
Abstract
In most non-Western cultures, there are two interpretations of altered states of consciousness (ASC). First, they are interpreted as states of possession in which a supernatural entity acts through the possessed individual. Second, they are conceptualized as a special state of the individual allowing close interaction with supernatural entities, such as perceiving them in visions, receiving their messages, and imitating their actions [1]. These two basic variations of culturally defined ASC have been designated possession-trance and trance, respectively.
It is important not to ‘pathologise’ certain cultural processes or trivialize the communicative value of trance states [2]. Some Hindus are able to dissociate through the use of meditative trance, thus creating a divided consciousness and gaining the ability to directly experience the deities of their religion. Because this special state of consciousness is so highly valued in Hindu culture (self-realization being the goal of the religion), the actual lived-experience is one of mild euphoria, and does not involve social or occupational impairment [3]. Particularly in cultures where possession trances are relatively common, it is very important that they are not wrongly diagnosed and treated inappropriately, for example, as a psychotic disorder.
Stephen and Suryani focus on traditional healers (balian) in Bali, Indonesia, to raise new arguments concerning the nature of the initiatory sufferings reportedly experienced by shamans in many cultures [4]. They point to a grey area wherein Western cultural assumptions about ego boundaries and hallucinatory experience has led to a pathologizing of experience which other cultures continue to value and foster.
DSM-IV has included dissociative trance disorder (DTD) as a subcategory of dissociative disorder not otherwise specified (DDNOS) to accommodate dissociative disorder that occurs in specific cultural contexts and involves ‘an involuntary state of trance that is not accepted by the person's culture as a part of a collective cultural or religious practice and that causes clinically significant distress or functional impairment’ [5]. Trance syndromes can be distinguished from possession trance syndromes, which are characterized by the replacement of the primary personality by a new identity, usually a ghost, demon, or deity. There are phenomenological differences between these two dissociative forms as well. The behaviour of persons with possession-trance syndromes is usually more complex, with a more complete alternate personality whose behaviour follows pre-established cultural patterns.
Situated at the tip of the peninsular West Malaysia in South-east Asia, Singapore is a multiracial society with a preponderance of Chinese (77.7%) over the other ethnic groups: Malays (14.1%) and Indians (7.1%). The ethnic composition has remained stable in the last decade. Trance behaviour is deeply rooted in our cultural and religious history [6–10]. For instance, belief in spirit possession remains fundamental in the Chinese religious belief system. A blend of Confuciansim, Buddhism and Taoism emphasizes balance with persons and nature, while a larger universal context for harmony includes ancestors, gods and spirits in addition to people and social institutions. The temporary possession by a shen (god) of a man or woman, is not uncommon in Singapore, and is found particularly among people of the Hokkien dialect group. People so possessed are called tang ki; they are not necessarily full-time priests and are often people having ordinary employment outside the hours set for medium performances [11]. Most temple mediums in Singapore are youths in their early twenties, although there are middle-aged exceptions. Assistants at the temple do not usually become entranced but perform the role of an interpreter in a normal state of consciousness. To meet this requirement, an assistant must be thoroughly familiar with the unique demands of mediumship [7]. The majority of people that go to medium performances are Chinese.
Many authors have studied the impact of psychosocial stressors on conversion and dissociative disorders [12–15]. Emotional stress also has been considered by patients as being significant in evoking an attack of possession-trance [14]. Ward and Beaubrun demonstrate that possessed individuals have higher levels of neuroticism and hysteria than controls, which they argue support the notion that the onset and duration of possession might be interpreted as induced by stress [15]. Ng et al. found that subjects with personality traits like nervousness, excitability, and emotional instability were more likely to have a higher frequency of trance states [16]. Following repeated attacks, subjects may develop a susceptibility to further attacks of trance when exposed to culture-bound stimuli, which include witnessing an exorcism ceremony, or possession state of another [14]. Inevitably, each person's experience of events is unique and is responsible for a unique susceptibility. An understanding of the precipitating psychosocial stressors that overwhelmed the patient's coping abilities would have implications for treatment by enabling the clinician to devise strategies for intervention and prevention. The aims of the present study are essentially threefold: (i) to identify the types of psychosocial stressors that precipitate DTD in Singapore; (ii) to compare the results with a group of patients with major depression seeking help at the same psychiatric hospital to see if the types of stressors differ between the two groups; and (iii) to determine the impact of the demographic and background factors on DTD.
Materials and methods
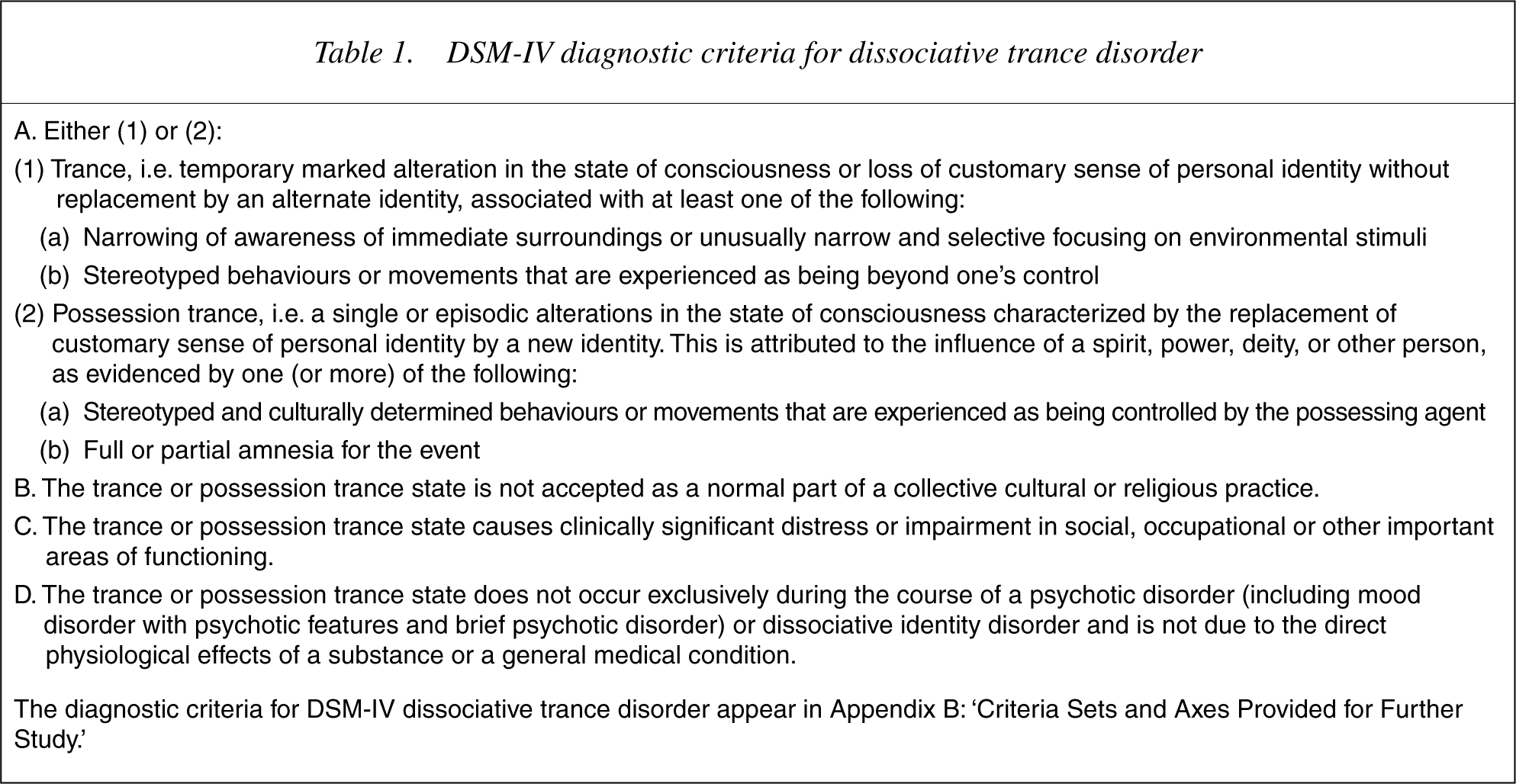
This is a study of consultations at Woodbridge Hospital, the only state psychiatric institute in Singapore. The hospital admits about 1000 new cases a year, while there are about 4000 re-admissions annually. Consecutive cases seen at the psychiatric hospital diagnosed with DTD were included in the study. The psychiatric diagnosis, assigned on the basis of information obtained in a semistructured psychiatric interview and hospital chart review, were made according to DSM-IV criteria (see Table 1).
DSM-IV diagnostic criteria for dissociative trance disorder
The patients were interviewed by one investigator (the first author) after the acute episode of trance state had resolved. Information was collated using a specially prepared protocol, with particular attention paid to their demographics, extent of prior involvement in trance states, and the presence of psychosocial stressors. The interview focused generally on the subjective experience of the affected individual. Assessments were carried out in the hospital, at the outpatient clinics, or at patients' homes.
We opted for the interview rather than the checklist approach to the assessment of major life stressors, as the former has the potential to provide far richer data than the checklist measures [17]. Stressors here refer to ‘specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person’ [18]. A psychosocial stressor is one that occurred in the minutes to weeks before the onset, recurrence, or exacerbation of the disorder. The interviews include probe questions that can be used to screen each important area of the patient's life in which events may have occurred. If an event is reported, enough detail is obtained to assess the impact of the event on the individual and to obtain a reliable date. Detailed questioning is done to date the onset of symptoms and only stressors that precede the trance state are counted [19]. The interview inquired about: the onset and temporal course of trances; education; military and vocational experiences; interpersonal and sexual relationships; family relationships; current economic situation; medical history; and forensic history. We looked for current life contexts that often contribute to stress or conflict. Families may be helpful sources of such information. Subjects also were asked why they thought they were having trances. We also provide the respondents with a calendar with holidays and birthdays of the respondents to help subjects’ memories. Accurate dating of events allows for the investigation of time elapsed since the occurrence of events as a predictor of disorder [17].
The interviews were conducted separately and patients were assured that their possible refusal to take part would not have made any impact on their management. The study was approved by the hospital human subjects review board and the subjects participated voluntarily after informed consent was obtained.
All in all, 58 cases were included in this study. Table 2 lists some of the demographics and other features. Ten patients with DTD received only outpatient treatment. The assessments were done at the hospital, outpatient clinics, and/or the patients' homes. For comparison, we examined the stressors encountered by a group of patients with major depression seeking help at the same psychiatric hospital and matched for age, gender, race and education. For statistical analysis, χ2 was applied to test for significant differences between categorical variables. All tests of significance were two-tailed. The significance level was set at 0.05.
Profiles of patients
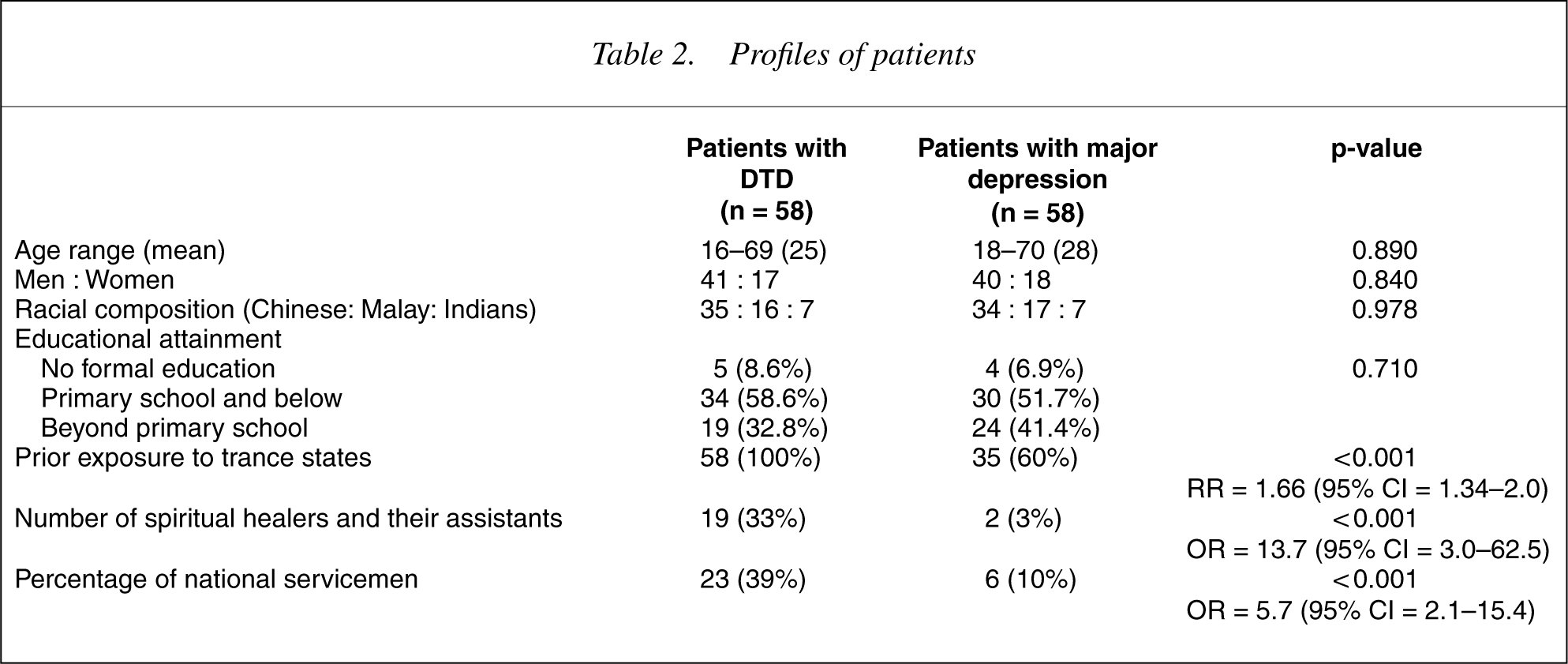
Table 2 demonstrates lower levels of activities among patients with MD than in those with DTD (e.g. lower previous exposure to trance states, less involvement in spiritual activities and lower enrolment in the military service). This could have influenced the groups differently, and could be responsible for the overall observation. Logistic regression was used in this situation where a number of variables significantly influenced the differences between the two groups.
Results
In all, 58 patients with DTD were studied. With regard to types of alternate embodied identities, 25 (43.1%) subjects were reported to be possessed by Buddhist and Taoist deities, five (8.6%) by departed relatives and ancestral spirits, three (5.2%) by Hindu deities, three (5.2%) by animal spirits, two (3.4%) by the Holy Spirit, and 20 (34.5%) by other spirits. The duration and intensity of trance varied considerably. Most attacks were brief, lasting 15–30 min. It was not uncommon for subjects to fall in and out of trances several times within the episode. An episode of possession trance frequently comprised many subsequent shifts and the whole episode might last for days. The extent of prior involvement in trance states was also examined: 16 (27.6%) were spiritual healers, seven (12.1%) were assistants to healers, nine (15.5%) had experiences with altered states of consciousness, while 26 (44.8%) had witnessed trances before.
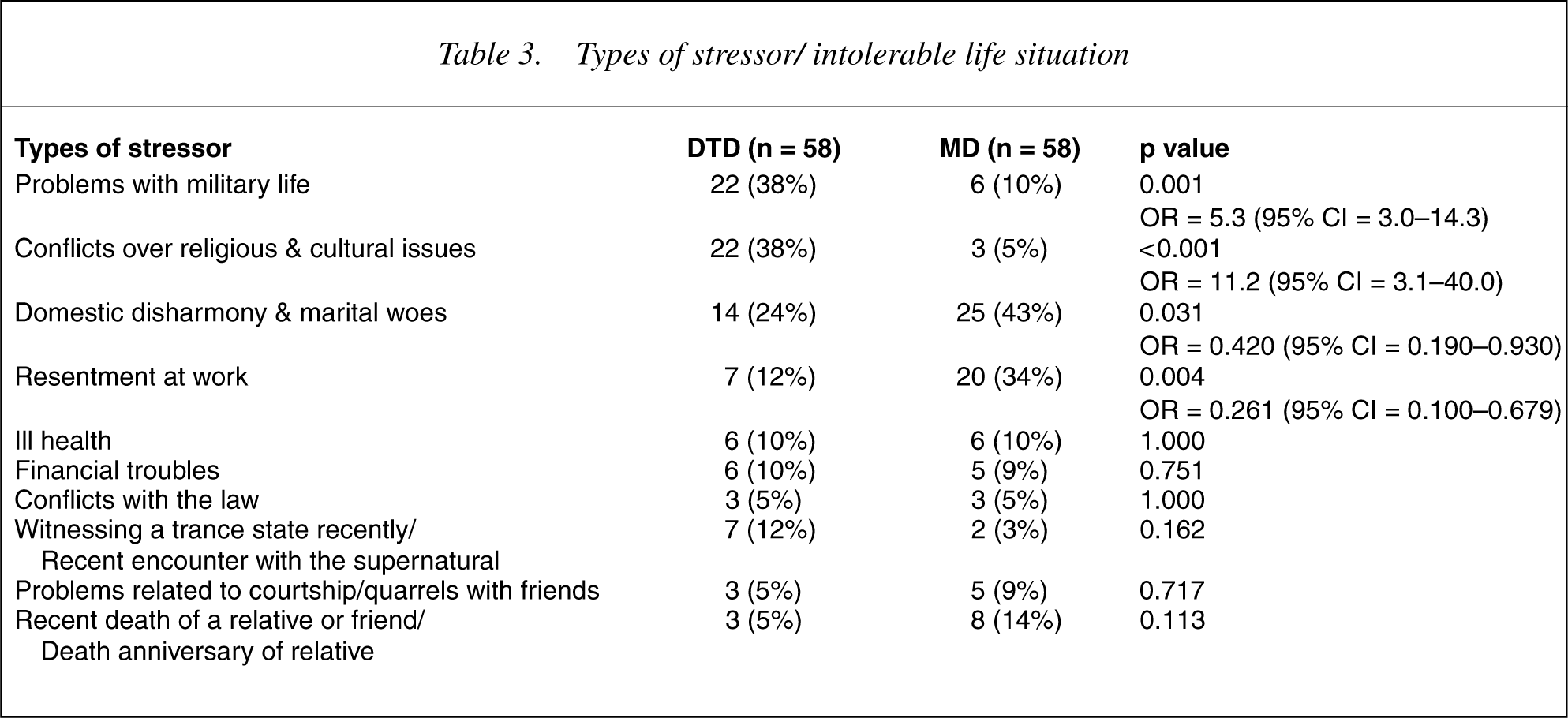
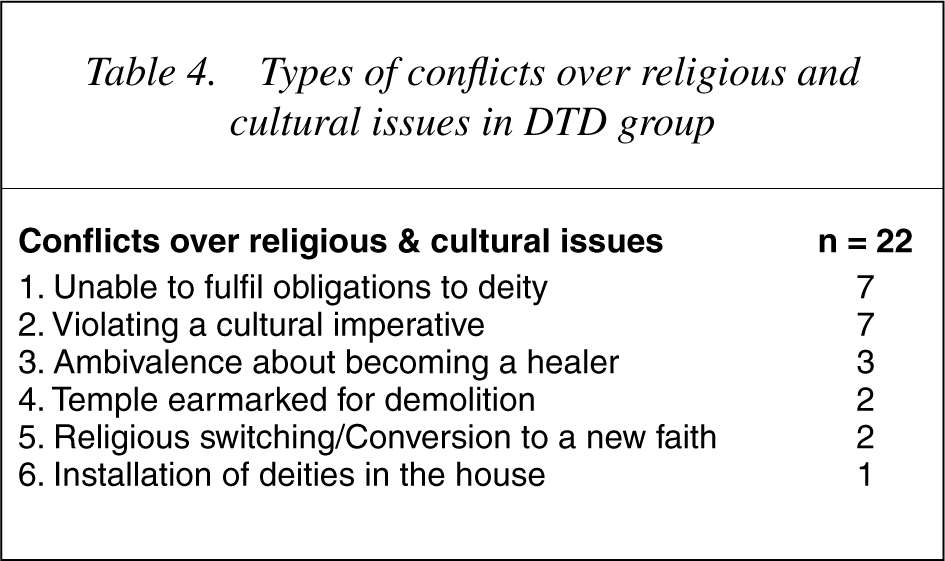
All the cases with DTD were characterized by the presence of psychosocial stressors, whereas this was the case in 80% of patients with major depression. An individual may experience multiple stressors; each stressor is considered and hence, the total in Table 3 exceeds 100%. Subjects often experienced more than one category of event as an immediate precipitant. For patients with DTD, 30 patients have only one stressor, 21 patients experienced only two stressors and seven patients reported three stressors. Common stressors for the DTD group include problems with military life (38%), conflicts over religious and cultural issues (38%), and domestic disharmony and marital woes (24%) (see Table 3). Table 4 shows the types of religious and cultural conflicts. Domestic disharmony and marital woes were also commonly reported by the group with MD.
Types of stressor/ intolerable life situation
Types of conflicts over religious and cultural issues in DTD group
In our series there were seven temple mediums who were not able to perform for their deities following enlistment into military service. The following case history can be used as an illustration: a soldier developed a trance state in the military camp soon after he was refused permission to return to the temple to participate in the consecration ceremony. The ceremony is a vital one as it enthrones and locates the deity within the temple grounds. The soldier was extremely frustrated because his request was not granted despite the pleas of 20 of his friends from the temple. His behaviour was in keeping with the cultural belief among some Chinese that a deity may punish a medium for disobeying instructions or when a medium terminates his service.
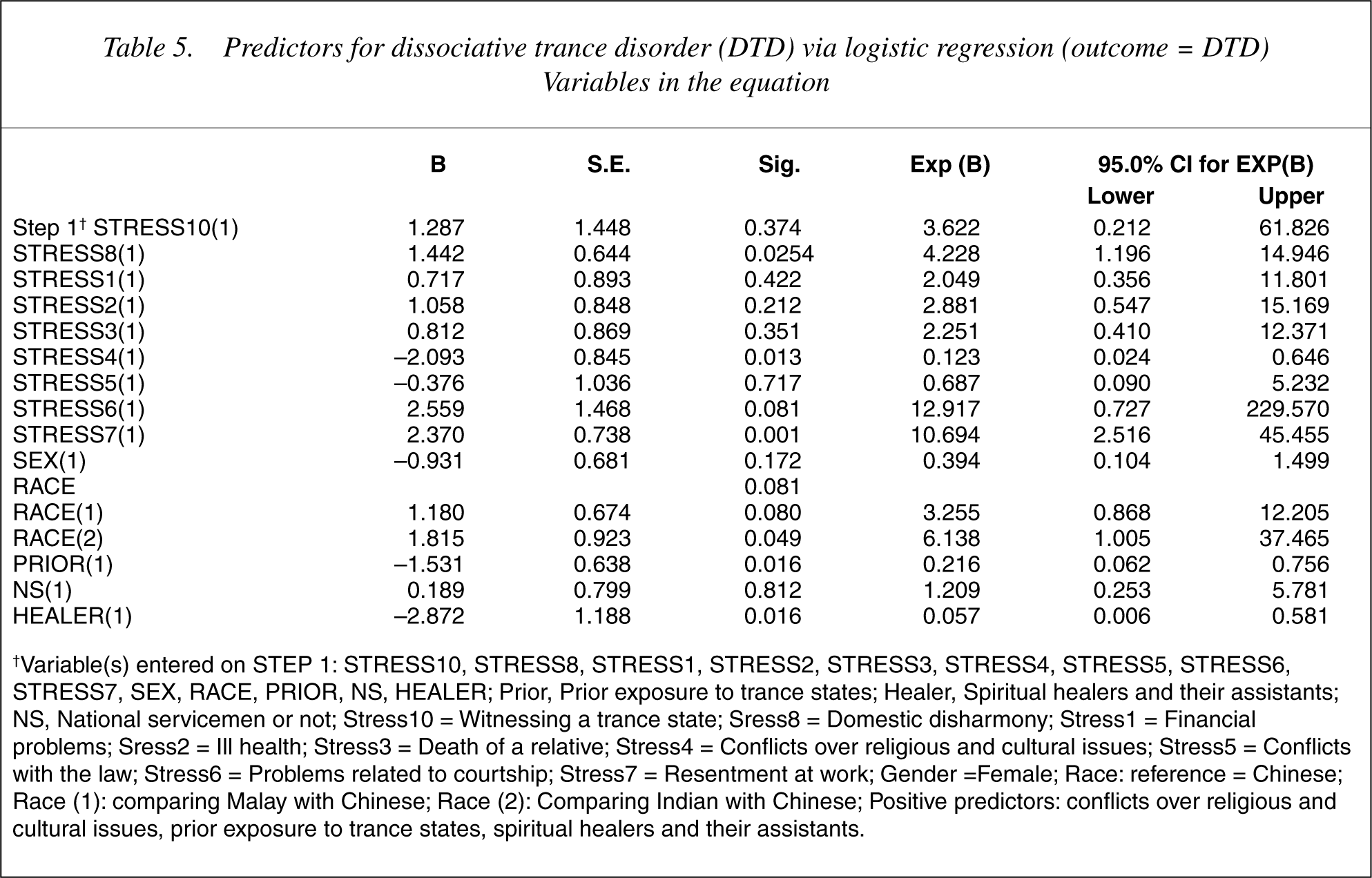
Those with DTD were more likely to have prior exposure to trance states (p < 0.001, OR = 1.66, 95% CI = 1.34–2.0). The group with MD was more likely to be non-national servicemen (p < 0.001, OR = 5.7, 95% CI = 2.1–15.4). Those with DTD were more likely to be spiritual healers and their assistants (p < 0.001, OR = 13.7, 95% CI = 3.0–62.5). The group with DTD was more likely to have problems with military life (p = 0.001, OR = 5.3 CI = 1.9–14.3), and more likely to encounter conflicts over religious and cultural issues (p < 0.001, OR = 11.2, 95 CI = 3.1–40.0). Logistic regression reveals that the following are positive predictors for DTD: conflicts over religious and cultural issues; prior exposure to trance states; and being a spiritual healer or an assistant to one (see Table 5).
Predictors for dissociative trance disorder (DTD) via logistic regression (outcome = DTD) Variables in the equation
Discussion
The predominance of national servicemen among the DTD group merits some mention. An entranced soldier would be sent to the public psychiatric hospital for observation and treatment. This is an attempt to discourage him from further trance states, to avoid empowering him within the environment, to limit the impact of the trance in the military setting and to prevent the occurrence of a mass hysteria. If the individual was not a soldier he could have sought help from the traditional healers instead and might not have been captured by the study framework.
The precipitant of trances may not be obvious. Some generally cannot be understood without exploration of the patient's life history and current life context. In this study many of the national servicemen with DTD reported problems with military life. Healthy men in Singapore have to perform at least 2 years of national service at the age of 18. The stint may sometimes be deferred for a few years for academic pursuits. Following enlistment into full-time national service, one's usual social support system is not readily available. As most camps are relatively distant from homes, with one in the offshore island, Pulau Tekong, the soldier's sense of isolation can be intensified. Separated from his relatives and friends, and in the absence of firm emotional support, the conscripted serviceman may experience a strong need for solace and comforting objects. It is possible that the mystical quest in trance states represents a search for comfort, peace and tranquillity. Military recruits may also need help to cope with the complex psychosocial and transactional challenges of national service.
It is possible that role conflict is another type of stressor, but the evidence here is anecdotal. Role conflict has been defined in a number of ways in the literature, although most definitions distinguish intrarole conflict from interrole conflict. The former exists when a person in a particular role position is confronted with incompatible expectations for his/her performance in that position, while the latter exists when a person occupies two different roles that have conflicting expectations for behaviour [20]. For Chinese temple mediums who were conscripted into military service, they have difficulty fulfilling their obligations to their gods or deities – an example of interrole conflict. The Chinese believe that a deity may punish a medium for disobeying instructions, for example, for having become impure in some ways or when a medium terminates his service. The local psychiatrists would recommend that they make arrangements to continue serving the gods after completion of their military stint.
This study also finds violation of cultural imperatives an important psychogenic precipitant. In traditional magic, it is humans and the intentions of humans that drive the intangible forces that transversely influence the actions of humanity [21]. Sickness is seen as a punishment by the gods for the breach of religious prohibitions or social taboos that have divine sanctions. The breach may be unintentional [22]. Malays need to observe certain taboos, violations of which are believed to result in punishment from God, for example, by making the individual entranced. The Moslems have many taboos and the ritual avoidance of pollution is exhibited. For instance, the Chinese and Indians in Singapore generally do not have as severe religious prohibitions against consuming alcohol as the Malays have [23]. The Islamic prohibition of alcohol is essentially based on its interference with the mind (the power of judgement). Thus the Malays in Singapore experience most guilt about their drinking compared to the other races even though they drink the least [23].
Almost half the cases of DTD reported two or more stressors. This is understandable given that important events often lead to other events. Chains of related events tend to cluster within a relatively short period of time. Coping resources may be overtaxed when events cluster in time [17].
In the absence of studies on DTD with systematic data collection, even anecdotal data on a dataset of this size should be considered impressive. This study is an attempt to ‘quantify’ narrative, observational data, and the results are clinically meaningful. However, being a hospital-based study, the sample of patients could not be considered representative of the general population. It has been recognized that a patient sample is often biased by social selection factors and by the reason for the consultation. With regards to the ‘psychogenic precipitants’, some of them (e.g. problems with military life) may be over-estimated and cannot be generalized due to sample bias. It is not clear whether the DTD patients are not capable of coping with what might be ordinary life stressors or that the level of certain stressors is higher in this group of patients thereby precipitating their disorder.
Psychological interventions subsequently focused on specific stressors and longstanding adjustment problems according to the individual needs of each patient. Goals of therapy included enhanced crisis management skills, reduced concern about the trance episodes themselves, and reinforcement of constructive problem-solving behaviour. Through an analysis of the timing and frequency of the trance episodes, patients became aware of the relationship between stress and dissociative episodes. The aversive and desirable consequences of adopting more effective and assertive responses to persisting interpersonal stressors (marriage, family, work) are also explored. Treatment for DTD takes time. The patient must be given aegis. Patients and their families are advised that dissociative episodes may continue for a time, but once a more effective and culturally acceptable coping strategy has been initiated, they will eventually disappear.