
Abstract
The silicon liner socket has been used in the trans-tibial prosthesis since the 1980s. Silicon liner sockets are sleeves of silicon material that are rolled onto the stump and fix the prosthesis to it. The producers of the liners propagate many advantages in their use i.e. better suspension of the prosthesis, protection of the stump skin and improved cosmetic appearance. This review was performed to find objective documentation in the literature in support of the advantages in prosthetic fitting and use of silicon liners. A medline search was performed with the key words: “silicon liner socket, Icelandic Roll On Silicon Socket (ICEROSS), trans-tibial prosthesis, lower leg prosthesis and stump sockets”. Six articles remained after application of the selection criteria. In two studies clinical examination was done while in the rest questionnaires were used to collect data. The indication for amputation varied from vascular insufficiency, diabetes mellitus and infection to trauma. Most studies mentioned improved prosthetic suspension compared to the conventional supracondylar fitting. Also the walking performance improved with less use of walking aids. There were reports of positive but also negative effects on the skin such as excessive perspiration and itching. Patients had a general preference in prosthetic appearance in favour of the prosthesis with a silicon liner. Further research is needed with the use of objective clinical parameters and a homogenous study group objectively to find advantages in the use of the silicon liner socket in the trans-tibial prosthesis.
Introduction
Silicon liners have increasingly been used in trans-tibial prostheses since their introduction by Kristinsson in 1986 (Kristinsson 1993). Many advantages have been propagated by the producers of the silicon liners in comparison with the “standard” prosthesis with a supracondylar fitting, i.e. kondyl Bettung Munster (KBM) and patellar tendon bearing (PTB), with or without suspension sleeve, and the conventional type prosthesis (Fillauer et al. 1989; Fitzlaff and Heim 2002; Kristinsson 1993). First of all the suspension of the silicon liner socket is claimed to be superior to the other socket types because of the close adhesion of the liner to the stump. The liner is also said to offer skin protection and diminish friction between the socket and the stump surface. Delicate skin would therefore be a good indication for liner use. The general comfort in wearing the prosthesis is also claimed to be improved. Lastly it is stated that the cosmesis is better and easily accepted by the amputee (Kapp 1999; Lake and Supan 1997). The material properties of the silicon liner, i.e. adherence to the skin, are reported to be partly responsible for these improvements in combination with the way the stump is fitted in the socket (Fillauer et al. 1989; Kristinsson 1993). The silicon material is pliable and sticky and closely follows the whole contour of the stump surface and a vacuum is created between the liner and skin. These properties also influence the soft tissue which is compacted, formed and controlled by the liner socket. The latter makes it possible to use the total surface bearing principle of the stump surface during loading of the prosthesis (Kristinsson 1993). These findings are however not substantially based on clinical research. In most instances the technical properties of the silicon liner socket are used to assume the benefits for the amputee.
Regardless of this a multitude of liners have been introduced in recent years, ranging from various silicon compositions to gel based, each with individual properties and theoretical advantages in use (Geertzen and Rietman 2002).
This review was performed to asses objective data in favour of the improvements in prosthetic fit and use in relation to the use of the silicon liner socket in the trans-tibial prosthesis.
Methods
Search
A literature search was performed in Medline, Embase and Amed to find relevant articles. Also the Cochrane and Cinahl databases were checked. The following key words were used: silicon liners, Icelandic Roll On Silicon Socket (ICEROSS), trans-tibial prosthesis, trans-tibial amputation, lower leg amputation and stump socket. Also the references of the studies found were checked.
Selection criteria
The following specific criteria were used systematically to describe the articles. Articles in English, Dutch and German were selected. Elements reviewed were the method of patient selection, study design (prospective, retrospective or case series), use of a valid research instrument and protocol with outcome measurements. Also the method of data presentation was noted (Table I). The authors preferred data given per individual patient i.e. the amount of centimetres of tibia displacement in the socket during swing or stance phase because this made data comparison between studies easier. There was a preference for prospective studies but well documented case series were accepted. Also studies with a study group larger than 10 patients were included and the use of a valid research instrument in combination with a well-documented protocol were preferred.
Inclusion criteria for studies.
Results
Search and description of the studies
A total of 132 studies were found in the literature search. After reading the abstracts, a total of 121 articles were excluded for not being relevant to the review: 38 articles studied the general biomechanics and socket techniques of the trans-tibial amputee/prosthesis, 25 discussed trans-femoral amputations, 14 discussed upper limb amputations, 8 studied silicon materials and properties, 3 discussed silicon finger prosthesis and 33 discussed silicon application in urology, implants etc. Eleven articles remained after this screening. After application of the selection criteria, five were excluded for the following reasons. Two studies did not use a well defined study population and three studies had an insufficient design. Six studies remained after the final selection and were analysed further.
Study population
A wide range of patient numbers was found to be included in the studies varying from 20 (Yigiter et al. 2002) to 83 (Hachisuka et al. 2001). In most studies the patients were selected from a larger group, however, the method of patient selection remained unclear. There were different indications for amputation including trauma, vascular insufficiency, diabetes, infection, tumor, congenital limb defects and spina bifida (Table II). The age of the included patients ranged from 15 (Yigiter et al. 2002) to 80 years (Datta et al. 1996). The age categories and age per patient was often not given in the individual studies. Also the duration of prosthetic use varied from 10 days (Yigiter et al. 2002) to 19 years (Dasgupta et al. 1997) and this was often not given for the individual patient but noted for a group.
Study population.
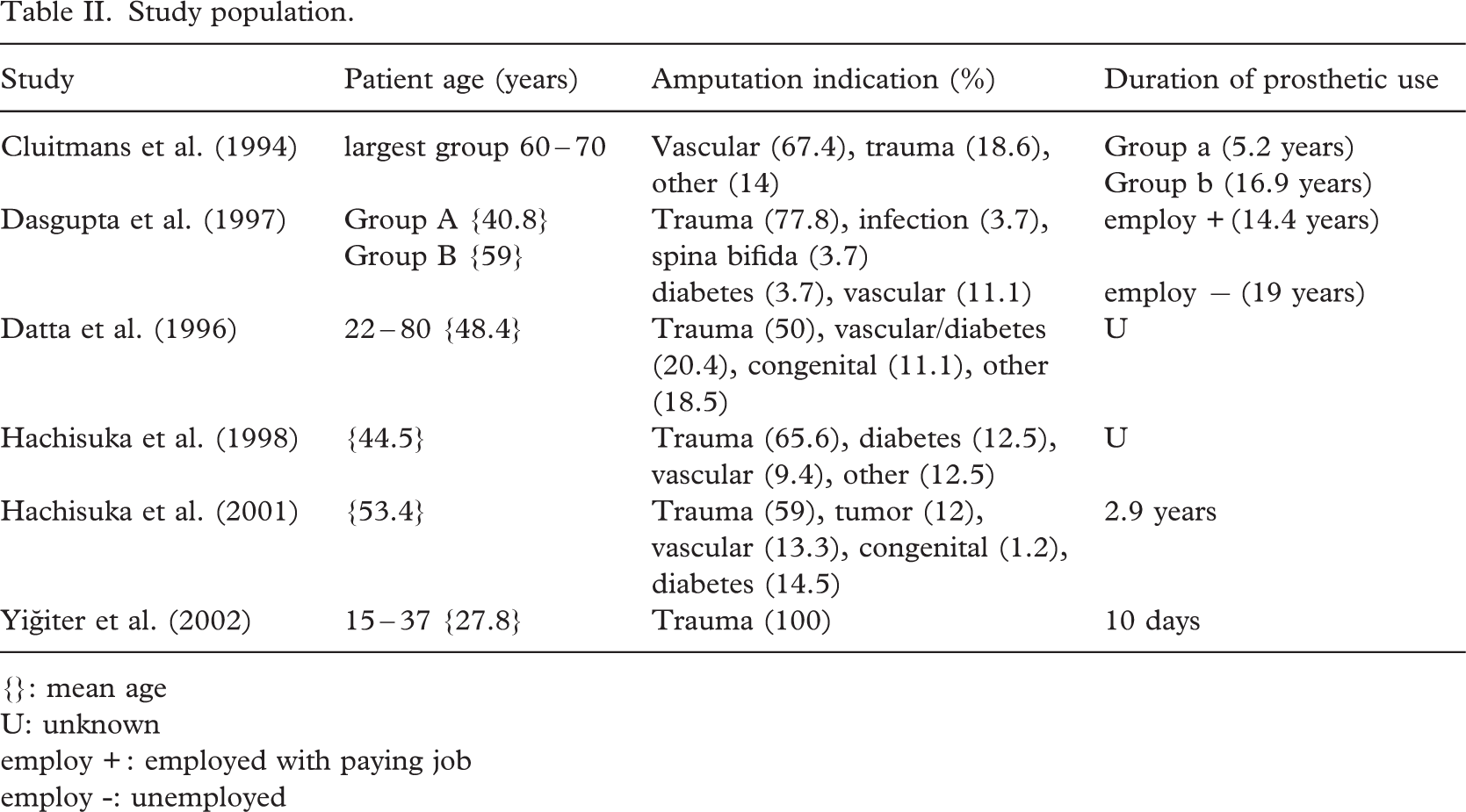
{}: mean age
U: unknown
employ +: employed with paying job
employ -: unemployed
Study design
In the study of Yigiter et al. (2002) a prospective design was used with inclusion of patients with a traumatic unilateral amputation. One-time examination was used to obtain the data. In two studies a retrospective design was used (Cluitmans et al. 1994; Dasgupta et al. 1997) while the rest were case series (Table III). In 5 of these studies (Cluitmans et al. 1994; Dasgupta et al. 1997; Datta et al. 1996; Hachisuka et al. 1998; Yigiter et al. 2002) the use of a silicon liner in the prosthesis was compared to the use of a patellar tendon bearing (PTB), Kondyl Bettung Munster (KBM) or other type of socket design (Figure 1).
Data presentation
In 4 studies (Cluitmans et al. 1994; Dasgupta et al. 1997; Datta et al. 1996; Hachisuka et al. 1998) the data were given per individual patient while in one study (Hachisuka et al. 2001) the data was presented as a percentage of the total. In the latter it was possible to calculate the patient data independently. One study (Yigiter et al. 2002) presented only group data (Table III).
Relevant outcome measurements
The authors were interested in the following outcome measurements: walking function, comfort, stump skin problems, pain in the stump or phantom pain, suspension, cosmesis and donning and doffing.
Qualities of the silicon liner
Different qualities of the prosthesis with a silicon liner socket have been examined in the studies. In Figures 1 and 2 these qualities are compared to those found in other types of prostheses.
Description of studies.
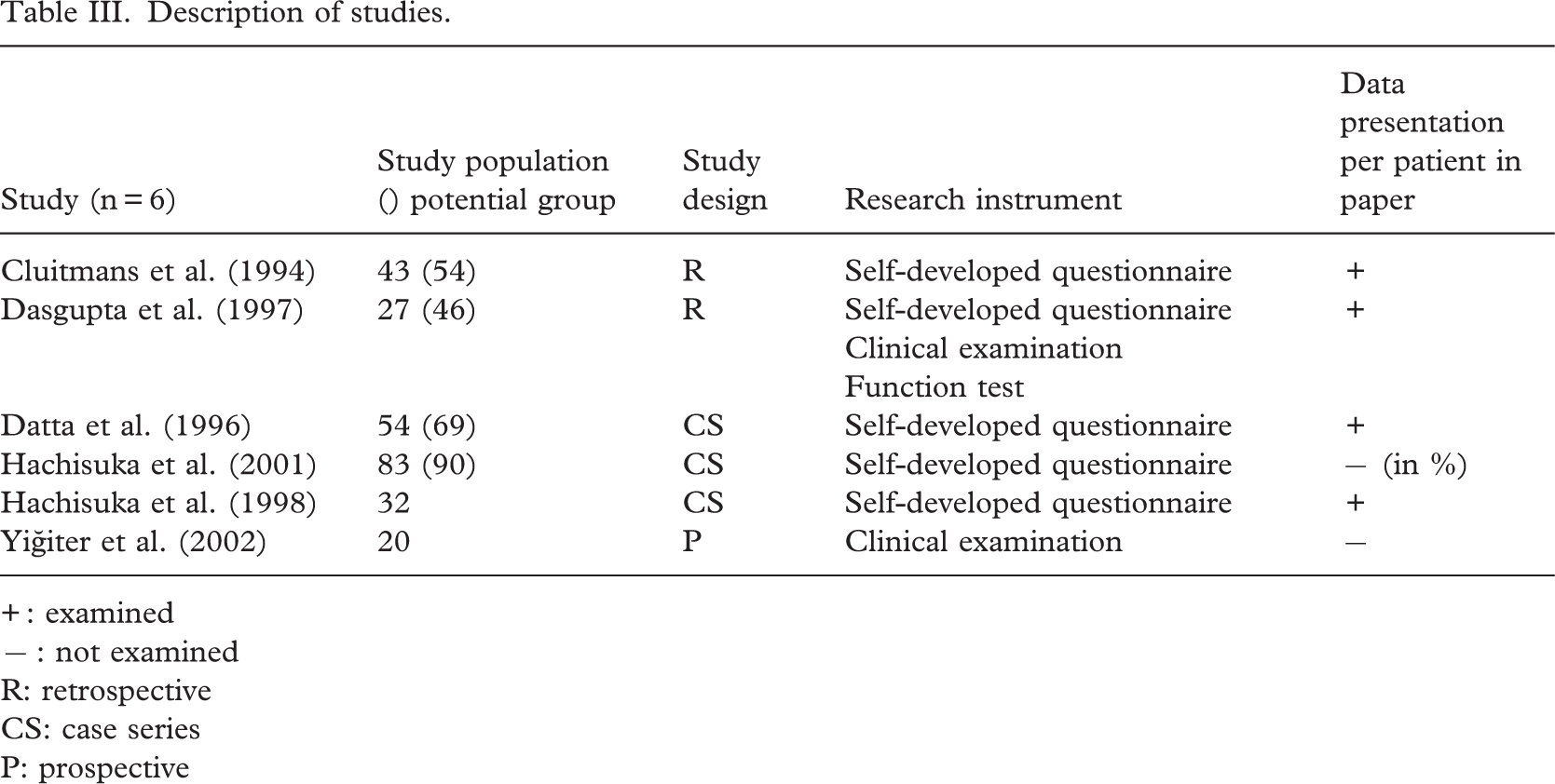
+: examined
-: not examined
R: retrospective
CS: case series
P: prospective
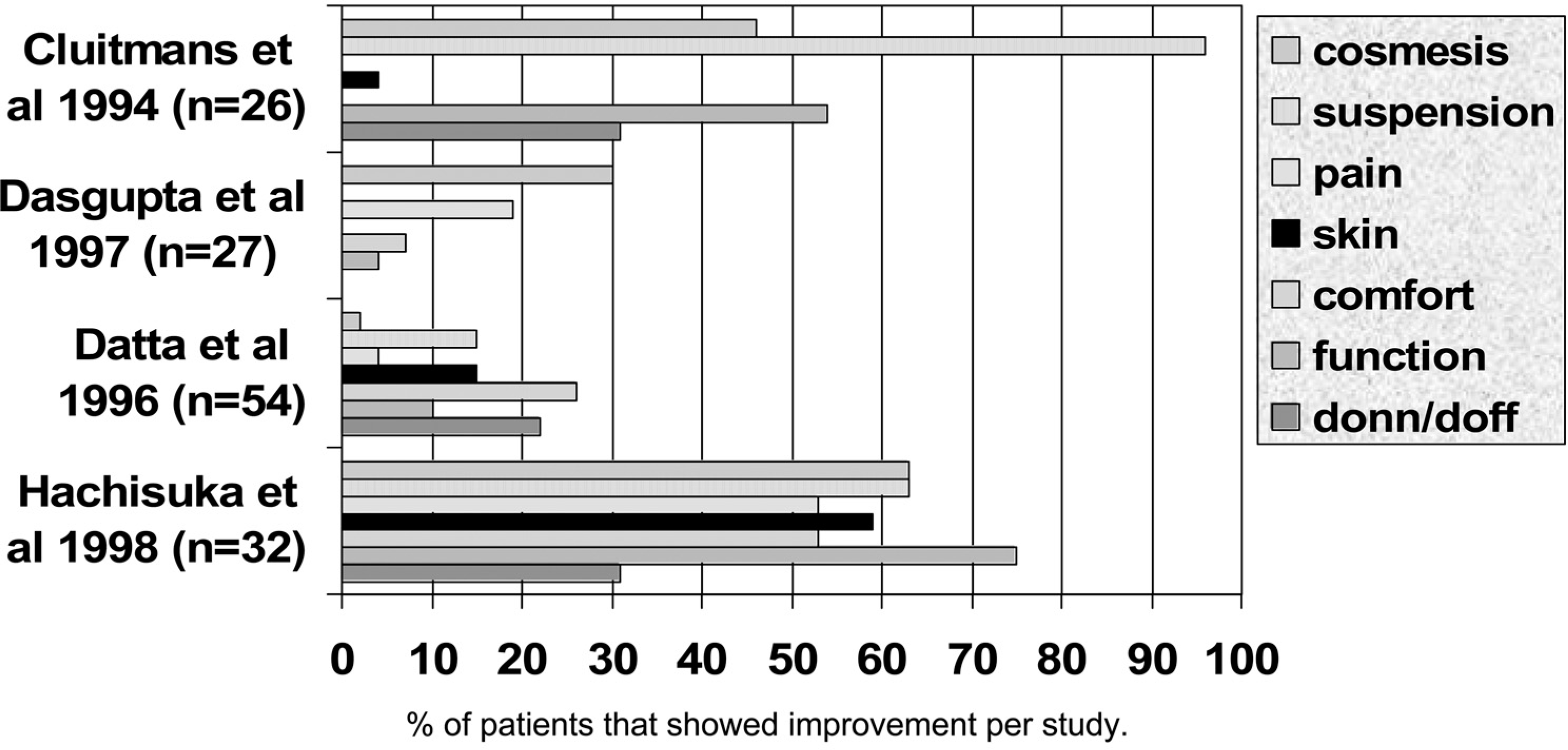
Silicon liner qualities: improvement compared to other socket type.
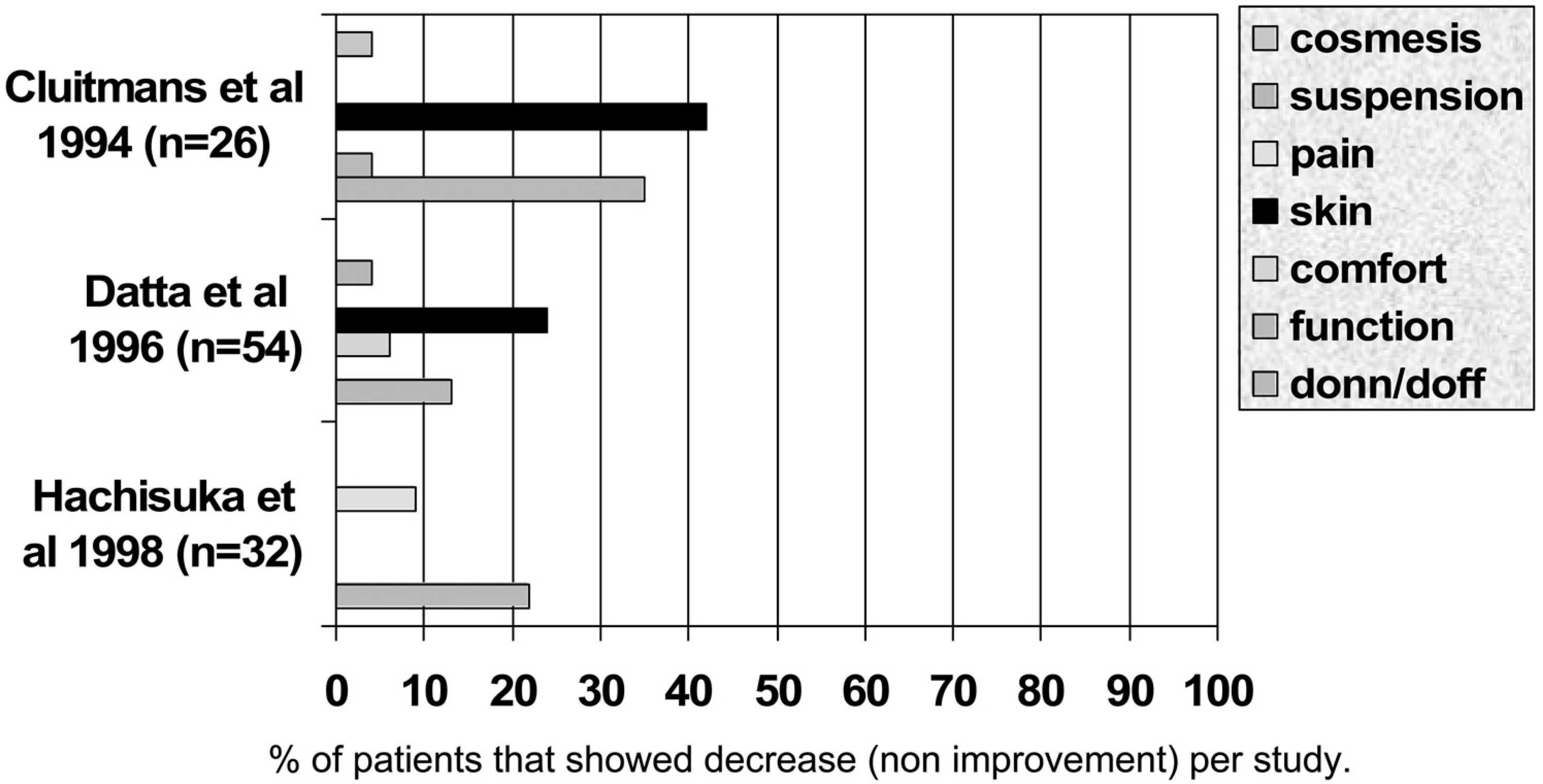
Silicon liner qualities: non improvers compared to other socket type.
Liner type
The ICEROSS silicon liner was used most often (Cluitmans et al. 1994; Dasgupta et al. 1997; Datta et al. 1996; Hachisuka et al. 2001). An exact specification of the type of ICEROSS liner was not given. In 2 studies (Hachisuka et al. 1998; Yigiter et al. 2002) the type of liner is not specified at all (Table IV).
Locking mechanism used
In 4 studies the shuttle lock mechanism was used (Cluitmans et al. 1994; Dasgupta et al. 1997; Datta et al. 1996; Hachisuka et al. 1998) to secure the silicon liner to the socket while in the remainder this was not specified (Table IV). In one study both the shuttle lock and cord lock was used (Cluitmans et al. 1994).
Socket characteristics.
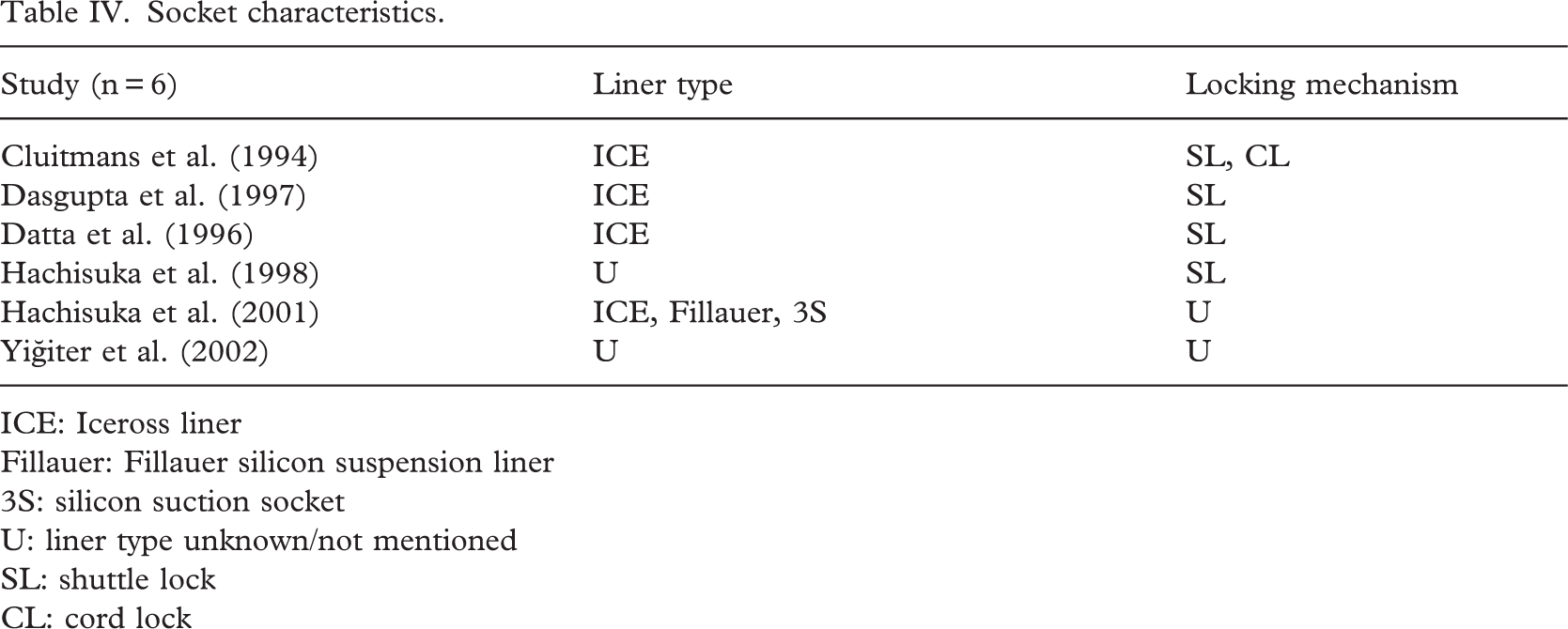
ICE: Iceross liner
Fillauer: Fillauer silicon suspension liner
3S: silicon suction socket
U: liner type unknown/not mentioned
SL: shuttle lock
CL: cord lock
Walking function
Walking function was improved in five studies, when compared to another type of prosthesis. Cluitmans et al. (1994) examined a total of 54 amputees. In a smaller group of 26 patients the use of the silicon liner socket was compared to KBM and other socket types. They examined changes in walking ability indoors and on uneven surfaces. They also examined changes in walking speed and distance with the most improvement in the latter (54%) compared to the KBM and other types of prostheses. Dasgupta et al. (1997) related the function to the number of meters that the patient could walk with the prosthesis. They found a slight increase in the distance and less use of walking aids in liner users. Datta et al. (1996) examined the change in prosthetic function by documenting the use of walking aids by the patient. They found a decrease in walking aid use indoors in combination with the use of a liner. Hachisuka et al. (1998) showed the most improvement in function related to general walking of the patient. Ambulation activities including walking and ascending and descending of stairs and inclines were studied by Yigiter et al. 2002. They compared the total surface bearing socket with the PTB and found a significant improvement(p5 0.05)in stair and incline ascending/descending. Also most temporal-distance characteristics like walking symmetry and velocity were improved. In general all studies showed improvement in walking function in liner users (Figure 1).
Comfort
In 3 studies (Dasgupta et al. 1997; Datta et al. 1996; Hachisuka et al. 1998) an increase in comfort was found ranging from 7–53% of the patients (Figure 1). Datta et al. (1996) also mentioned a decrease in comfort in a few patients that used the liner (Figure 2).
Skin
Skin changes are mentioned in 3 studies (Cluitmans et al. 1994; Datta et al. 1996; Hachisuka et al. 1998). Cluitmans et al. (1994) found an increase in skin problems from perspiration in 42% of the patients after liner use (Figure 2). Also creasing in the back of the knee presented a problem in 38%. In contrast local pressure points on the stump decreased after liner use. Datta et al. (1996) mentioned a decrease in skin abrasion and irritation in liner users (Figure 1). However, an increase in ulceration, itching, perspiration and blistering was found in other patients and this sometimes made it necessary to stop the use of the liner. Furthermore the liner caused irritation in the back of the knee in some cases. In contrast local pressure points on the stump decreased in these patients. Hachisuka et al. (1998) mentioned complaints of itching, perspiration and skin irritation in liner users but generally a decrease in skin problems.
Pain
In 3 studies (Dasgupta et al. 1997; Datta et al. 1996; Hachisuka et al. 1998) the sensation of pain was examined (Figure 1). Datta et al. (1996) mentioned a decrease of stump pain in some patients while a decrease in phantom pain in liner users was noted in 19% of the patients by Dasgupta et al. (1997). Hachisuka et al. (1998) also found a decrease in pain sensation in liner users (53%).
Suspension
In 4 studies (Cluitmans et al. 1994; Datta et al. 1996; Hachisuka et al. 1998; Yigiter et al. 2002) the suspension properties were viewed (Figure 1). Improved suspension was found by Cluitmans et al. (1994) in 96% of the patients that used the silicon liner sockets. Datta et al. (1996) found only a 15% improvement. Hachisuka et al. (1998) found a 63% improvement in suspension in liner users rated as a decrease in pistoning of the prosthesis. These suspension properties were however not studied clinically. The pistoning of the prosthesis was clinically studied by Yigiter et al. (2002). They marked the anterior superior border of the socket and measured the difference in the stance and swing phase of the prosthesis and found an average of 1.2cm. less pistoning in the liner socket compared to the PTB socket.
Cosmesis
In general, patients judged the appearance of the prosthesis with a silicon liner socket favourably (Figure 1). Hachisuka et al. (1998) mentioned the most improvement in cosmesis (63%) however a number of patients stated a decrease in cosmesis (Figure 2). Dasgupta et al. (1997) mentioned an improved cosmesis found by a number of patients. Datta et al. (1996) found no improvement and Cluitmans et al. (1994) noted an improved appearance of the prosthesis.
Donning and doffing
In 4 studies (Cluitmans et al. 1994; Datta et al. 1996; Hachisuka et al. 1998; Yigiter et al. 2002) donning and doffing of the prosthesis was judged (Figure 1). In general this regularly posed a problem in liner users. Cluitmans et al. (1994) and Hachisuka et al. (1998) mentioned a decrease in donning and doffing ease in respectively 35% and 22% of liner users (Figure 2). In both studies improvement was found in 31% of the patients when comparing liner use with another socket type (Figure 1). A significant (p50.05) improvement in donning and doffing was found by Yigiter et al. (2002) in favour of the liner users. Both an improvement and decrease were found by Datta et al. (1996).
Other qualities
A better stump hygiene in liner users was found by Cluitmans et al. (1994). Hachisuka et al. (2001) concluded that 66% of the patients washed the stump regularly while 53% washed the liner daily. Dasgupta et al. (1997) mentioned that patients who used a liner more often had a paying job possibly because of improved performance with the prosthesis.
Datta et al. (1996) found that patients felt they had better control over the prosthesis and mentioned that it felt like a part of the intact body.
Mechanism of action and indication for use
The positive effects of the use of a silicon liner socket can in theory be attributed to two mechanisms. The first relates to the way the stump is fitted in the socket and the second to the properties of the silicon liner material.
The fitting of the stump in the socket is done according to the hydrostatic volume principle said to result in an even pressure distribution over the stump in the socket known as “total surface bearing”. Skin and soft tissue is evenly loaded while standing and walking so that no peak pressure areas occur (Kristinsson 1993). In contrast the PTB principle uses the patellar tendon area and the medial flare of the tibia as the main areas of support (Fitzlaff and Heim 2002). Also the silicon liner controls the stump volume to a large degree and this can result in a better fit in the socket and improved proprioception. The latter in turn can have a positive effect on performance with the prosthesis.
The silicon liner material has different properties (Emrich and Slater 1998). The silicon sticks to the skin and maintains a vacuum between the stump and the liner. Both qualities have a positive effect on prosthesis suspension. Also abrasion, irritation and skin breakdown is prevented because the liner forms a protective layer between the stump and the socket. Fillauer et al. (1989) and McCurdie et al. (1997) stated that a short stump with a cylindrical or tapering shape was a good indication for liner use in the silicon suction socket (3S) system. Relative contra-indications can be a fluctuating stump volume, hypersensitivity of the stump, considerable scar tissue and bony adhesions, a long stump, excessive distal redundancy and patients unable to handle the system. Wetz et al. (1992) mentioned that deep scar tissue and trophic skin changes i.e. with diabetes the full contact silicon liner is tolerated less well on the stump. Also he mentioned that inadequate stump hygiene poses a contra-indication for use. The conclusions of these authors is based on empirical and not on scientific evidence. In contrast Berman and Flores (1999) and Fulton (1995) both mentioned the positive effects of silicon material on scar tissue. The scar becomes softer and pliable during the use of silicon coverings. The exact mechanism behind this effect remains unclear.
Discussion
The silicon socket liner can have different effects on the amputee. These can be divided in stump-related factors and function or prosthesis related factors. The former includes influences on stump pain and skin while the latter includes walking function, comfort, cosmesis, suspension and donning and doffing of the prosthesis.
There is, however, little clinical evidence to support the positive effects of silicon liner socket use in the trans-tibial prosthesis. The research on the subject is in general of poor quality. The authors found that in the literature the suspension properties of the silicon liner socket were judged to be good however this conclusion is based mostly on patients' opinions rather than on clinical research. The suspension is also dependent on the type of locking mechanism and adequate donning and doffing (Grevsten 1978; Heim et al. 1997; Mak et al. 2001). Narita et al. (1997) examined the suspension properties of the silicon liner socket in one patient with x-ray examination. They showed that the distal tibia moved less in relation to the socket in standing and relaxed position of the stump with the use of the silicon liner compared to the patellar tendon bearing (PTB) system. Also Tanner and Berke (2001) made a comparison of tibial movement in one patient using the ICEROSS liner in a silicon suction socket and the PTB system with a neoprene sleeve. They found, using x-ray examination, that the silicon suction socket resulted in the least movement of the tibia and soft tissue in the socket. Both studies used x-ray examination, but regrettably too few patients were examined to draw substantial conclusions. Fillauer et al. (1989) included a small patient study in a descriptive article about the silicon suction socket (3S) system. They followed 45 patients for a period of 1.5 years and stated that the majority was satisfied with the suspension properties and range of knee motion. Regrettably it is unclear how this data was obtained.
Larsson et al. (1999) mentioned in their treatment protocol for lower limb amputations the postoperative use of silicon liners. In this protocol the liner is used 5–7 days postoperatively. They followed 74 patients 3 months after surgery. The immediate postoperative use resulted in the attainment of a stable stump shape faster and therefore the initial prosthesis could be made sooner. Also the hospital stay was shorter than with the conventional treatment without a liner. Of these patients 59% became walkers and 3% became functional users of a prosthesis defined as using the prosthesis a large part of the day during short walks and making transfers. It is unclear if all these patients used liners in their prosthesis. In a review performed by Cochrane et al. (2001) regarding prosthetic components it was concluded that silicon and polyurethane liners offer an improved suspension but also pose an increased risk of dermatological stump problems especially in active users of the prosthesis, traumatic patients and patients with pre-existing dermatological problems. These problems include folliculitis, allergic reactions, skin maceration and heat rash. Also bunching and wrinkling in the knee was mentioned.
Despite the shortcomings in the studies there is reason to believe that the suspension of the prosthesis is improved with the use of a silicon liner. In the majority of the studies the ICEROSS liner was used in combination with the shuttle lock system so the conclusions can only be drawn for this socket design. Also the cosmesis of the prosthesis was generally judged favourably by the amputee. Skin problems were frequently mentioned by liner users and donning and doffing presented a problem in a number of the patients.
It stands to reason that improved suspension and cosmesis will have a positive effect on prosthetic function and general satisfaction of the amputee (Wirta et al. 1990). In regard to the latter the amputee can have a more positive impression of the prosthesis and thus be more satisfied with other qualities i.e. the appearance. Also complaints of pain and stump discomfort can influence the satisfaction of the amputee on these issues. Because the studies found did not give individual data to this degree a relationship between these factors (function, appearance satisfaction, stump pain and discomfort) could not be found. It is, however highly likely that these factors influence one another and dictate the outcome of the individual studies especially because most data was obtained by asking the patients' opinions using self completed questionnaires. The study group in the individual studies was heterogeneous in relation to co-morbidity, indication for amputation, age and duration of prosthesis use. The indications for amputation varied from various vascular problems, trauma, diabetes, congenital problems and infection. Also the age of the study population varied from 15 to 80 years and prosthetic use ranged from 10 days to 19 years. In these studies most data were obtained using a self completed questionnaire without objective clinical parameters. It is important to realise that in studying non-objective parameters (i.e. pain perception, cosmesis and general satisfaction) with such questionnaires, these can influence one another and give unclear results in research outcome. For this reason the use of objective parameters should be preferred.
To improve the quality of the research on silicon liner use in the trans-tibial prosthesis the authors advise the use of a homogenous patient group in relation to the indication for amputation, co-morbidity, duration of prosthetic use and age. These factors have a large influence on skin quality of the stump as found by Lake et al. (1997). They mentioned for example a decrease in perspiration in older patients. Also the level of activity and duration of prosthetic use play an important role. They stated that dermatological problems such as folliculitis are more often found in active users of the prosthesis.
Conclusion
There is little clinical evidence in the literature to support the positive qualities of the silicon liner socket use in the trans-tibial prosthesis. This is to a large extent related to low quality in study designs. However, there is a good indication to believe that the suspension of the prosthesis is improved when using a liner. Also the walking performance with the prosthesis is positively affected which results in increased walking distance outdoors and less dependence on walking aids. It seems that skin problems are not generally solved by liner use and are sometimes caused by this. Further research with an adequate study design, homogenous population and objective study parameters is needed to show objectively the advantages of silicon liner socket use in the trans-tibial amputees.