint. Prevention of physical harm to patient, other patients and clinical staff. Prevention of psychological trauma arising from the management of emergency situations to patients and staff. Prevention of adverse events from use of physical or pharmacological restraint during acute emergency situations. Prevention of sequelae of emergency restraint.
Preventive strategies
Clinical environments should be well designed and furnished to reduce stress and fear. A domestic feel should be created where possible. Overcrowding and noise should be avoided. Soft lighting and music can help, and in services providing for indigenous patients, appropriate posters and pamphlets can signal inclusiveness and consideration. Providing space and resources for designated relatives may be a significant factor in reducing agitation. Unprepared confrontations should be avoided. Escalating tensions should be identified and defused. Counterprojective behaviour and language should be utilized and any subtle physical or verbal confrontation avoided. If the patient is not combative, non-pharmacological interventions should be employed: The patient's usual clinician should try to engage the patient Patient's concerns should be responded to if possible and the family supported Reassurance should be offered and attempts to resolve conflict made. As much control as possible should be returned to the patient. The patient (if an inpatient) should be encouraged to enter a secure area if possible (or at least separated from other patients, who will also need immediate explanation and support). Agitation and risk of violence should be expertly graded according to established scales.
Emergency care
Most patients and especially neuroleptic-naive young people are highly sensitive to EPS, hence typical neuroleptics should only be used as a last resort in emergency tranquillization. Even in multiepisode patients, the doses of typical neuroleptics (especially high potency drugs) required for tranquillization inevitably exceed the threshold for EPS. If the patient is non-combative, oral therapy with benzodiazepines should be tried, e.g. lorazepam 1–2 mg or diazepam 5–10 mg. Oral olanzapine wafers (5–10 mg) or oral quetiapine (50–100 mg) may be useful as a next option. The use of haloperidol is quite inappropriate, as it is non-sedative and is associated with severe EPS and dysphoria in most cases. Substantially higher doses of benzodiazepine may be required for some patients, especially those with severe substance dependence. If the patient is already combative, refuses oral medication or if the initial strategy does not lead to response, or the response must be rapid due to escalating aggression, parenteral medication will be necessary. 5 mg midazolam IM is the best initial strategy. As benzodiazepines may rarely cause respiratory depression (especially in older patients or if other sedatives present), staff trained in resuscitation techniques, suitable equipment (airway and airbag), flumazenil (benzodiazepine antagonist), and direct observation of the patient for up to 2 h must be available. The latter is essential anyway following emergency sedation and reduced conscious level. Onset of action is rapid usually within 5–15 min, and the clinically useful sedative effects may last for some hours. These policies are achievable in mainstreamed general hospital acute psychiatric units and emergency departments, and hence the use of midazolam should normally be first line (some emergency physicians prefer to give IV midazolam for speed and predictability of action). It is a safer option than parenteral antipsychotic medications, such as droperidol (QT problems) and haloperidol (extrapyramidal side-effects). IM clonazepam (0.5–2 mg) and more recently IM olanzapine may be useful alternatives. Once again (parenteral) haloperidol is likely to be the most iatrogenic and least effective strategy. If initial steps have been ineffective or the patient refuses outright, the following can be tried. If there is no response to oral benzodiazepine and sedative oral atypical therapy, chlorpromazine 50–100 mg orally can be tried. If there is no response to IM therapy, droperidol can be considered. While an ECG may have been impossible to perform beforehand, an ECG after tranquillization is necessary to monitor the QT interval, and access to CPR and defibrillation must be assured. Where repeated injections are occurring, zuclopenthixol acetate can be considered. Low doses are essential especially in neuroleptic naïve patients as EPS are frequent. After parenteral tranquillization, the following parameters should be monitored: temperature, pulse, blood pressure and respiratory rate every 5–10 min for one hour, then half-hourly until patient is ambulatory. Caution should be exercised, especially in patients who have never before received neuroleptics, because of higher risk of reduced respiratory rate, irregular or slow pulse, fall in blood pressure, acute dystonia and unconsciousness. If available, ECG monitoring is also strongly recommended, especially when higher doses are used. Possible extrapyramidal side-effects should be treated early, e.g. acute dystonic reactions with benztropine (1–2 mg IM or IV) or procyclidine (5–10 mg IM or IV).
Post-emergency care
After remission of symptoms and with the patient's compliance, the patient should normally be maintained on the lowest effective dose of an atypical antipsychotic. Debriefing for patients, staff, family members or other caregivers should always be provided.
Conclusion
These guidelines tackle only one element in the endeavour to reduce the impact of schizophrenia. They distil the current evidence-base and make recommendations based on the best available knowledge. The evidencebase is incomplete and of variable standard, indeed it is striking how much more clinical research is required. The evidence has been interpreted from a purely clinical perspective. Another perspective has recently been advanced intended to influence the management of people with schizophrenia in Australia [15]. This approach can be termed ‘assumption-based medicine’ to highlight the contrast with true evidence-based medicine. Much of this work argues, using selective data, embryonic modelling and debatable assumptions [16], [17], for a pattern of treatment based principally on economic rather than clinical grounds, one which, intentionally or otherwise, risks supporting the current bias towards reactive acute management with a limited focus on aftercare and recovery programs. This approach has the potential to undermine the improvement in treatment quality that is desperately required as well as readily achievable, since it is naturally appealing to governments intent on limiting growth in mental health spending. Despite the reputedly high direct cost of treating schizophrenia in Australia and New Zealand and the tight targeting of services to ‘serious mental illness’, expenditure, in Australia especially, sits at bargain basement levels within the developed world. Treating schizophrenia adequately, and to the best of our present ability, will cost substantially more in direct costs, and will require a more specialized, professional and proactive approach. This goal should not be allowed to conflict with the equally urgent need to broaden the coverage and quality treatment of the full range of mental disorders, an objective of equal value which the schizophrenia field strongly supports.
These guidelines are inevitably a ‘work in progress’. The evidence base continues to grow steadily and, despite gaps and the lack of uniform level I evidence, is relatively clearcut, as judged by the degree of consensus between these guidelines and those from other countries, which have produced similar documents. Naturally, there is room for much greater efficacy in the treatment of schizophrenia, however, an urgent priority is to translate the knowledge we already have into frontline clinical care of people with schizophrenia to produce more effective care. To this end these guidelines have highlighted some of the obstacles to this translation. These include skill levels, workforce quality and work practice issues, and division and political weakness within the mental health field, however, the minimalist approach to the funding of specialist mental health services for schizophrenia in the postdeinstitutional era is a fundamental barrier and must be addressed urgently.
Footnotes
CPG Editorial Team
Patrick McGorry and Eóin Killackey (ORYGEN Research Centre & Department of Psychology, University of Melbourne); Tim Lambert (OPEN and Department of Psychiatry, University of Melbourne); Martin Lambert (ORYGEN Research Centre and Department of Psychiatry, University of Hamburg).
Expert Advisory Panel
Henry Jackson (Department of Psychology, University of Melbourne and ORYGEN Research Centre); David Codyre (Health Innovations, Auckland); Norman James (Former Chief Psychiatrist of Victoria, Clinical Director, Glenside Hospital, Adelaide); Christos Pantelis (Melbourne Neuropsychiatry Centre, Department of Psychiatry, University of Melbourne); Jane Pirkis (Centre for Health Program Evaluation, University of Melbourne); Peter Jones (Department of Psychiatry, University of Cambridge); Mason Arohia Durie (Massey University, New Zealand); John McGrath (Queensland Centre for Mental Health Research); Thomas McGlashan (Yale University, New Haven, USA); Ashok Malla (Department of Psychiatry, McGill University, Montreal, Canada); John Farhall (Senior Lecturer in Psychology, La Trobe University and North-west Mental Health); Helen Hermann (St. Vincent's Hospital and Department of Psychiatry, University of Melbourne); Barbara Hocking (Executive Director, SANE Australia).