
Abstract
The involvement of consumers in the development, provision and evaluation of mental health services has attracted increasing attention in this country since the articulation of the National Mental Health Policy in 1992 [1]. Several models for consumer participation had been described, primarily from the United States, including consumer-operated, self-help services [2] and collaborative models involving shared decision making by consumers and providers.
The principle underpinning the involvement of consumers in the provision of services is empowerment. This has been described as a process through which clients obtain resources at multiple levels to enable them to gain greater control over their environment [3]. Concepts of self-efficacy, increased self-esteem and the sense that personal change can be achieved through one's own efforts are integral. Segal et al. [4], in their review of the components critical to empowerment, emphasise these concepts and the role of participation in the nexus of organisational and community activities as essential to the attainment of empowerment. While mental health services now concede the need to incorporate participation and empowerment into service delivery and depart from paternalistic models, there has been little consensus as how to best achieve equal status for consumers and how to work in a model of true partnership.
The Community and Consumer Service (CCS) Project received special project funding under the Innovative Grants Program of the National Mental Health Strategy to investigate the provision of client-focused services to community-based clients with schizophrenia and bipolar disorder. The Project aimed to empower the client by establishing parity between client and staff without legal imposition, and by involving clients in their rehabilitative process in a consensual manner that promoted their respect, dignity and self-determination.
The objectives of the study were as follows: (i) to provide client-focused services, thereby empowering clients to participate as more equal players in the management of their illness, and so increase compliance and service satisfaction; (ii) to reduce disability and increase client functioning by crisis stabilisation, active treatment interventions and support; (iii) to reduce rehospitalisation by stabilising client behaviour, thereby improving quality of life and reducing burden of care; and (iv) to deliver goal-orientated outcomes through development of structured client-focused recovery agreements.
The specific hypotheses to be tested in the Project were: (i) that the delivery of case management services in a more client-focused style than standard community practice would improve the outcome of clients with respect to functioning, disability, quality of life, service satisfaction and family burden of care; (ii) that the use of consumer advocacy services to enhance the client focus of service delivery would improve outcome; and (iii) that clients empowered by the use of more client-focused approaches to outcome would be more satisfied and compliant with received services.
Method
Selection criteria
The criteria for inclusion of clients in the study were: meeting DSM-PV criteria for schizophrenia, schizoaffective disorder, schizophreniform disorder or bipolar affective disorder; aged 18-65 years; English-speaking; referred for case management by community health services within the old Eastern Sydney Area Health Service; no co-diagnosis of substance dependence disorder; no extant Community Treatment Order (CTO) or Community Counselling Order (CCO); no significant history of violence unless associated with acute psychosis.
Procedures
Subjects meeting the referral criteria were invited to participate, and included inpatients due to be discharged from hospital and who had previously been case managed or new referrals; or community health centre clients who required re-referral for case management due to service delivery requirements. After giving written informed consent, participants were randomly assigned to one of three groups: (i) control group or standard case management group (i.e. case management as it is routinely practised by community mental health staff); (ii) client-focused case management (i.e. case management by CCS Project staff)—research group 1 (RG1); (iii) client-focused case management plus consumer advocate (case management by CCS Project staff plus assignment of a CCS Project community consumer advocate)—research group 2 (RG2).
Thus, we tested for advantages above and beyond standard case management, effected by a client-focused approach and, in turn, the addition of an advocate.
Treatment groups
Client-focused case management or RG1
Subjects allocated to this experimental group were case managed for a 12-month period by Project staff who were specifically orientated to a client-focused approach. Case managers participated in training workshops to enable the use of Rose's Advocacy Empowerment Model in clinical practice [5]. They also familiarised themselves with solution-focused [6] and narrative [7] approaches to therapy. During the study period, Project case managers strove to work in equal partnership with their clients. This process was enhanced by the use of customised recovery plans, adapted from Rose's [5] direction plan, with emphasis on the client's goals for recovery, not the service provider's. Where possible, recovery agreement meetings between the client, the case manager, the treating psychiatrist, a family member or significant other, and sometimes the consumer advocate were convened to reinforce support for the client in achieving their goals for recovery, thereby empowering the client and promoting self-advocacy. Although not based on the Strengths' Model [8], the Project case management style shared its focus on individual strengths and capabilities rather than illness and deficits.
Client-focused case management plus advocacy or RG2
Subjects allocated to this group also received the client-focused style of case management provided by Project staff described above, but were also assigned a consumer advocate. Six advocates and three reserve advocates were initially recruited to each work 3 h per week. Initially, this group comprised people who had experienced mental illness themselves (primary consumers) who were currently well, as well as siblings or carers of people who had experienced mental illness (secondary consumers) and some non-consumers who were interested in working with people with mental illness. Consumer advocates were trained at the commencement of the Project from both the perspective of the mental health professional as well as from the consumer's perspective. A number of consumer consultants were employed to train the Project advocates, during an intensive 3-day period on rights, the Mental Health Act, communication skills, listening skills and about the availability of resources. Mental health staff also provided information to the advocates on relevant issues associated with mental illness, treatment, and hospital and community management. The guiding principle for consumer advocates in their work was the promotion of self-advocacy for clients. Their role was to encourage client's self-confidence, provide role models for clients during their recovery, enhance their communication with case managers and participate in the development of recovery agreement meetings if the client wished. Consumer advocates were introduced to their clients by their case managers and assigned between three and six clients each, ideally for a 12-month period.
Standard community case management
Subjects in the standard group were case managed by existing community case managers using a diverse range of customary case management practices. Their practices were under frequent review by regular staff to incorporate changes in community mental health attitudes towards clients, consumer roles and therapeutic options. In general, however, there was less emphasis placed on client-focused approaches to improving compliance and client participation than in the research styles of case management. For example, there was no onus on case managers to develop recovery plans or arrange meetings with clients, families and service providers to empower the client. Clients in the control group remained with the same case manager if they were already receiving case management on study entry.
Baseline assessment
On study entry, the research assistant and Project case managers collected demographic data and information concerning age of onset of illness, duration of illness, medication type and dose, response to treatment, side-effects of treatment, attitudes to treatment, compliance with treatment, and attendance and participation in community health programs. A survey of clients' needs and attitudes to available services was also conducted prior to commencement of case management.
Measures
Baseline measures of functioning, disability, quality of life, service satisfaction and family burden were completed by different staff and family members. The measures of functioning and disability were: the Life Skills Profile (LSP), a 39-item measure of function and disability completed by case managers and families [9]; the Health of the Nation Outcomes Scales (HoNOS), a 12-item measure of functioning assessing global morbidity and functioning, completed by nursing staff and/or case managers [10]; and the DSM-III-R Global Assessment and Functioning Scale (GAF), assessing global functioning, completed by psychiatrist/psychiatric registrar [11]. Quality of life was measured using a brief 25-item questionnaire modified from the Quality of Life Index for Mental Health [12] and was completed by the client. Burden of care was assessed using the 30-item, semi-structured Family Interview Schedule [13], and completed by a family member via a telephone interview with the research assistant. Service satisfaction was measured using a brief nine-item scale modified from the Client Service Satisfaction Questionnaire (CSQ) [14,15] and completed by the client with the research assistant.
Twelve-month follow-up
All measures were repeated on completion of the study after approximately 12 months. Information concerning compliance, response to treatment, case load numbers and satisfaction with case management was again recorded and data collected concerning the client's satisfaction with involvement in the CCS Project.
Information was also collected from Project and community staff case managers concerning their sense of satisfaction with the service they provided, their ratings of clients' response to treatment, compliance with treatment and the extent to which they believed they had been client-focused in their style of case management.
Data relating to the number and duration of hospital admissions (bed-days) and the use of crisis services were obtained from medical records for the 12 months of participation in the Project.
Statistical methods
For continuous variables, analysis of variance was used, with or without the repeated measures factor as appropriate, to analyse group differences. Cross-sectional comparisons were performed using the Chi-squared statistic for categorical data. The final stage of the data analysis involved predicting outcome using regression analyses.
Results
In total, 530 clients were considered for participation in the CCS Project. Of these, 359 clients did not fit the selection criteria, largely due to clients with dual diagnoses, older age, or a significant history of violence, together with a number who were admitted to our services from other areas. Table 1 summarises the reasons for clients failing to meet the selection criteria. Fifty-two clients refused participation. Of those, 17 were ‘happy to remain with their current case manager’; nine felt that there was ‘too much going on’ in their lives to consider participation; 17 were ‘disinterested’ in the Project; five were unwilling to answer any questions or discuss their mental health; and four subjects ‘didn't want case management at all’, despite being referred for it.
The 119 subjects who agreed to participate in the study were randomly allocated to one of three groups. A total of 35 subjects comprised the control or standard case management group, the client-focused case management group (RG1) had 39 subjects and the client-focused case management plus advocate group (RG2) had 45 subjects. Of the total, 43 were recruited from the Inner City sector and 76 were recruited from the Eastern sector. Sixty-nine subjects were recruited from psychiatric hospitals and 50 from the community health centre. All subjects had been referred for case management. Figure 1 shows the number participating in each group and the drop-out rates over the course of the Project. Although subjects were also followed up at 6 months, the results for this stage will not be presented here as they add little to the study results.
Baseline results
Total group subject characteristics-sociodemographics
The mean age of the 119 subjects was 36 years (SD = 9.8); 68 were male and 51 female. The mean number of years of education was 11.6. Subjects predominantly lived alone (39%) or with family (30%). Seventy-two percent were supported by the disability support pension or sickness allowance, and for a mean duration of 80 months. Seventy-nine (66%) subjects met DSM-IV criteria for schizophrenia; 19 (16%) for schizoaffective disorder, seven (6%) for schizophreniform disorder and 14 (12%) for bipolar disorder. The mean duration of illness was 117 months (SD = 98.9, range = 1–432) with a median duration of 90 months. The mean number of hospital admissions since illness onset was six (SD = 6.4, range = 1–30), with a median number of four admissions. The mean and median number of admissions in the year prior to entry into the study was one (SD = 0.93, range = 0–6).
Number of clients not suitable for inclusion in the study
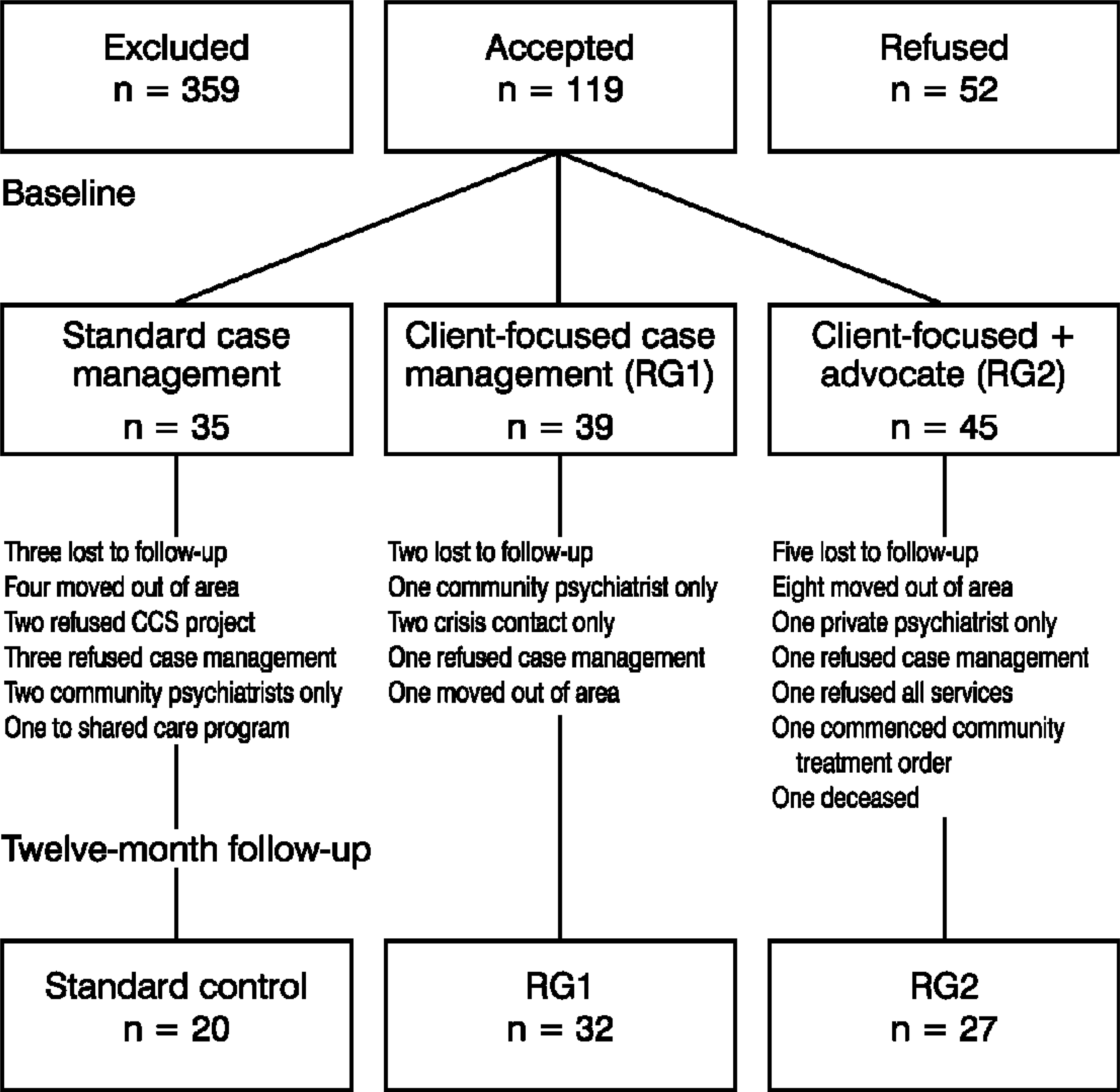
Flow chart of clients through the course of the Community and Customer Service Project
Comparison of the three study groups
Baseline subject characteristics and sociodemographic variables
Table 2 demonstrates that there were no significant differences between the three groups at baseline with respect to sociodemographic variables, illness factors or medication factors. Furthermore, there were no significant (between group) differences for diagnosis, medication compliance, compliance with treatment, response to treatment and the clients and service providers' perception of the clients' link to psychiatric services.
Table 3 shows that there were no significant differences between the three groups at baseline with respect to measures of functioning, disability, satisfaction with service, quality of life and family burden of care. The sample size varies for each test in accordance with difficulties in data collection.
Twelve-month follow-up
By 12 months, 34% of clients had dropped out, leaving 79 subjects remaining in the Project (see previous Fig. 1). Drop-outs (n = 40) were compared to non-drop-outs on sociodemographic and illness variables. The only significant difference between the groups was that there was a higher percentage of clients living alone who remained in the Project (χ2 = 17.78, p < 0.01).
With respect to the three study groups, there were no significant differences between the groups at 12 months concerning current neuroleptic dose, severity of side effects, compliance with medication and response to treatment. Furthermore, there were no significant differences between service compliance and the case manager's perception of the client's link to services.
Baseline subject characteristics, sociodemographic, and illness variables in the study groups
There were significant (between group) differences with case manager's satisfaction working with their clients, specifically between the control and RG2 groups (F2,74 = 3.4, p = 0.04), with the latter being more satisfied. Again, there was a highly significant difference between the size of the case managers' case loads, with the experimental groups having smaller loads (p < 0.01).
Repeated measures analysis of GAF scores (F1,44 = 20.02, p < 0.01), overall disability scores on the HoNOS (F1,51 = 4.98, p = 0.03), and quality-of-life scores (F1.66 = 5.29, p = 0.03) showed significant improvement in functioning from baseline to 12-month follow-up; however, there was no significant difference between the groups for any of these measures (F2.44 = 0.20, p = 0.82). Life Skills Profile total scores did not change across 12 months, nor were there significant changes on the satisfaction with service questionnaire.
Mean total scores for measures of functioning, disability, quality of life and service satisfaction at baseline
Family Burden of Care scores showed significant differences both over time and between groups. Repeated measures analysis of total burden scores over 12 months were significant (F1,25 = 24.9, p < 0.01) as were total severity of burden scores (F1,25 = 11.64, p < 0.01), both in the direction of decreased burden. Only total severity of burden scores showed significant differences between groups at 12 months with families of the client-focused case management groups reporting less severe burden than the standard case management group (F2,25 = 4.36, p = 0.02).
There was no significant difference between groups in the number of days spent in hospital (F2,76 = 1.23, p = 0.30) or whether they were readmitted (F2,76 = 1.26, p = 0.29) during their involvement in the Project.
Although there was a trend towards a greater number of client contacts with crisis services for the control group compared with the experimental groups, the difference between groups was not significant.
Client satisfaction with involvement in the Project
Of the 70 clients who completed the Project Satisfaction Questionnaire at 12 months, 96% (n = 67) said they were satisfied to be involved with the Project. Reasons given by subjects in the control group were mainly ‘wanting to have a say in the improvement of services’ and ‘didn't mind helping out’, whereas the main reason for satisfaction in the client-focused case management groups was ‘changing to a more supportive case manager’.
Seventy-five percent of the client-focused case management subjects reported feeling that participation in the Project had made their lives ‘better’ whereas all of the control subjects reported things being the ‘same’ in their lives at the end of the Project (X 2 = 27.9, p < 0.01).
For standard case management, ‘being asked my opinion’ was the most important aspect of their positive response (69%), whereas the combined client-focused case management groups predominantly reported ‘the style of case management’ (41%) and ‘seeing their case managers more regularly’ (22%) as being influential. Twenty-five percent of the standard case management group felt they had ‘more say’ in their treatment compared with 56% of the client-focused case management groups. The predominant way that all study group members felt they had more say was by ‘having their suggestions listened to’.
Case management
Approximately equal numbers of control and research group subjects had had more than one case manager over the 12 months of the study (32%). All subjects in the client-focused case management groups reported that their case managers were satisfactory, compared to 81% of the standard case management subjects (p < 0.01).
There were significant differences between case manager characteristics in the client-focused case management groups compared with the control group. In particular, client-focused case management clients more frequently reported that their case managers seemed ‘to understand my problems’ (p = 0.04), ‘listen to me’ (p = 0.03), ‘help me reach my goals’ (p = 0.07) as well as ‘be available when I needed them’ (p = 0.01) than standard community case managers.
Consumer advocacy
A total of 27 subjects assigned to the advocacy group completed the study. Of these, only 17 subjects made sufficient contact with their advocate to give opinions on its usefulness. There were 10 clients who either refused to see a consumer advocate or were unable to be contacted by the advocate. The most frequently reported comment for those who did have contact with an advocate was that it was ‘supportive’ and they could ‘share experiences’ (65%). Most (88%) found having an advocate helpful. Subjects less commonly found that having an advocate ‘helped me to reach my goals’ (35%) but more often they felt ‘listened to’ (94%) and that their ‘ideas and opinions were valued’ (88%).
Discussion
This study set out to determine whether the provision of client-focused services to community-based clients with schizophrenia and bipolar disorder could improve outcome in terms of functioning, disability, quality of life, service satisfaction and family burden of care. It also aimed to determine whether clients were more satisfied with the provision of more client-focused services than with standard forms of case management. Client-focused services were defined by the provision of a style of case management which encouraged clients to work in equal partnership with their case managers and, as an additional experimental factor, by the inclusion of consumer advocates in the delivery of these services.
Improvements in outcome were found over time, but were not group specific. Most clients showed improvements in functioning, disability and quality of life over 12 months. This finding is in conflict with the recent review by Marshall et al. [16], who held that there was little evidence of improvement in mental state, social functioning or quality of life in case management clients with serious mental illness (compared to those receiving standard care). Improvement here could, of course, reflect the benefits of support service or ongoing improvement following earlier hospitalisations and illness exacerbation.
With respect to satisfaction with the style of case management and the provision of consumer advocacy, qualitative measures demonstrated that clients in the research groups more frequently reported that they were ‘being listened to’, ‘valued’ and ‘understood’ by Project case managers and that their case managers were ‘more available’ when they needed them, giving partial support to the original hypotheses; however, satisfaction with case management style and involvement with consumer advocates, did not impact on compliance-related variables.
While the hypotheses with regard to the effect of more client-focused services on outcome were not proven, several factors need to be taken into consideration with respect to interpreting the findings. The usefulness of the Project in terms of highlighting issues associated with community-based service delivery research, case management practices and the development of consumer advocacy services warrants careful analysis.
Limitations of the study
Sample size
A major limitation of the study was the sample size. With at least 600 clients with a diagnosis of schizophrenia in our area, we aimed to have 50 subjects in each of our groups, but had not anticipated the numbers of clients who would fail to meet the inclusion criteria. Severity of illness was not the major factor limiting recruitment, as scores on the measures of functioning (GAP, HoNOS and LSP) indicate, rather it was the numbers of clients who were transient and out of area together with those with significant substance abuse who mostly diminished the study sample size. Comprehending the complexities of the study and the need for randomisation in this population of clients with serious mental illness also hindered recruitment.
The high attrition rate throughout the course of the study may have affected the outcome measures by making it less likely that the sample was representative of the population of clients we set out to study [17]. These problems hamper most treatment studies in any population of clients with serious mental illness and emphasise the need for very large sample populations. Accommodating selection criteria as wide as possible would seem critical to obtaining adequate sample sizes sufficient to conduct meaningful community-based treatment trials.
Time frame
Clients were offered these client-focused approaches to treatment over a period of 1 year. This time frame was dictated by the period of funding (2 years) and the need to follow up each client after 12 months. However, to effect enduring changes, treatment periods may need to be longer. Subjective client reports from the study support the fact that they liked the approach to treatment; however, concepts of empowerment, partnership with health professionals and consumer participation in the delivery of services were new to their understanding. Project case managers frequently emphasised how much of their time was spent validating and supporting clients' capacity to make their own choices about treatment, indicating the likelihood that they had insufficient time to fully utilise this form of case management or to derive maximum benefit from it. Previous exposure to traditional case management was not accounted for and may have made adjustment to a client-focused approach more difficult.
Were there valid differences between the treatment approaches?
The concepts of advocacy and empowerment underpinning the client-focused approach to case management used in the study are not new to community psychiatry. The need for these treatment approaches has been increasingly espoused [18–20] and since the handing down of the Burdekin Report [21] in this country, mental health services and individual clinicians have undergone numerous atti-tudinal changes. These factors may have already affected the delivery of services to clients to such an extent that attempting to evaluate the impact of styles of case management based specifically on concepts of advocacy and empowerment was not possible because standard practice had already accommodated these principles and were too similar to be able to determine any differences.
Findings from the current study which support the likelihood that the style of case management was distinctive come from the qualitative data concerning clients' satisfaction with the service delivered by the Project staff. Clients in the client-focused research groups were more likely to perceive their case managers as more helpful, supportive, respectful and as assisting them in achieving their goals, supporting some differences in their approach. However, the most significant aspect of their perception of satisfaction was that they found their case managers to ‘be available’ when they needed them. While this is a key component of a client-focused approach, it is possible that these perceptions were based partly on the fact that Project case managers had more time available for clients, as they had fewer clients assigned to them, compared with standard case managers. This was not intended at the outset of the Project but developed as an artefact of the difficulties associated with recruitment. If it was the case that the case manager-client ratio was the key factor in both the clients' perception of receiving client-focused case management and a main reason why case managers perceived they could deliver this service, it underscores the importance of limiting the number of clients assigned to case managers so they are able to carry out their duties effectively and give satisfaction to both clients and case managers alike.
The contribution of consumer advocates
Unlike Felton etaI. [22], we were unable to demonstrate a beneficial effect on the outcome of clients who were assisted by consumer advocates. Consumer advocacy was a relatively new concept within Eastern Area Mental Health at the commencement of this Project. Indeed, a major component of the innovative nature of our grant application was the participation of consumers in the delivery of services. In our area, Consumer Consultative Committees were already in evidence in that consumers contributed to policy and planning on advisory boards, but the CCS Project was the first attempt at bringing consumers into mental health services as peer support persons. While their primary brief was to promote self-advocacy in clients so that they could work in equal partnership with service providers and redress the perceived hierarchical imbalance which has so often been a source of dissatisfaction to consumers, they had few real examples of how to do this. A major limitation then of the study was that consumer advocacy was not already established as a service to consumers at the time the research project commenced. This meant that consumers had to be recruited, trained, have their job descriptions defined, introduce themselves to service providers, promote their usefulness, deal with client confusion about their role, trial working in community settings, develop adequate opportunities for debriefing, determine ongoing training needs, and develop group cohesiveness during the lifespan of the Project and be evaluated for the impact of their services on client outcome at the same time.
Taken together, these factors hindered the full potential of the consumer advocates and limited the capacity of the Project to evaluate their impact. The Project did, however, provide an excellent learning opportunity and during its course, the advocates overcame the numerous setbacks and developed into a strong cohesive group with solid views on how consumer advocacy should be carried forward. These issues are more fully developed in a separate paper [23]. However, from the research perspective, these factors negatively impacted on the numbers of clients assigned an advocate and on the depth of their experience of advocacy. As only 17 clients had a relatively meaningful experience of advocacy, the sample size was too small to reach any definite conclusions about their effect on outcome. As clients' reports of their subjective experience of advocacy were positive, our findings support evaluation of an active advocacy program.
Footnotes
Acknowledgements
This Project would not have been possible without the support and assistance of the staff of the Prince of Wales, Prince Henry and St Vincent's Hospital Psychiatry Units and the Bondi Junction and Darlinghurst Community Health Centres. Particular thanks are due to Nancy Kohn, Madeleine Bridgett and Evan Kourkoulis for their involvement in the first half of the study. Special thanks are also due to the advocates who participated in the Project and to the Steering Committee for their guidance in developing the Project. The support of Susan Johnston and Renay Atkinson was also most appreciated.
We thank the Commonwealth Innovative Grants Program of the National Mental Health Strategy (Grant No. 22004) for funding this study.