
Abstract
Women's mood during pregnancy and postpartum is mediated by a range of personal, psychological, biological, social, cultural and economic variables. While disturbed mood is characterised by a number of different states including anxiety, anger and depression, it is the latter that has been most extensively investigated.
The period following childbirth is a particularly vulnerable time for the onset of depression [1,2]. The prevalence of postpartum depression is estimated to be between 8% and 20%, depending upon the timing and method of assessment [3–7]. Personality factors positively associated with postpartum depression include neuroticism [4], external locus of control [8] and interpersonal sensitivity [9]. Inadequate partner support [4,5,9–11], stressful life events [12] and operative obstetric intervention [13–16] have also been significantly linked with postpartum depression.
Antepartum depression has not been as well characterised as postpartum depression, but the prevalence is estimated to be 4–9% [1,3–5,7,10,11]. Factors associated with depression during pregnancy include inadequate partner support [4,5,10] and ambivalent feelings about having the baby [5]. The presence of antepartum depression has been identified as a predictor of postpartum depression [6,12,17].
There is a well-documented relationship between socioeconomic factors and health. Socioeconomically disadvantaged groups generally have poorer physical and mental health than their more advantaged peers [18–25]. However, studies investigating the association between socioeconomic factors and psychological health during pregnancy and following birth have reported contradictory findings [4,5,8,13,15,26,27].
Information regarding the relationship between socioeconomic status and mood disturbance during pregnancy and following childbirth among Australian women potentially assists health planners and service providers to direct prevention strategies and treatment programs appropriately.
In this study private health insurance was assumed to be an indicator of socioeconomic advantage. In 1984 approximately 50% of the Australian population were covered by private health insurance, compared with only 31.6% in 1997 [28]. Between 1984 and 1996 private insurance premiums increased, in real terms, between 58% and 173%, leading to a decline in affordability, particularly among lower income groups [28]. Income is a strong predictor of private health insurance. Only 23% of people in income units with a gross annual income under $20 000 had private health insurance in 1995, compared with 72% of people in income units with a gross annual income over $70 000 [29].
It was hypothesised that the ante- and postpartum mood of private patients would be more positive than that of public patients. Additional variables potentially associated with mood during pregnancy and following birth were measured including: age; the women and their partner's employment status and level of education; number of children; previous birth experiences; personality traits; and perception of partner support.
Method
A longitudinal, prospective study of the psychological aspects of the childbirth experiences of multiparous women in Melbourne was undertaken by Jane Fisher and commenced in 1994. Three hundred and twenty women were recruited in the early stage of pregnancy via the print media and from hospital booking and obstetricians' lists. The main objective of the study was to investigate the impact of obstetric interventions on postpartum mood (the findings related to this objective will be published elsewhere). These longitudinal data were used to investigate the relationship between health insurance status and mood during pregnancy and following childbirth.
Women who volunteered to participate in the study were contacted by telephone and surveyed on five occasions: during each trimester of pregnancy and at 2 and 8 months following birth. On entry to the study demographic information was recorded and a detailed obstetric history taken. The women were classified as private patients if they were receiving private or shared care in a private hospital, and as public patients if they were attending a public clinic in a public hospital or were participating in a shared care arrangement at a public hospital. Women having homebirths (n = 6) were coded as public patients.
Psychometric assessment
A range of standardised, valid, self-administered psychometric tests were used to assess the following factors: mood (including measures of anxiety and depression); locus of control; defence style; and partner support. Psychometric tests were posted out to participants who returned the completed forms to the researchers in a reply-paid envelope.
The personality traits of locus of control and defence style were assessed during the first trimester of pregnancy. Levenson's Locus of Control (LOC) scale is a validated and reliable instrument that assesses the extent to which individuals attribute the cause of events to themselves (internal control), powerful others or chance (external control) [30]. Relatively high scores on the internal control dimension and low scores on the external control dimension tend to be associated with psychological wellbeing.
Defence style is a psychological construct that characterises the way in which individuals respond to anxiety-provoking situations such as pregnancy and childbirth. A hierarchy of defences derived from psychodynamic theory are classified as mature, immature or neurotic [31]. A predominantly mature defence style is associated with psychological health, while predominantly immature or neurotic defence styles are associated with psychological morbidity. Assessment of defence style is a relatively recent development in psychometric testing and, consequently, the instruments are still evolving. The Defense Style Questionnaire (DFQ) used in this study was designed by Andrews, Pollock and Stewart (1989) [31] who adapted it from the work of Valliant and Bond [32].
Partner support was measured during the first trimester of pregnancy and 2 months postpartum using the 24-item Intimate Bond Measure (IBM) of Wihelm and Parker (1988) which assesses two fundamental dimensions of intimate relationships: how caring and how controlling the respondents perceive their partners to be [33].
Mood was assessed using the Profile of Mood States (POMS) developed by McNair, Lorr and Droppleman (1981) which measures six identifiable mood or affective states (tension-anxiety, depression-dejection, anger-hostility, vigour-activity, confusion-bewilderment, fatigue-inertia) [34]. It consists of a checklist of mood-related adjectives derived through a factor analytic process. The higher the POMS score, the greater the disturbance in mood. This applies to both the total score and those of the individual affective states except vigour-activity. The higher the vigour-activity score, the greater the level of the positive attribute of vigour. The POMS questionnaire was administered during each trimester of pregnancy, and 2 and 8 months postpartum.
All data were entered into a database and analysed using Statistical Package for the Social Sciences (SPSS; SPSS, Chicago, IL, USA) Version 8.0. Statistical procedures included t-tests, chi-squared and odds ratio. Stepwise linear regression and repeated measure ANOVA were the statistical procedures employed for multivariate analyses.
The project was approved by the institutional ethics committee of the University of Melbourne.
Results
Demographic, personality and obstetric differences
Of the 320 women originally enrolled in the study, 12 (4%) had a spontaneous or induced abortion (for foetal abnormality), four (1%) withdrew during pregnancy and eight (2%) withdrew postpartum. Thus, 296 women (92.5%) remained in the study until the completion of data collection. The mean age of the women was 31.9 years (range = 21–41 years). During the current pregnancy 54.7% (n = 175) were treated as private patients (members of a health insurance fund) and 45.3% (n = 145) as public patients. Most of the women (61%) had one child, 29% had two, 9% had three and less than 2% had four or more children (prior to the current pregnancy).
Private patients compared with public patients were older (32.7 years cf. 31.0 years, p < 0.001) and had fewer children (2.4 cf. 2.7, p < 0.005). They were more likely to be tertiary educated, in a legal marriage and to have a partner who was tertiary educated and employed full-time. Additionally, they more frequently had a caesarean section for their first delivery (Table 1). There were no significant differences between private and public participants on any of the personality measures (defence style or locus of control) or the measure of intimate bonds as assessed at study entry.
Demographic and obstetric differences between private and public patients
Compared with women giving birth to their second or subsequent child in Victoria during 1995, the study group were older [mean = 31.9 years (95%CI = 31.7–32.4) cf. 30.3 years] and more likely to be Australian born (87.1% [95%CI = 83.4–90.7] cf. 74.5%) and married (92% [95%CI = 89.1–94.9] cf. 82.3%). Fewer women having their second or subsequent child in Victoria in 1995 had a caesarean section (9.2%) compared with women in the study group (19.1%; 95%CI = 14.8–23.4) [Perinatal Data Collection Unit, Department of Human Services, Victoria: correspondence]. Thirty-five per cent of Victorian women aged 20–40 years were reported to have private health insurance in 1995, considerably fewer than in the study group (54.7%; 95%CI = 49.3–60.1) (Mike Langan, National Health Survey: personal communication). The study participants were more likely to be tertiary educated (62.2%; 95%CI = 56.9–67.5) compared with Australian women generally (34%) [35].
Pattern of mood during pregnancy and following birth
A distinct pattern of mood change across the duration of pregnancy was identified. Mood was at its worst during the first trimester of pregnancy, improved during the second trimester, and then declined in the third trimester to a level similar to that observed during the first.
The public patients returned a consistently higher POMS score during all three trimesters of pregnancy compared with the private patients (Fig. 1). However, this difference only reached statistical significance during the second (p = 0.05) and third trimesters (p = 0.02). The scores on the subscales of anger-hostility, confusion-bewilderment, tension-anxiety and depression-dejection consistently contributed to the differences observed on these two occasions (Table 2).
Difference in Profile of Mood States (POMS) subscale mean scores between private and public patients
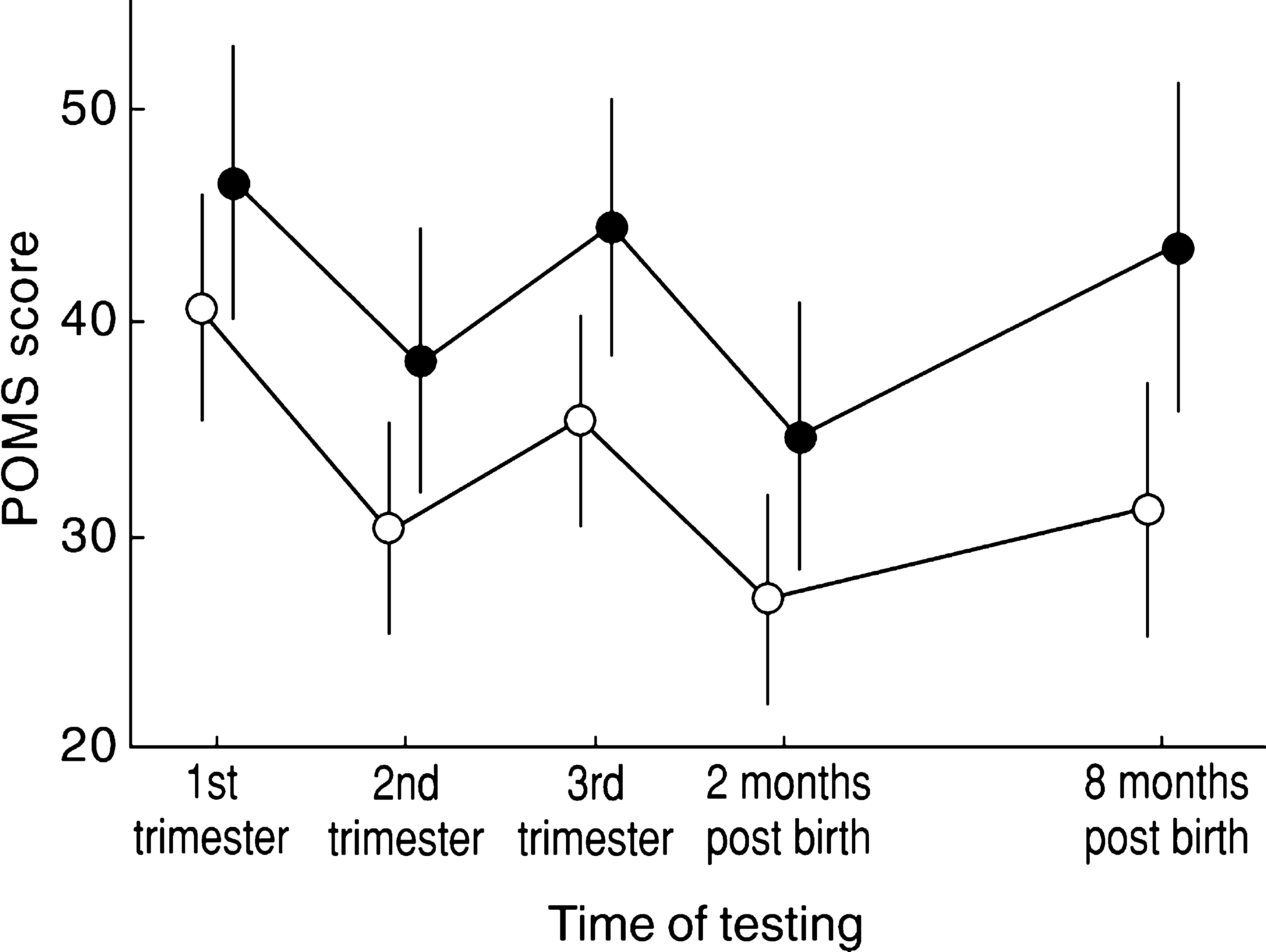
Ante and postpartum POMS scores. •, public patient; ○, private patient
Two months after birth the women experienced an improvement in mood relative to that experienced during pregnancy. In fact, mood at this time was better than on any other occasion for both private and public participants. However, mood had declined once again by 8 months after birth.
The POMS score of the public patients was consistently higher than that of the private patients during the postpartum period also. However, the difference reached statistical significance (p = 0.01) only 8 months after birth. The decline in mood between 2 and 8 months after birth was more pronounced for the public participants (Fig. 1). The scores on the subscales of anger-hostility, confusion-bewilderment, depression-dejection, tension-anxiety and vigour-activity were higher among the public participants at 8 months after birth (Table 2).
Overall mood of public and private patients
Repeated measures ANOVA was undertaken to assess the difference between public and private patients' mood over time. Women missing only one POMS score (n = 24) were included in the analysis and the missing value was imputed on the basis of the public and private group means. Women with more than one missing POMS score were excluded from the analysis. This resulted in a sample of 299 women.
The following covariates were selected to be included in the model on the basis of their significant relationship with the outcome variable; Intimate Bonds scores (care and control); Locus of Control scores (internal and external); Defense Style scores (mature and immature); mother's age, education (tertiary-educated vs nontertiary-educated) and employment (full-time vs not full-time) status; and father's employment status.
The null hypothesis that there was no difference between the mood of public and private patients during pregnancy and after childbirth was rejected (F = 4.45, p = 0.036). Covariates positively associated with mood during pregnancy and following childbirth were perception of partner's care (F = 8.89, p = 0.003) and mature defence style (F = 17.40, p < 0.001). Immature defence style was negatively associated with mood (F = 17.91, p < 0.001). External locus of control was also influential in the model, although not significant (F = 3.57, p = 0.06).
Predictors of mood during pregnancy and following childbirth
The effect of hospital insurance status on mood during pregnancy and birth (as indicated by the mean POMS score for each woman) was modelled using stepwise linear regression, controlling for variables that also potentially influence mood. Predictor variables included in the model were health insurance status (public vs private); mother's age, education and employment status; father's employment status; and Intimate Bonds, Locus of Control and Defense Style scores.
The variables that significantly predicted mood during pregnancy and following birth (i.e. those remaining in the model) were private health insurance (β = −8.01 [95%CI = −13.36 to −2.66], p = 0.0036); perception of partner's caring behaviour (β = −0.63 [95%CI = −0.99–0.27], p = 0.0007); external locus of control (β = 0.24 [95%CI = 0.03–0.45], p = 0.0237); mature defence style (β = −5.72 [95%CI = −8.41 to −3.03], p < 0.0000) and immature defence style (β = 9.29 [95%CI = 5.77–12.81], p < 0.0000). These factors together accounted for 29% of the variance in mood.
Women with private health insurance, on average, scored eight points better than those without private health insurance. The interquartile range for the average POMS score was 35.6 points. Thus, the difference between the mood score of public and private patients was equivalent to almost one-quarter of the interquartile range.
Private health insurance was not confounded by any of the other significant variables, that is, the coefficient for private health insurance was largely unchanged as the other variables were added to the model.
Discussion
In this study the ante- and postpartum mood of women who were private patients was significantly more positive than that of women who were public patients. These findings can be interpreted in several ways. It is possible that the different models of obstetric care provided by the public and private health systems influence the mood of the women who use them. Alternately, there may be personal and social factors that the women bring with them to the life-changing event of pregnancy and birth that contribute to their mood.
There are differences between the care provided for public and private obstetric patients in Australia, including the fact that private patients have a longer hospital stay [36]. Additionally, they generally have more continuity of care and have chosen their birth attendant, and may therefore feel more in control of their lives.
Given the relationship between income and private health insurance, the better overall mood of the private patients could be related to their materially advantaged circumstances. It may be that pregnancy and birth are more welcome and less stressful events for women who are economically secure. Certainly, other studies have reported a relationship between income or standard of living and depression [23–27].
External locus of control and immature and mature defence styles proved to be important personality factors influencing mood during pregnancy and following birth. A previous study has identified an association between a high score on antepartum assessment of external locus of control and postpartum depression [8] while another found no such relationship [37]. Immature and mature defence styles were the strongest predictors of overall mood. Further research to evaluate the usefulness of the Defense Style Questionnaire as a screening tool to identify women at heightened risk of mood disturbance during pregnancy and following birth is indicated.
The findings of many other studies have also highlighted the critical role played by partners in the psychological wellbeing of women during pregnancy and following birth. Women who perceive their partners to be uncaring are more likely to be assessed as having disturbed mood including depression and have a poorer outcome following a depressive illness [4,5,9–11,38].
The changing pattern of mood during pregnancy and after birth described in this study is similar to that observed previously. In particular, an improvement in mood during the middle trimester of pregnancy has been noted [18]. The other consistent finding is a peak in mood disturbance immediately prior to delivery, which tends to improve considerably in the weeks following birth [1,39,40]. Understanding the changing pattern of mood during pregnancy and following birth can inform both clinical practice and women themselves.
The main strength of this study is the longitudinal study design, which facilitated the follow up of a large group of women across their pregnancy and for a substantial period following birth. The high retention rate (92%) is also noteworthy. However, certain limitations must be acknowledged when interpreting the findings. The study participants were volunteers and not a representative sample of Australian women. The extent to which this biases the results is difficult to estimate. The outcome measure was based upon a self-administered questionnaire. Consequently, the validity of the findings depends on the sensitivity of the instruments, the accuracy of the participant's recall of events and their willingness to disclose personal information regarding emotional states. Finally, the POMS questionnaire is a screening tool, and while a high score indicates a disturbed mood, this is not the same as a clinical diagnosis of depression.
The impact of social and economic policies on the distribution of wealth cannot be ignored if we want to prevent both physical and psychological ill-health, including antepartum and postpartum depression. However, more short-term, pragmatic responses are also relevant. Planning for the nature and distribution of health and other services is one area in which knowledge about vulnerable groups can be meaningfully applied. Access to services should be based upon need, and not upon ability to pay. In the case of psychological wellbeing during pregnancy and following birth this is particularly important given that those with diminished ability to pay are the more vulnerable group. Public patients are more likely to experience mood disturbance during pregnancy and following birth compared with private patients, and are therefore in greater need of preventive and supportive social, psychological and psychiatric services.
Footnotes
Acknowledgements
Heather Rowe Murray (KCWH, The University of Melbourne), Jean Small (KCWH, The University of Melbourne) and Ewa Karafilowska (ITS, The University of Melbourne). This research was funded by the National Health and Medical Research Council as a Postdoctoral Public Health Fellowship awarded to Jane Fisher.