
Abstract
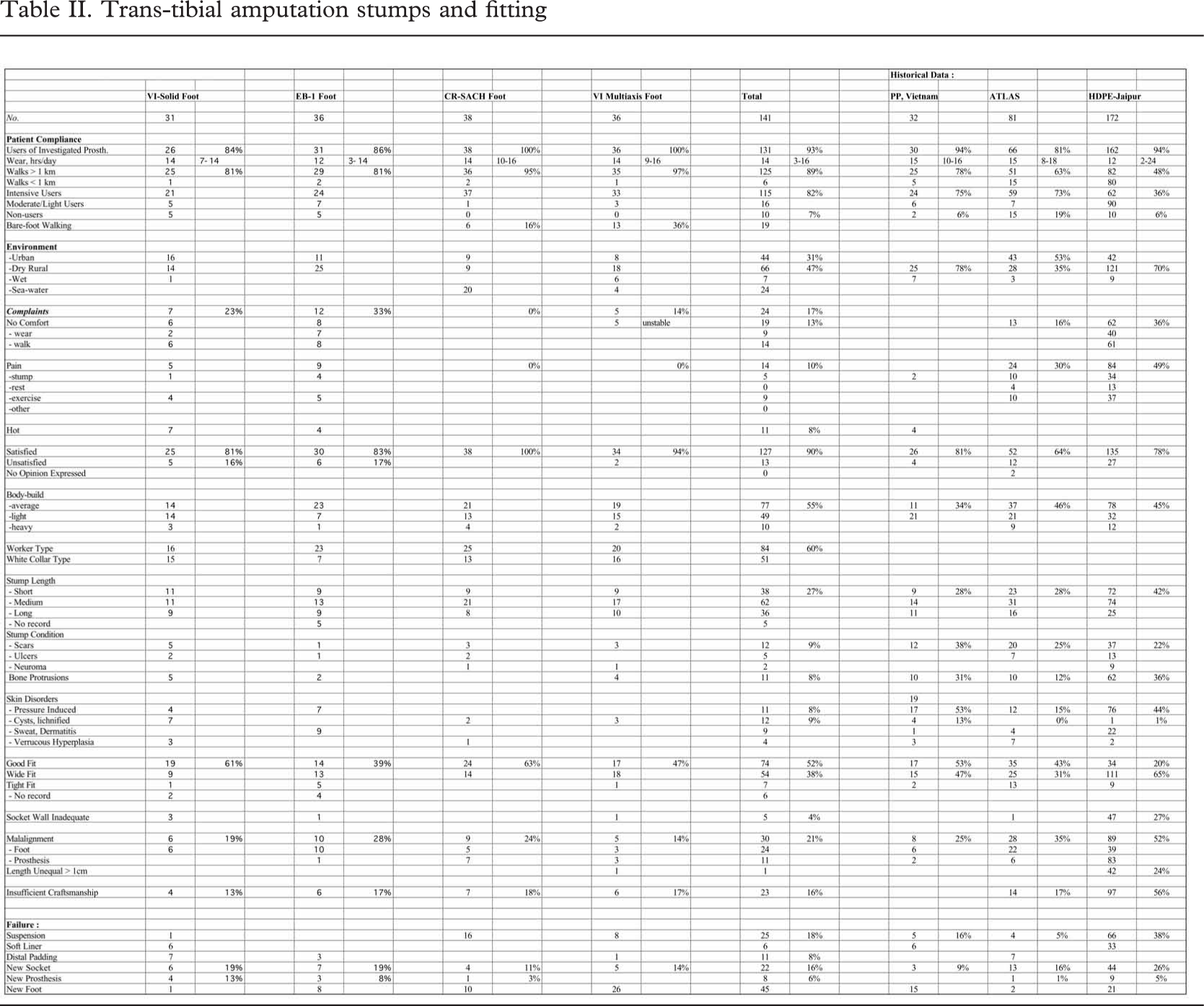
Based on four series of patients (N = 141) participating in clinical field testing of prosthetic feet and all provided with trans-tibial prostheses in accordance with the polypropylene component and assembly system developed by the International Committee of the Red Cross (ICRC) a series of quality benchmarks was developed and tested against historical data. The patient compliance demands were set for walking > 1km at 90 ± 10%, non-users at 5 ± 5%, discomfort at 10 ± 10%, pain at 10 ± 10%, and patient satisfaction at 90 ± 10%. The technical performance demands were set for good socket fit at 60 ± 10%, misalignment at 15 ± 10%, insufficient craftsmanship at 10 ± 10%, and requirements for socket change at 10 ± 10%.
Introduction
Little attention has been given to developing quality standards for craftsmanship, durability and patient compliance in respect of trans-tibial prosthetics.
At the 1995 ISPO consensus conference on appropriate prosthetic technology in developing countries (Day, 1996) several authors confirmed that the vast majority of service units utilised the plaster wrapping cast and used a modified plaster model to fabricate a plastic PTB socket. Polypropylene is the most commonly used material for socket fabrication. However, this requires the skill of a trained prosthetist or a trained orthopaedic technologist. The question raised was, if it is possible to define a gold standard for trans-tibial prosthetics in low-income countries?
Patients and methods
In order to achieve consistency of prosthetics provision and of clinical follow-up two series were selected prospectively from each of the two Category-II schools in Cambodia (CSPO) and Vietnam (VIETCOT), who were running clinical field testing programmes for ISPO with the polypropylene prosthetics system (Verhoeff et al., 1999) brought to the market place by the ICRC. The prostheses were supplied by the teachers and their students and a systematic follow-up programme implemented, which allowed for comparison with other follow-up studies conducted by ISPO. The feet utilised in Cambodia were the polyurethane rubber coated SACH foot from CR Equipment SA, Switzerland), which is distributed through ICRC to their projects; and a vulcanised, multi-axis foot from VVAF (Vietnam Veterans America Foundation), Kien Khleang, Cambodia. In Vietnam the feet were both SACH designs with internal keel and vulcanised rubber skin from VVAF, Kien Khleang, Cambodia, or Prosthetic Outreach Foundation (POF), Ba Vi Factory, Vietnam.
The follow-up was planned after approximately 9 months and 18 months, respectively, but the study was completed, if the foot had broken down and required replacement. The follow-up focused on patient compliance based on direct interviews; the basis for prosthetic supply, i.e. stump descriptors and amputee characteristics as based on the examination by the follow-up team; the craftsmanship, i.e. fit, alignment (< 20° deviation), socket wall adequacy (< 2 cm short), length (< 2cm difference), as assessed by the follow-up team; and eventually recording of failures. All interviews were conducted by an orthopaedic surgeon (JSJ, Denmark), who also assessed the stump and prostheses together with a Category-I prosthetist-orthotist (RN, Norway; JZ, USA).
For statistics Students-t-test (unpaired, two-tailed, two-sample, unequal variance) was applied.
Demographics
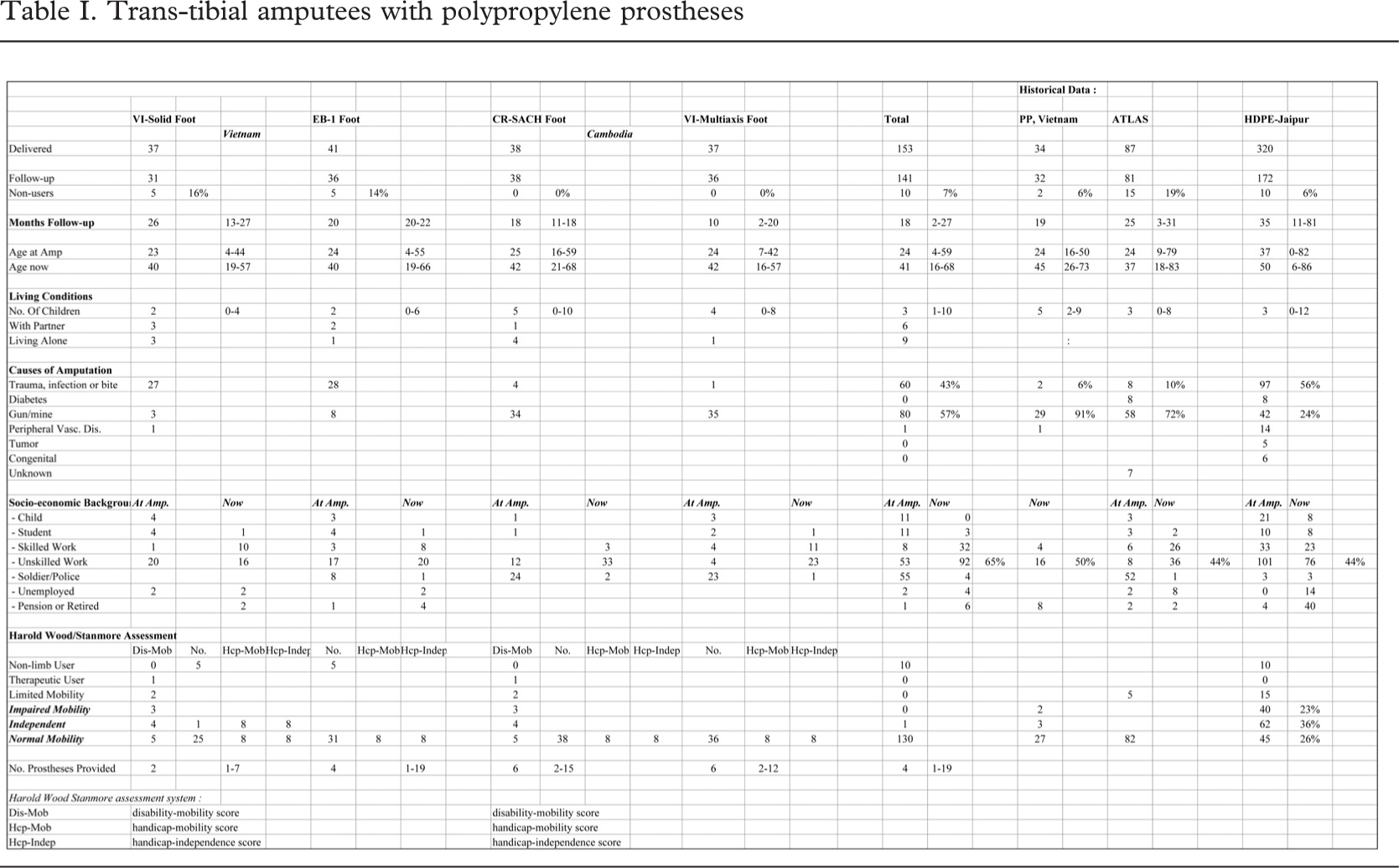
Altogether 153 trans-tibial polypropylene prostheses were delivered; 141 being followed for a median of 18(2–27) months; being shortest for the multi-axis foot because of high early failure rate, and longest for the other foot from VVAF because of delayed delivery of the matching foot series in Vietnam.
The amputees were 24(4–59) years of age at the time of amputation, and 41(1–68) years at the time of the latest follow-up (Table I). Some 6% (9/141) lived alone, 6 (4%) with partner; the remainder had a family with a median of 3(1–10) children.
The cause of amputation was peripheral vascular disease in one and trauma in 140; 57% as a result of landmines or other war ordnance. As seen from the table 64% (47/74) of the Cambodian amputees were soldiers or police at the time of amputation. At the time of follow-up 65% (92/141) were occupied with unskilled work, mostly farming, and for nearly half of the Cambodians salt-water fishing. Over the years a median of 4(–19) prostheses had been provided.
At the follow-up 10 were non-users of the provided prosthesis, whereas the remainder experienced unlimited use and no restrictions in coping with the surroundings; all being community ambulators (Davies and Datta, 2003).
Three other series (Jensen and Heim, 2000; Jensen and Raab, 2002; Jensen et al., 2004) were identified in which the same assessment system had been applied (Table I). The series from Vietnam provided with polypropylene prostheses according to ICRC were 45(26–73) years of age at the time of follow-up, 97% (31/32) of amputations resulting from war ordnance or trauma, and 63% (20/32) were in work at the time of follow-up. The ATLAS series was from El Salvador and Cambodia, being 37(18–83) years at follow-up, 82% (66/81) resulting from war ordnance or trauma, and 78% (63/81) in work at the time of follow-up. Finally the HDPE-Jaipur limb series was from Honduras, Uganda and India. The age at follow-up was 50(6–86) years, 81% (139/172) of amputations were traumatic, and 80% (137/172) in work at the time of follow-up.
Trans-tibial amputees with polypropylene prostheses
Patient compliance
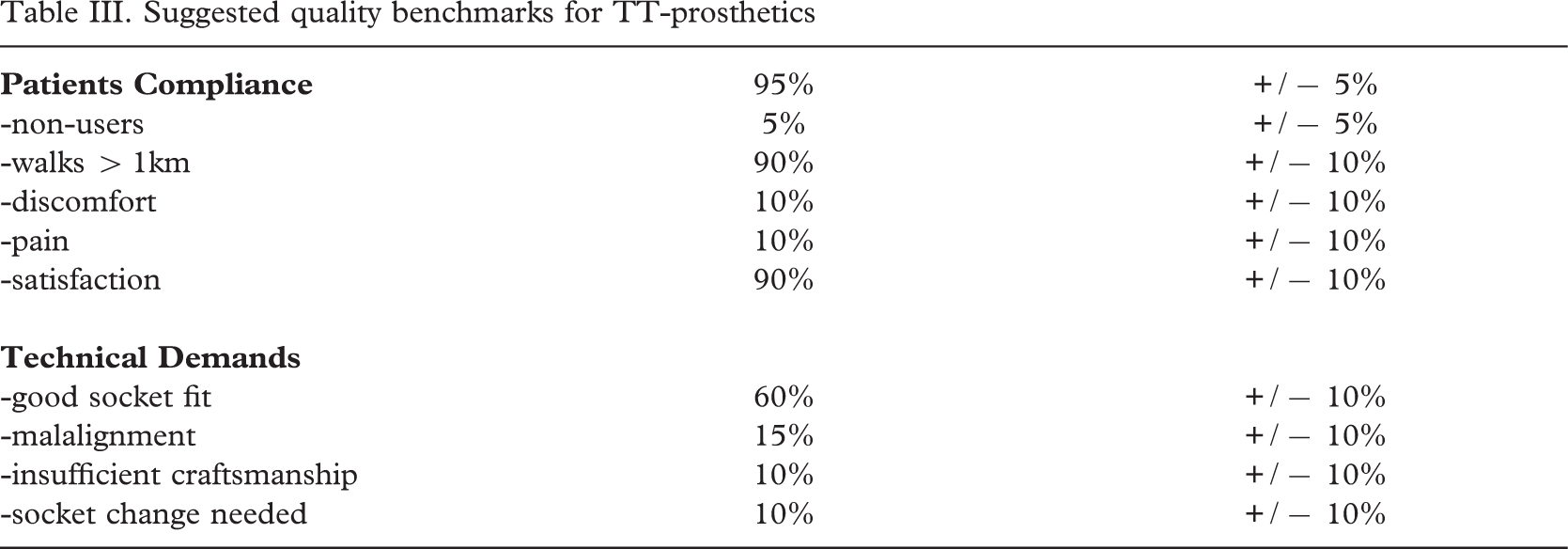
The patient compliance (Table II) was high; 93% (131/141) being users of the investigated prosthesis with a median wearing period of 14(3–16) hrs/day. Intensive use was recorded for 82% (115/141), and 89% (125/141) could walk > 1km; the environment being dry rural or urban in 78% (110/141) of cases.
Complaints were noted in 17% (24/141), being discomfort in 13% (19/141), or pain in 10%(14/141) solely or in combination. Some 8% (11/141), all Vietnamese, felt the soft liner of the socket as being hot. Altogether 90% (127/141) were satisfied with the prosthesis, ranging from 81% (25/31) to 100% (38/38) in the different series.
Characteristics of amputees and stumps
Sixty per cent (60%, 84/141) were assessed as worker types, and the body-build being average in 55% (77/141). The stumps were found to be short in 27% (38/141). Only a limited number had scars (9%, 12/141) and bone protrusions (8%, 11/141). Pressure induced skin disorders, cysts and lichnified skin was encountered in 17% (23/141).
Craftsmanship
A good fit was obtained in 52% (74/141), however, ranging from 39% (14/36) to 63% (24/38). A wide fit was seen in every third patient (38%, 54/141). An inadequate socket wall height (>2cm) was recorded in 4% (5/141). Misalignment (>20°) was a feature in 21% (30/141), mostly related to the foot being in dorsiflexion. Inadequate craftsmanship, which was defined as two errors or more in respect of fit, socket wall, alignment and length (±2cm), was encountered in 16% (23/141). Failure of the socket and/or alignment, or failure of the foot fixture resulted in a new socket in 16% (22/141), or a new prosthesis in 6% (8/141).
Trans-tibial amputation stumps and fitting
Discussion
With regard to the demographics there is no major deviation between the subsets although recruited from two different, although neighbouring countries.
The crucial question raised is whether the four subsets are consistent enough to permit the development of quality benchmarks. The standard deviation on the mean of the four series in respect of walking > 1km, non-users, lack of comfort, patient satisfaction are all less than 10% points; for pain and good fit 11–12% points; and alignment, inadequate craftsmanship, and need of socket change 2–6% points. This could allow the definition of the benchmarks as the rounded off average percentage ±10% points.
In respect of the historical series there are some minor differences in relation to age for the HDPE-Jaipur series, and prevalence of unskilled work in both the ATLAS and HDPE-Jaipur series. More than 93% of amputees in the series under investigation were community ambulators (Davies and Datta, 2004); the same being the case with the polypropylene (Jensen and Heim, 2000) and ATLAS (Jensen and Raab, 2002) series. In the HDPE-Jaipur series (Jensen et al., 2004) 62% were community ambulators, but 85% household ambulators, giving a fair basis for comparison.
The primary goal of prosthetic provision is to make the amputee ambulatory, comfortable and satisfied with the device. If benchmarks were set for walking > 1 km at 90 ± 10%, non-users at 5 ± 5%, discomfort at 10 ± 10%, pain at 10 ± 10%, and patients satisfaction at 90 ± 10%, then the poly-propylene series from Vietnam (Jensen and Heim, 2000) would fulfil all the criteria, but ATLAS (Jensen and Raab, 2002) fall short on non-users, pain and satisfaction; and HDPE-Jaipur technology (Jensen et al., 2004) on walking capacity, discomfort, pain and patient satisfaction. This is consistent with the conclusions of those publications.
Suggested quality benchmarks for TT-prosthetics
At the 1995 consensus conference (ISPO, 1996) many authors asserted that end contact in sockets was contraindicated because the terminal soft tissue cover of many stumps was inadequate in amount and quality. In such circumstances the plastic sockets were claimed to be deliberately lengthened to avoid such contact, and many fitted as hard sockets (Day, 1996). The investigated series presented less stump problems than the historical series, which can contribute to better comfort and less pain.
In the area of technical performance the benchmarks could be set for good socket fit at 60 ± 10%, misalignment at 15 ± 10%, poor craftsmanship at 10 ± 10%, requirement for socket change at 10 ± 10%. It has been said before (Jensen, and Heim, 2000) that wide fitting sockets are common in many developing countries together with open-ended sockets. A wide fit can not prevent the stump from sliding down leading to pressure induced skin disorders and stump pain, as occurred in the ATLAS (Jensen and Raab, 2002) and HDPE-Jaipur (Jensen et al., 2004) series. In respect of alignment both the ATLAS (Jensen and Raab, 2002) and HDPE-Jaipur (Jensen et al., 2004) series failed and also in respect of overall craftsmanship. Eventually all series passed the benchmark for requirement of new sockets.
In conclusion, it is possible to develop quality benchmarks (Table III) from this study. There is certainly room for improvements before a gold standard can be defined and proved in practical use. It is felt that the results of this series should be found in the lower end of the acceptance level for quality. In the meantime there are no other definitions to measure against. It is important that the prosthetic service providers put the patient in focus and pay attention to these rather simple measures of quality, and that the education and training of the professionals take these into account. These measures should be built into their check-out and production record systems with the purpose of keeping track on the units’ standards for serving the amputees for the benefit of maximising patient compliance.
Acknowledgements
The study was sponsored by the Leahy War Victims Fund, United States Agency for International Development (grant no. HRN-G-00-00-00015-00). The opinions expressed in this paper are those of the authors and ISPO, and do not necessarily reflect the views of the USAID.