
Abstract
The relatively low involvement of women psychiatrists in research is a matter of concern [1–8]. Women are entering the profession in increasing numbers. In Australia, for instance, currently one in four psychiatrists are women but they comprise half of those in training [9]. However, the proportion contributing to its academic advancement is diminishing [1], [2], [5], [10], [11]. Comparable figures exist for the US: only one in three academic psychiatrists are women and a mere 14% occupy senior professorial positions [12]. Canadian figures mirror this pattern [13]. Despite 50% of British medical graduates being women, only one in 10 is found in academia – across all specialties [14]. Psychiatry can ill afford to lose the contribution to research of half its members; they are obviously a rich pool from which to recruit future investigators [1], [15].
Men and women psychiatrists' reports of different career experiences may help to illuminate the disparity in research activity. Specific factors, however, remain elusive [2], [6], [13], [16]. For instance, although an entire issue of Academic Psychiatry highlights the shortage of researchers in psychiatry, gender differences are not considered [17].
A range of factors may account for the gender imbalance, including less access to mentoring opportunities [1], [4], [5], [13], lack of role models [16], [18], inflexible career structure [10], [12], a promotion system biased against women [1], family responsibilities [4], [8], [10], [18], [19] and relatively fewer women in the higher echelons of academia [1], [19]. Research on these aspects has been conducted largely in North America and the UK [2], [4], [13],[20–23]. The picture in Australasian psychiatry is similar but has not been examined systematically. In the light of sparse knowledge overall and among Australasian women psychiatrists in particular, we have studied the attitudes to research of women Fellows of the RANZCP in the hope that better understanding of what contributes to the prevailing gender disparity could point to strategies to improve the situation.
When considering women's research careers, it is useful to reflect on factors that influence gender-based attitudes and behaviour. Various theoretical frameworks compete for our attention. Psychoanalytic thinking has classically portrayed women as instinctually driven, inferior, passive beings. A cognitive-developmental approach, such as that mapped out by Piaget, also espouses biologically influenced factors [24].
A feminist view has it that a woman's reproductive function is the sole biological reason for gender differences, since it forces women into socially constructed roles and these differences could therefore be overcome with the provision of appropriate opportunities [24].
Socialization theories posit that gender-based behaviour and attitudes result from selective reinforcement [24]. According to gender schema theory, the root of gender differences is attributable to the human tendency to form hypotheses (and stereotypes) about others. Thus, Valian [25] asserts that a set of non-conscious hypotheses about these differences, acquired in early childhood and extending throughout life, play a pivotal role in influencing men's and women's professional experiences. In the case of medicine, women are disadvantaged because men have moulded the profession so that attributes traditionally associated with men – technical competence, autonomy, linear reasoning and competitiveness – are rewarded and feminine qualities of empathy, supportiveness and collaborativeness are devalued [26]. Women doctors are in fact under-represented in the spheres of research, administrative leadership and policymaking [1–3],[12], [27]. Socialization theory helps to explain such patterns. Socially acquired identity leads to career choices that support gender stereotyping [27]. This may account for the relatively high proportion of women in psychiatry and general practice.
Attention has focused recently on the role of institutional factors (rather than individual preferences) in determining career choice in medicine [12],[28–30]. Structural barriers may act as gatekeeping mechanisms to the inner circle of medicine [27]. In such a hierarchical profession as medicine, women doctors encounter difficulty negotiating networks of power, which is necessary in order to attain positions of authority [12].
Given the multiplicity and variegated nature of theories and the sparse knowledge on factors operating in women psychiatrists, we opted for an atheoretical research approach but relied on past empirical studies together with our own intuitive understanding.
Method
We devised a questionnaire to fulfil two purposes: identify research involvement and ascertain facilitating and hindering factors. Using a list of women Fellows in the Royal Australian and New Zealand College of Psychiatrists 2001 database, we conducted an anonymous postal survey of this group (n = 670) in 2001. A reminder letter was sent 6 weeks later. The questionnaire covered: demographic details; level of research involvement; factors affecting participation in research; institutional influences (for example, protected research time and availability of mentors and role models); and family aspects. We also sought suggestions as to how to promote research among women. Likert-type scales were used to measure respondents' attitudes and an opportunity to elaborate on their responses was provided.
Responses were analyzed using the Statistical Package for the Social Sciences [31]. We applied the χ2 to examine for differences between researcher and non-researcher groups.
Results
Fifty-six per cent of the 670 women in the sample responded. Their average age was 48 (SD = 11, range 30–86). Seventy per cent were married or in de facto relationships, 5% were widowed, 15% separated or divorced and 10% single. Three-quarters had children (mean = 1.6, SD = 1.3).
The women had graduated an average 24 years earlier (SD = 11) and worked in specialist practice for an average 12 years (SD = 9). The mean interval between graduation and attainment of specialist qualifications was 12 years (SD = 6). Two-thirds specified an interest or involvement in a subspecialty, mainly child psychiatry, psychotherapy and psychogeriatrics. The average period in a subspecialty was 11 years (SD = 7.8). Fifteen (4%) had retired, of whom two retained a research position.
Comparing the researchers and non-researchers
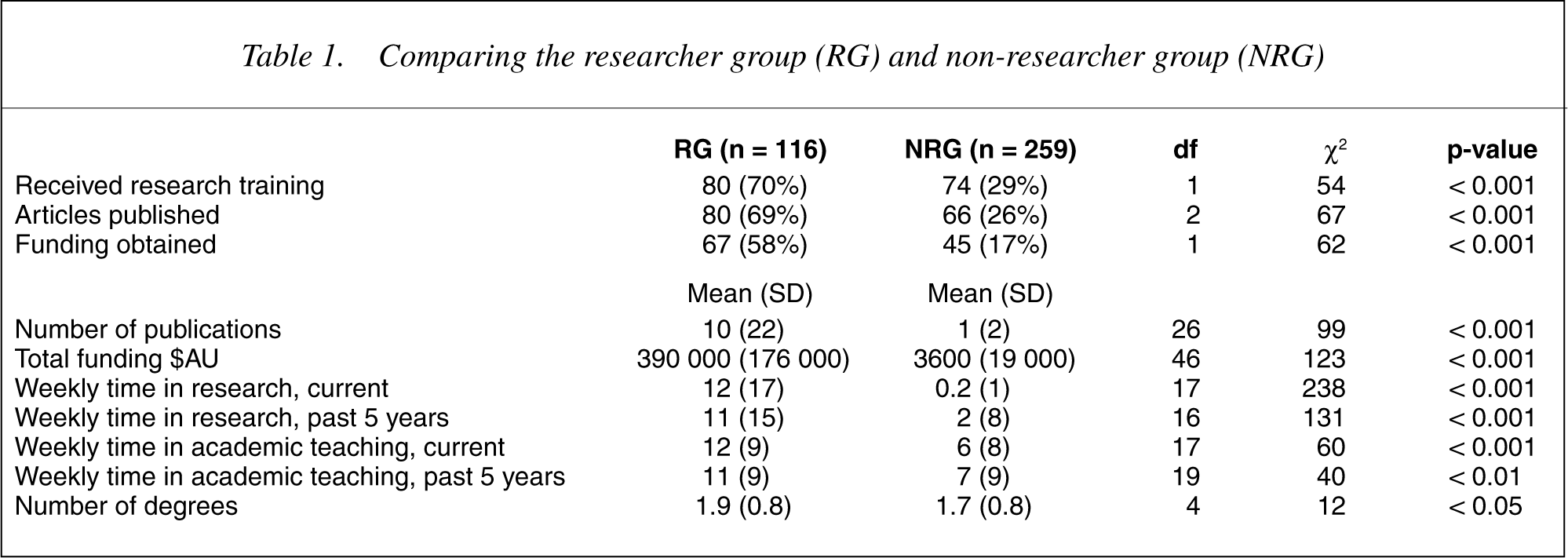
Several questions were to distinguish between researchers and nonresearchers. The emergent groups, 116 (31%) involved in research and 259 (69%) not, differed significantly in relation to time committed to research, research funding obtained, and publications (Table 1). Not unexpectedly, researchers were more likely to have received research training than non-researchers, spent more hours a week on research at the time of the survey and during the previous 5 years. Researchers devoted more time to academic teaching and acquisition of higher degrees. Twice as many researchers as non-researchers had published peer-reviewed articles; the average number was substantially greater. The researchers had obtained funding for their studies far more often than their non-researching counterparts; the average amount was 100 times greater.
Comparing the researcher group (RG) and non-researcher group (NRG)
Factors influencing research involvement
In comparing the researcher group (RG) and non-researcher group (NRG) on factors that could reasonably be anticipated to encourage participation in research, the role of the professional environment emerged as most notable (Table 2). Twice as many RG as NRG members saw the employing institution as exerting a substantial facilitatory effect, in particular by setting time aside for staff to conduct research and by having women in senior positions and active in research. In addition, twice as many RG as NRG women were aware that affirmative action policies applied to their employing institution.
Factors influencing involvement in research in researcher group (RG) and non-researcher group (NRG)
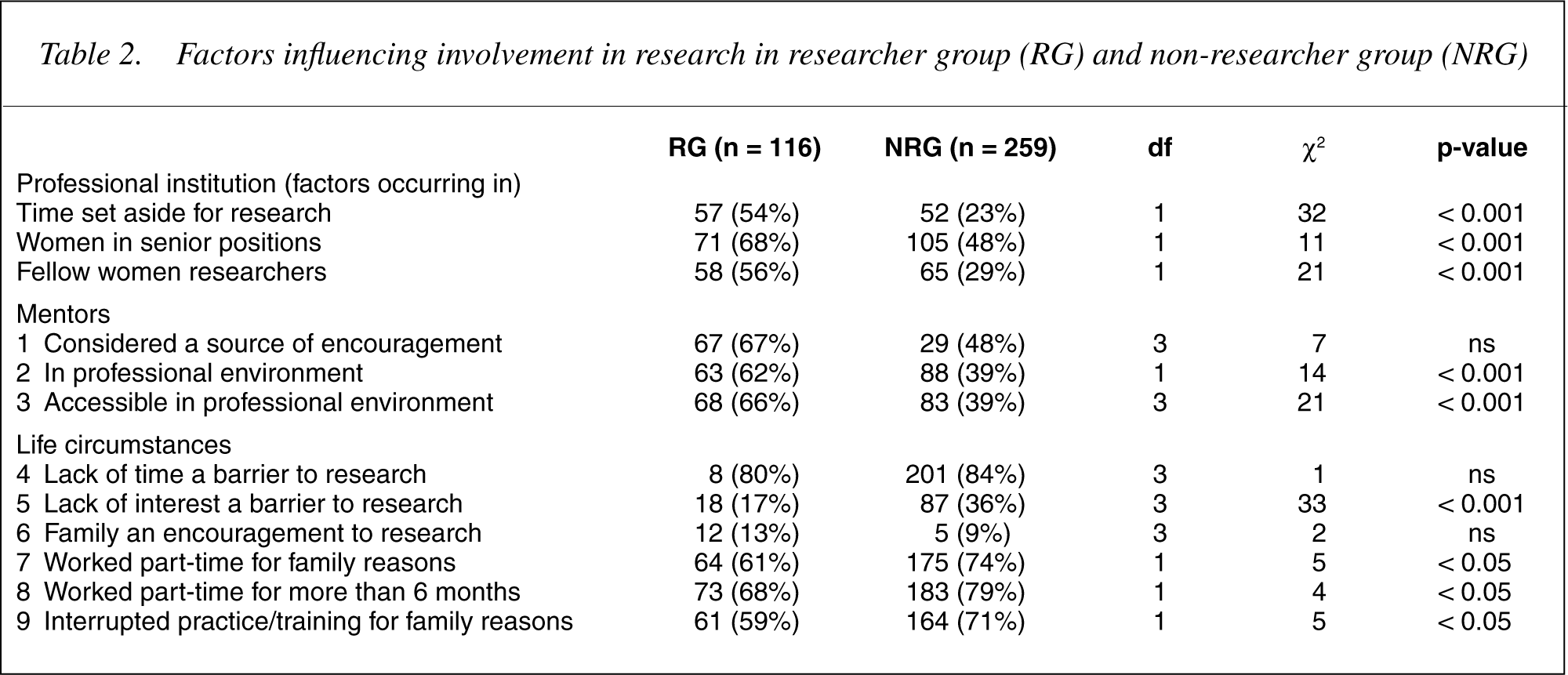
Mentoring also stood out as influencing participation in research, with two-thirds of the RG viewing a mentor as exerting a positive effect compared to under half of the NRG. In their current professional environment, mentoring was available to 62% of the RG but only to 39% of the NRG. Similarly, two-thirds of the RG had been able to access a mentor compared to about a third of the NRG. Members of both groups, in similar proportions, regarded the lack of a mentor as an impediment. An unsuitable mentor exerted a substantial hindrance to research participation in a third of the RG compared to a fifth of the NRG.
Both groups viewed the RANZCP (the educational body responsible for promoting clinical practice and training) as having only a minor role in encouraging research. Lack of training in the area was considered by half of each group to hamper becoming an active investigator.
Equal proportions of both groups saw lack of finances as exerting either a substantial or minor role. Both groups equally considered lack of time as a barrier to research (i.e. no consistent pattern emerged) although the RG was less likely to have worked part-time in order to spend more time with family or to interrupt their professional practice or training.
A striking negative finding was both groups not regarding the opportunity for flexible work schedules hours as a spur to do research.
Discussion
We were able to confirm the relatively small proportion of women psychiatrists in the research domain by allocating respondents to RG and NRG groups based on self-identification and bolstered by level of research funding, papers published and time devoted to research. We are confident therefore that we could meaningfully compare the two groups in terms of facilitatory and inhibitory influences.
The factor emerging as most crucial in aiding women psychiatrists' involvement in research is the professional environment, specifically the presence of women researchers, women colleagues occupying senior positions and time dedicated to research. This is exemplified by this typical comment from an RG respondent: ‘Lively research department which allowed much cross-talk and fuelled and grounded ideas.’ Lack of such a milieu was often mentioned, for example: ‘My job in a major teaching hospital has never set aside in-house time for research. The people who do research work a large amount of out of hours. I am unwilling to use family time for research’; and ‘The clinical load was dominant – research interests were regarded more as a hobby.’ Clinical practice in a private setting was cited as hindering participation in research: ‘No structure is available to be involved in research when working in private practice.’
Previous studies have revealed women's substantially lesser role in research compared to their male colleagues but few have examined specific factors that contribute to this imbalance [2], [13]. Our finding of the beneficial impact of a research-orientated professional ethos is echoed in the work of Haviland et al. [20] who established in both genders that exposure to research as a medical student was strongly associated with the intent to pursue an academic career. In a comprehensive study by Leibenluft et al. [4], the salience of a ‘microenvironment’ was referred to in an attempt to explain their finding that women child psychiatrists published more papers than either their men counterparts or women in adult psychiatry. In a study of paediatricians, less institutional support of women to conduct research was considered to contribute to the lower rate of women in the senior faculty [32]. By contrast, Mcginty et al. [22] reported that institutional factors encouraging pursuit of a research career relate to a preference in women for a nurturing environment, while availability of research activity or prominent researchers are rated as least important. Kaplan et al. [32] were more specific in positing that institutional support – protected time, availability of research assistants and support staff and access to research space – was rated as more pertinent by more academically productive women. Pincus et al. [21], [33] highlighted research training as the most prominent influence in both men and women psychiatrists.
Mentoring emerges as a cogent process in promoting research. Illustrative comments reflect this: ‘I've been exposed to a wonderful mentor. All hindrances can be addressed by a good mentor’; and ‘Good mentoring increases the chances that I will persist with research as it gives me a map, a pathway to follow and increased confidence.’ Conversely, non-researcher Fellows indicate that lack of a mentor hampered their pursuit of research: ‘I find it difficult to gain access to a mentor, more because of my part-time status than because of my gender’; and ‘It's mostly men who do research, and they are mostly interested in mentoring other men who are full time and furthering their career at all costs.’
Other investigators have demonstrated the influence of mentoring in fostering research among psychiatrists [33–35]. While this applies to men, it may pertain particularly to women, since they are traditionally underrepresented in positions of academic leadership [36]. El-Guebely et al. [13] found that although all researchers value the availability of a mentor, it is more so for women.
Opportunities to obtain mentoring may be reduced for women, given customary patterns of career disruption, part-time employment and resultant loss of professional affiliations. A common complaint from our respondents was: ‘Working odd hours takes you out of the mainstream and you miss out on the opportunities.’ Tesch et al. [10] found that women have fewer research networking skills and postulate that this underlies gender differences in academic ranks. A report by the American Association of Medical Colleges [12] concludes that because women encounter more difficulty in gaining mentors they have less access to information vital to career advancement.
The relative lack of women in prestigious academic positions probably exerts an undermining effect on junior women researchers as revealed by these quotes: ‘Female academic role models are few and male academics are poor models since they tend to be “workaholics” and rely on their wives to carry family responsibilities'; and ‘Few female mentors are available and those that exist are over-subscribed.’ Turner et al. [37] echo this pattern when positing that it is the absence of role models and subsequent lack of access to an informal network of professional support readily available to men that hinders women doctors' careers.
A third element distinguishing RG from NRG groups is research training. Several respondents stressed the undermining effect of its lack: ‘There is no training in how to do good research, only in how to recognize bad research’; ‘I don't understand the statistics and have felt intimidated’; and ‘No opportunity to piggy back on others’ research in order to learn.’ Pincus et al.'s [21], [33] findings support this observation in showing that psychiatric researchers – men and women – have been exposed to research as students. Similarly, Mcginty's [22] survey revealed that research participation during training is tied to a preference for an academic career. Shapiro and Mrazek [34], [35] found a strong association between research training and research involvement in both men and women.
Much to our surprise, RG and NRG members viewed family issues similarly. Although role strain is commonly cited as influencing the careers of women, the link however, has not been confirmed empirically, including in our survey [10], [38]. Valian's [25] comprehensive review of relevant work concludes that although women are less productive than men, those with children are not less productive than women without children. Childbearing and the corresponding demands of a young family invariably coincide with those of pursuing research, writing and establishing a clinical practice [10]. This underlies the usual hypotheses that family responsibilities account for gender differences in academic progress [18]. Three-quarters of both groups had children of equivalent age. Similar proportions were affected by the challenge of combining career and family, with no significant implications for research involvement. Other studies generate the same pattern. Leibenluft [4] queried the impact of motherhood on women's careers, finding that lack of a mentor was more problematic than lack of time. McGinty et al. [22] found that family pressures could influence career choices in women psychiatric trainees but no specific associations emerged. Turner et al. [37] referred to role strain but added the caveat that it is simplistic to attribute women doctors' impeded career development to reproductive function alone.
Limitations
Among the limitations of our investigation, the response rate of 56% raises the issue of sample bias. We have no way of identifying features of the non-responders since we opted for an anonymous survey. However, the sample size compared with most other surveys of this kind is substantial [22], [34], [35], [37]. Moreover, no other studies of women psychiatrists' views on factors influencing research involvement have been published. We did not seek data from men psychiatrists but then we did not aim to do so. Responses of a sample of men psychiatrists would be illuminating.
The self-report nature of the questionnaire is a limitation in that we did not provide a definition of research. This was deemed too difficult to achieve given the range of activities under this rubric, for example research degree, conceptual research, pilot study, and team-based research. Nevertheless, time dedicated to research, funding obtained and papers published are customary indicators of research activity.
The cross-sectional nature of the study provides a picture of factors women psychiatrists regard as hindering or facilitating research involvement at only one point in time. Should policy concerning training and research experience change, it would be informative to examine its effects and then compare the two sets of findings.
Implications
Do our findings offer any guide to elevating the proportion of researchers among women psychiatrists? Since the professional environment is pivotal, an ethos promoting curiosity about research and encouraging professional networks and intellectual stimulation is paramount. University departments of psychiatry have a responsibility to provide this kind of milieu. Even at a structural level, academic institutions can discourage women as this respondent implies: ‘The need to work part-time as many women do, makes them ineligible for many research posts.’ Offering short-term experience of research is an obvious corollary [1].
Another cardinal implication arising from our study is that university departments and co-ordinators of training programs should systematically incorporate opportunities for mentoring in a way that is readily feasible. Indirect mentoring through exposure to successful female researchers at workshops and conferences as well as in training programs could complement more direct forms [2], [12], [39].
Early exposure to teaching programs in research design and methodology is likely to appeal, especially if presented by teachers of both sexes. Providing opportunities to experience what it is like to be part of a research team, which includes women, would facilitate ‘hands on’ involvement (as well as indirect mentoring).
Child-rearing and the realities of family life are legitimate issues to be considered when planning recruitment and retention of women researchers even though role strain has not emerged as a cogent factor in our work or that of other investigators. Changes to customary career pathways could play a role. Measures to make allowance for interruptions would contribute to reversing the trend for women academics to progress much more slowly than their male colleagues [2], [3], [7]. As a respondent lamented, rigid policies are exasperating: ‘I received a junior researcher award. It all went down hill when l fell pregnant and had a child. My institution was unwilling to employ me in a part-time academic position.’ Valian [25] argues compellingly that it is the many and minor disadvantages of contemporary arrangements that buffet women academics and accumulate to generate substantial negative effects.
Fortunately, the picture may be changing with new approaches implemented in some institutions as part of equal opportunity programs [30], [39]. As Fried [29] claims, strategies to remove gender-based hurdles are feasible and can exert an enormous difference to women aspiring to enjoying academic pursuits.
Footnotes
Acknowledgements
We thank Tony Pinzone and Helen Evert for statistical advice, the RANZCP for a grant-in-aid and Helen Herrman, J. Kulkarni, Carolynne Marks and Michael Salzberg for their comments on an earlier draft.