
Abstract
Keywords
Although Kraeplin recognized many less severe forms of bipolar disorder than those hospitalized with manic depressive insanity [1], in recent times it was the observations of David Dunner which led to the modern conceptualization of bipolar II disorder [2]. In DSM-IV [3] the diagnosis of bipolar II disorder requires a history of major depressive episodes and of one or more hypomanic episodes. The critical criteria for a hypomanic episode is a period of at least 4 days duration of manic symptoms which do not lead to significant impairment, do not require admission to hospital and are not associated with psychotic features. Akiskal and other writers [4–6] have further expanded the bipolar concept, and this broader bipolar spectrum includes both bipolar II disorder and a wider spectrum of mood disorders with some bipolar features.
Since Dunner's description of bipolar II disorder there have been some studies comparing bipolar II patients with either bipolar I or major depressive patients. For instance, there is some evidence that bipolar II ‘breeds true’ [7–9] and may be associated with greater comorbidity both on axis I and axis II [10]. One area of clinical debate is the overlap of bipolar II disorder with cluster B, especially borderline personality disorder. Although clinicians may occasionally polarize the issues in this debate, DSM-IV would recommend that both diagnoses are made if patients meet criteria for both diagnoses.
In this paper on bipolar II disorder we utilize data collected in two clinical trials to examine relationships between bipolar II disorder and personality traits. These two clinical trials were conducted in our Clinical Research Unit [11] and were a randomised trial of fluoxetine or nortriptyline in outpatients presenting with a major depressive episode [12–15] (depressed sample), and a cognitive therapy trial in women with bulimia nervosa [16–20] (bulimic sample). Our objectives, utilizing data from both studies were: to compare the personality traits and disorders of patients with bipolar II disorder to patients with unipolar major depression; to examine the impact of a bipolar II diagnosis on the short and long-term outcomes of the patients in the two samples.
Methods
Full details of the assessment and treatment of these two clinical samples are available in other papers reporting on the Christchurch Outcome of Depression Study [12] and the Bulimia Treatment Study [16]. In brief, the depression study recruited 195 patients suffering from a current major depressive episode which required treatment with antidepressant medication. After the baseline assessment, the depressed patients were randomised to either fluoxetine or nortriptyline for an initial six-week antidepressant trial. Patients who improved with their initially prescribed antidepressant, continued with the same drug, but patients not responding to the first antidepressant prescribed had their medication changed. Patients continued to receive clinical care in the Clinical Research Unit for at least 18 months and follow-up will be for 5 years. The bulimia study recruited 135 women with current bulimia nervosa. Patients initially received eight sessions of cognitive therapy and were then randomised to a further eight sessions of exposure treatment with response prevention or relaxation (as a control). After completing the course of cognitive behaviour therapy, these patients were also followed up for 5 years following entry into the study [20].
Both studies were approved by the Canterbury Ethics Committee. While inclusion criteria were different and related to the presence of a current major depressive episode or current bulimia nervosa, exclusion criteria and key assessments were generally similar. Thus, across both studies, we attempted to minimize exclusion criteria, although patients with schizophrenia, bipolar I disorder, major medical illness, cognitive impairment and a primary diagnosis of severe alcohol or drug dependence were excluded.
In both studies, patients were assessed for axis I diagnoses with the Structured Clinical Interview for DSM-III-R (SCID) [21] and with the SCID-II [22] for personality disorders. Although there were different clinicians in the two studies, two psychiatrists (PRJ and PFS) were common to both studies and had central roles in clinical diagnostic training across studies.
Data from each study was entered into relational databases and transferred to appropriate statistical packages for statistical analysis. In this paper, the data were transferred to SYSTAT. Statistical analyses included t-tests and analyses of variance, with post hoc tests for dimensional data, χ2 tests or Fisher's exact tests (when appropriate due to small numbers) for categorical data.
Results
Personality traits and disorders
Depressive sample
The depressive sample consisted of 195 patients with a principal current diagnosis of a major depressive episode. At baseline, 19 (10%) also had a history of one or more hypomanic episodes. These 19 were generally similar to the remainder with major depression as regards age, gender, depression severity, melancholia, atypical symptoms and axis I comorbidity. The non-significant differences of note were lifetime rates of alcohol dependence (42% in bipolar II versus 29% in major depression), panic disorder (26% in bipolar II versus 14% in major depression), and of suicide attempts (47% in bipolar II versus 33% in major depression). The bipolar II patients had a significantly younger age of onset of depression (17.3 ± 9.4 years) compared to those with a single episode of depression (26.8 ± 11.3), but not compared to those with recurrent depression (19.8 ± 9.7).
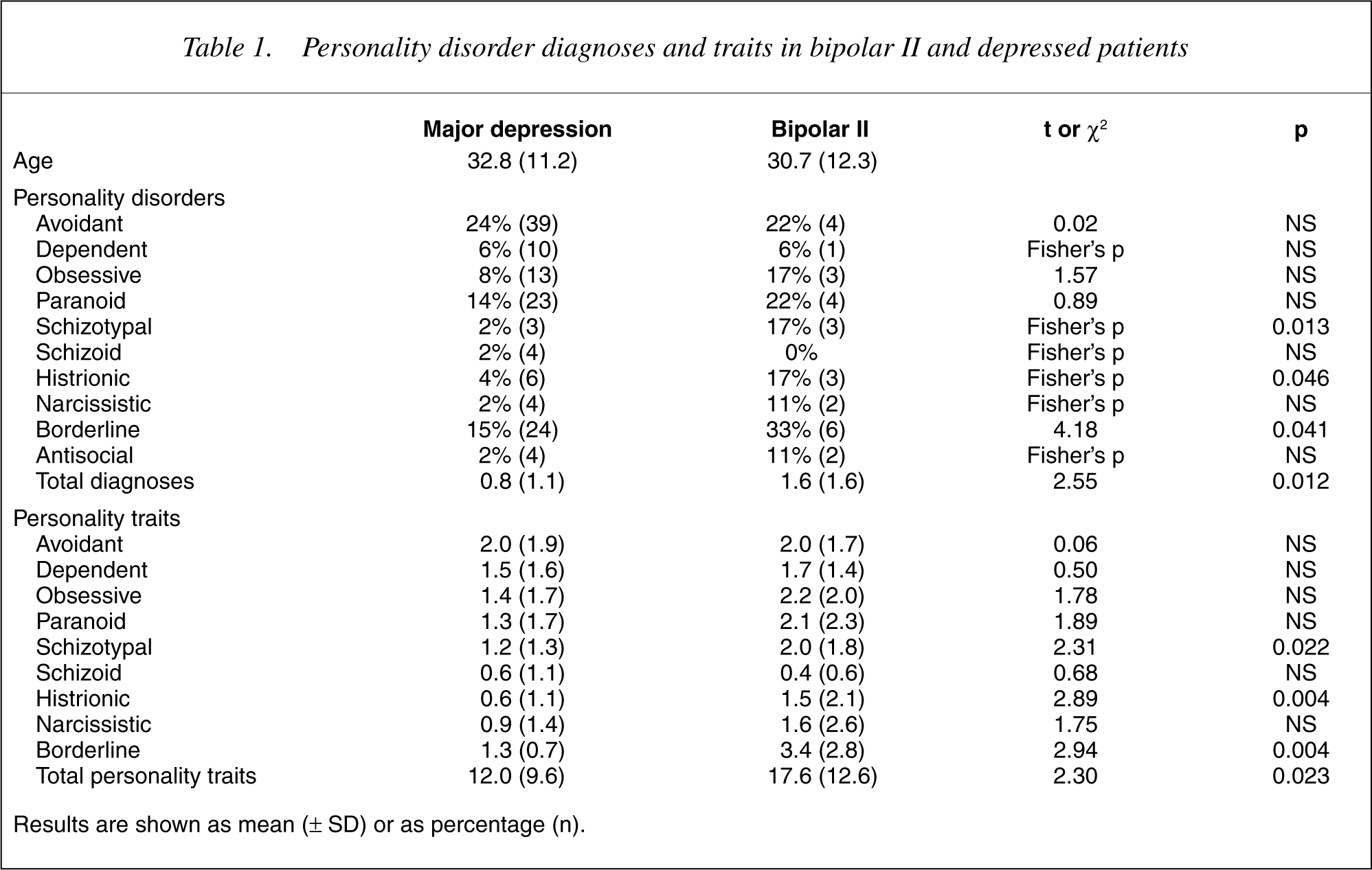
Table 1 shows the personality disorders and personality disorder symptoms (personality traits) of bipolar II and major depression patients. From this table it can be seen that the bipolar II patients have more personality disorder symptoms and diagnoses and have more borderline, histrionic and schizotypal symptoms and diagnoses.
Personality disorder diagnoses and traits in bipolar II and depressed patients
Bulimic sample
Table 2 divides the bulimic sample into three groups based upon their lifetime histories of major affective disorder, namely: no history of major depression; a lifetime history of major depression; or a lifetime history of bipolar II disorder. One patient who gave a clear history of recurrent hypomanic episodes, but who had no lifetime history of major depressive episodes, was excluded from these analyses. From Table 2 it can be seen that those bulimic women with any mood disorder versus no mood disorder had higher rates of avoidant personality disorder traits and diagnoses, higher rates of dependent traits, higher rates of paranoid personality traits and diagnoses, higher rates of schizotypal traits, higher rates of both histrionic and borderline personality disorder traits and diagnoses. In addition, those with any mood disorder had higher rates of total personality disorder traits and diagnoses.
Personality disorder diagnoses and traits in women with bulimia nervosa by mood disorder history
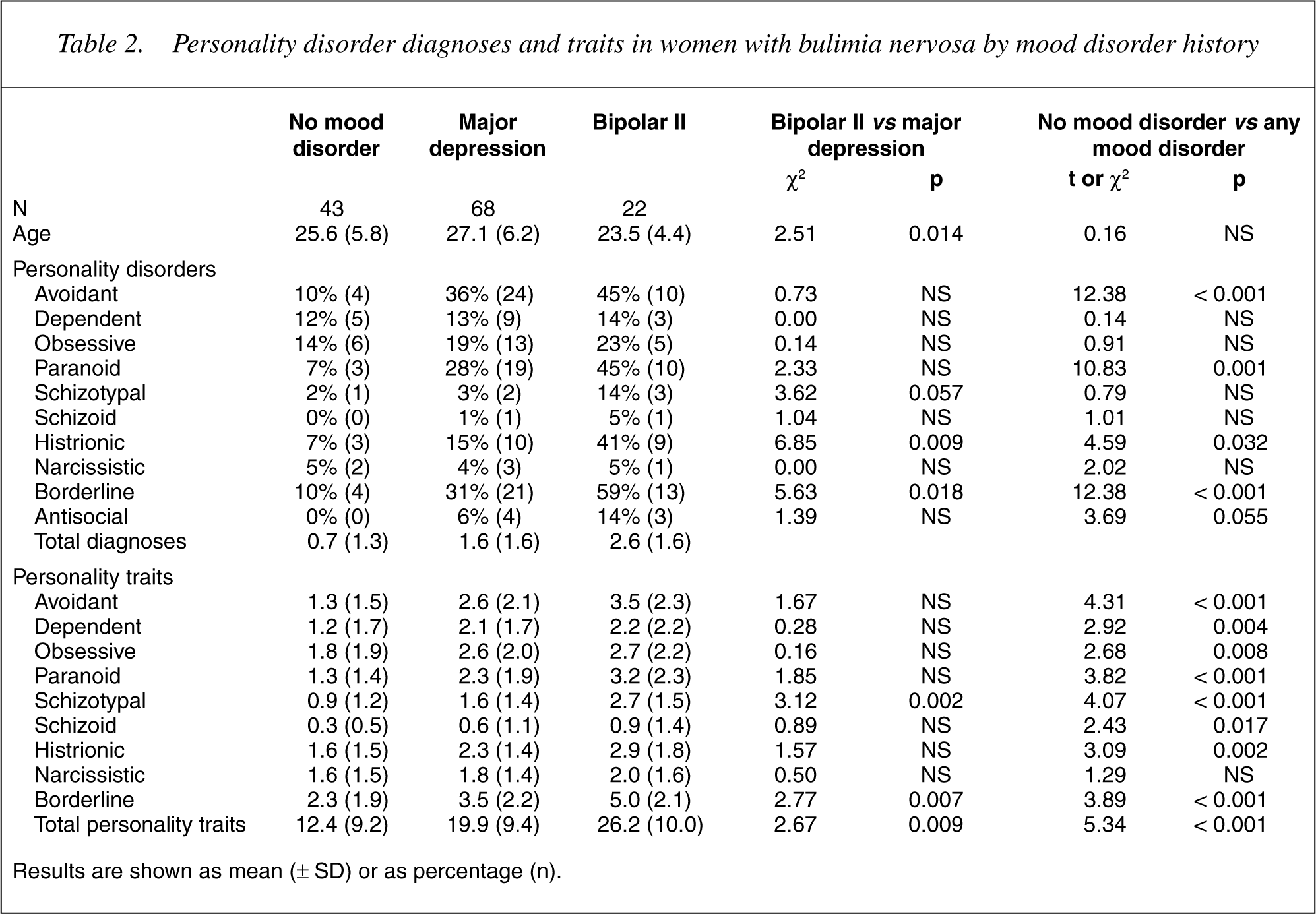
However, over and above the impact of any mood disorder, the bipolar II bulimic women had higher rates than major depressive bulimic women on histrionic and borderline personality disorder traits and diagnoses, and higher rates of schizotypal traits. In addition the bipolar II women had higher rates of total personality disorder traits and diagnoses.
Personality traits and the development of hypomania
In the depressive sample, nine patients who were diagnosed with major depression at baseline experienced a hypomanic episode during follow-up. Four of these patients had a hypomanic episode within 6 months of entry to the study, a further three by 18 months and a further two by 3 years. When these nine patients who developed hypomania (emergent bipolar II disorder) are compared to those who remained as having major depression on baseline personality traits, the emergent bipolar II patients had more schizotypal traits (2.6 ± 1.3 versus 1.1 ± 1.2, t = 3.25, p = 0.001). There were no suggestions that baseline histrionic or borderline traits predicted future hypomania.
Outcome
Depressive sample
Over the first 6 weeks of treatment, with either fluoxetine or nortriptyline, 63% (12/19) of bipolar II patients were classified as responders and 44% (78/176) of major depression patients were classified as responders. No patient developed a hypomanic (or manic) episode within 6 weeks.
By 6 months, one bipolar II patient (5%) and four major depression patients (2%) had experienced a hypomanic episode. At 6 months 71% (12/17) of bipolar II patients were without significant affective symptoms and 63% (100/159) of major depression patients were similarly symptom free.
By 18 months, 71% of both the bipolar II and major depression patients were free of affective symptoms. By this time only two bipolar II patients (11%) and seven major depression patients (4%) had experienced a hypomanic episode.
Bulimic sample
During the 5 years of follow-up, two patients developed a bipolar I diagnosiss. Both had been diagnosed as bipolar II at baseline. For one patient the manic episode occurred post-partum, and for the other patient, follow-up included hospitalization for both a psychotic depressive episode and a manic episode.
During the 5 years of follow-up, 55% of women with no history of a major depressive disorder or bipolar II disorder had a depressive episode, compared to 84% of those with a baseline history of major depression and 82% of those with bipolar II disorder. By 5 years 83% of women with no mood disorder history, 73% of women with major depression and 95% of bipolar II women no longer met criteria for any eating disorder diagnosis. In other words, only one (of 20 available for follow-up) of the bipolar II women with bulimia still suffered from any eating disorder.
Discussion
We have shown that across two clinical samples bipolar II patients differ from those with major depression on some personality traits; specifically the bipolar II patients have more borderline, histrionic and schizotypal traits. Furthermore, in the depressive sample, schizotypal traits predict future hypomanic episodes. Despite these differences in personality traits, we have shown that a bipolar II diagnosis at baseline has little prognostic significance. Thus, across the two samples, only two (5%) of the bipolar II patients developed bipolar I disorder, suggesting that a bipolar II diagnosis is relatively stable. This low rate of development of bipolar I disorder happened in the face of treating bipolar II depressed patients with antidepressant drugs, and without the protection of mood stabliser medication.
In the depressive sample 10% (19/195) met criteria for bipolar II disorder. This is lower than some writers on the bipolar spectrum would suggest [4–6]. However, in these studies a bipolar II diagnosis is limited to those with a four-day or greater hypomanic episode, as required by DSM-IV, and patients with briefer bipolar symptomatology remain in the major depressive disorder sample. Perhaps more surprising is the rate of bipolar II disorder in the women who sought help for bulimia nervosa. However, high rates of bipolar II disorder in patients with severe persistent eating disorders has been previously noted [23], and in bipolar patients eating disorder comorbidity is relatively common and is only surpassed by anxiety and substance disorder comorbidity [24].
The association between bipolar II disorder and borderline/histrionic personality traits is not surprising and is widely recognized [4],[25–29]. What is more contentious are the reasons for this pattern of comorbidity. We would suggest that these arguments will only be resolved when we know about the neurobiological basis of affective instability in both bipolar disorder and borderline personality disorder. However, one tentative explanation is that childhood and adolescent affective episodes increase the probability of developing a personality disorder (as currently defined). Thus there is growing evidence that childhood and adolescent disorders increase the risk for later personality disorders [30]. It is possible that childhood or adolescent hypomania specifically further increases the probability for a borderline/histrionic personality disorder. Indeed, in the bulimic sample all women who gave a history of one or more hypomanic episodes before the age of 15, also received a borderline personality disorder diagnosis. Furthermore, the observation that borderline/histrionic traits did not predict future adult hypomanic episodes in the depressive sample is consistent with the notion that it is childhood or adolescent hypomania which adversely impacts on personality development.
The association between schizotypal personality traits and bipolar II disorder has received relatively little attention, but was found in the NIMH Psychobiology of Depression Study, which was the first large study to examine the bipolar II diagnosis in detail [10], [31]. In the NIMH study they also looked at the characteristics of 48 patients who converted from major depression to bipolar II during an 11-year prospective follow-up. Predictors of future hypomanic episodes, based on selfreport, included mood lability, energy-activity and daydreaming. Furthermore, this group of bipolar II converters had high rates of substance abuse, educational, marital and occupational disruption and reported more minor antisocial acts prior to the development of discrete hypomanic episodes [32]. We do not have the equivalent measures, but have found that schizotypal traits predict future hypomanic episodes. Perhaps the analogy is too simplistic, but it is intriguing that psychotic symptoms in young people with depression predict future bipolar I disorder [32–35], while subsyndromal psychotic symptoms (schizotypal features) predict future bipolar II disorder.
Across these two clinical samples only two (5%) of 41 bipolar II patients developed bipolar I disorder. In the NIMH Psychobiology of Depression Study the bipolar II patients also seldom developed bipolar I disorder [36]. The stability of a bipolar II diagnosis during follow-up is also consistent with family study data, which suggests that bipolar II ‘breeds true’ [7–9]. The importance of this for clinicians is that future manic episodes are unlikely and that prophylactic anti-manic or mood stabliser drugs may not be necessary in most bipolar II patients. Indeed in our depressive sample, the majority of our depressed bipolar II patients had satisfactory treatment outcomes with antidepressant medication alone.
A further important finding from this study is that in both clinical samples, a bipolar II diagnosis was not associated with a poorer treatment outcome. Indeed, in the depressive sample the non-significant trend is for bipolar II patients to have marginally better responses to their initial antidepressant and at 6 months. However, our findings need to be considered in the light of data on the long-term outcome of bipolar II disorder reported in other studies, such as the NIMH Psychobiology of Depression [37], where bipolar II patients spent approximately 50% of prospective weeks with depressive symptomatology. At 6, 18 and 36 months we have only reported on the likelihood that a patient is free of symptoms rather than the cumulative time unwell. However, our data does not find that the bipolar II patients are less likely to be well than the major depression patients. Similarly, response of the bulimic sample to cognitive behaviour therapy was not adversely affected by a mood disorder history. Perhaps of greatest note is the high rate of prospective depressive episodes during follow-up of the bulimic sample; not surprisingly this is most marked in those who gave histories of depressive episodes (with or without a history of hypomania) at the time of entry to the study.
All studies have limitations and the results should be interpreted with this in mind. The first key issue relates to the diagnosis of hypomanic episodes. In these studies the key diagnostic instrument was the SCID, and using DSM criteria, a hypomanic episode required a minimum duration of 4 days. Thus, we have not coded as bipolar II any patients with briefer hypomanic episodes, or those who show mixed mood features during depressive episodes. Furthermore, the diagnosis of past hypomanic episodes has relatively low reliability. Thus, on the basis of one interview patients may not give a history of hypomania, which they may give during a second interview. However, obtaining the history on even one occasion is probably valid, as such patients have excessive bipolar relatives. Thus, a hypomanic episode on one interview has low sensitivity but high specificity [38]. Both of these factors suggest we may have underestimated the extent of bipolar spectrum disorders in these samples. However, underestimation would not invalidate the results presented here. Similarly, during follow-up, untreated hypomanic episodes may have been underestimated, but it is unlikely that we have missed any patients hospitalized for mania. Thus, if the extent of bipolar spectrum disorders in these samples has been underestimated, the rate of conversion to bipolar I disorder is likely to be even lower than the 5% conversion rate observed.
Bipolar II disorder is an extremely interesting disorder which has both similarities and differences with both major depression and bipolar I disorder [31]. In this study we have highlighted the higher rates of borderline, histrionic and schizotypal traits in bipolar II patients compared to those with major depression. Furthermore, only a small minority of bipolar II patients became bipolar I during follow-up, and thus the use of prophylactic anti-manic or mood stabliser medication is only occasionally indicated. Finally, a bipolar II diagnosis was not associated with a poorer treatment outcome, whether treating patients in a depressive episode with antidepressants or treating women with bulimia nervosa with cognitive behaviour therapy.
Footnotes
Acknowledgements
These studies were funded by the Health Research Council of New Zealand. We thank Isobel Stevens, Robyn Abbott, Leslie Livingston and Andrea Bartram for their assistance.